
Abstract
Background:
Pain is the most common cancer-related symptom, but it is often undertreated. Telemedicine is widely used in cancer treatment, but its effectiveness is uncertain.
Objective:
We aimed to evaluate the impact of telemedicine intervention on pain in patients with cancer.
Design:
Methodological quality and risk-of-bias evaluation were conducted, and the sources of heterogeneity were explored through subgroup analysis and sensitivity analysis.
Data Sources and Methods:
PubMed, Embase, Web of Science, Cochrane Library, and clinical trial databases were searched up to 16 August 2022. Randomized controlled trials of the impact of telemedicine intervention regarding pain in patients with cancer were included, and the results related to pain were extracted.
Results:
Twenty-one randomized controlled trials were selected from 1810 articles. A total of 1454 patients received telemedicine interventions, and 2213 received conventional medical services. Telemedical intervention had a positive effect on improving pain intensity [standard mean deviation (SMD) = −0.28, 95% confidence interval (CI): −0.49 to −0.06, p = 0.01] and pain interference (SMD = −0.41, 95% CI: −0.54 to −0.28, p < 0.00001), with statistical difference between the two groups. The subgroup analysis results showed that the telemedicine subgroup based on an application (SMD = −0.54, 95% CI: −0.91 to −0.18, p = 0.004) and the subgroup with intervention time ⩾ 6 months (SMD = −0.33, 95% CI: −0.52 to −0.13, p = 0.001), both demonstrated significant improvement regarding pain intensity, with significant statistical difference between the two groups. When the follow-up time was ⩾ 6 months, there was no significant difference (SMD = −0.24, 95% CI: −0.55 to 0.07, p = 0.13).
Conclusion:
Compared with conventional medical services, telemedicine intervention can improve the pain of patients with cancer and is effective and acceptable regarding symptom monitoring. Integrating telemedicine interventions into cancer pain management may be a feasible option. But its long-term effects still need to be confirmed with more high-quality randomized controlled trials in the future.
Registration:
https://www.crd.york.ac.uk/PROSPERO/; CRD42022361990
Introduction
Pain has been defined as the fifth vital sign, and it is one of the most common and difficult symptoms faced by patients with cancer. 1 The prevalence of cancer pain is very high,2,3 and more than one-third of patients with cancer will experience moderate to severe pain. 4 However, research shows that nearly 50% of cancer pain are not appropriately treated, with inadequate cancer pain management.5–7 Uncontrolled pain will interfere with daily life, impair patients’ health-related quality of life (HRQOL), increase anxiety and depression, hinder cancer recovery, and increase emergency medical services. 8 Especially for remote patients who already left the hospital and have less access to medical care,9,10 face-to-face pain treatment faces many challenges,11–13 including physical burden, transportation distance, money and time cost, shortage of medical resources, energy of caregivers, and so on. Therefore, how to timely and effectively monitor and evaluate pain symptoms, and how to achieve good dynamic pain management in daily practice are urgent public health problems that need to be solved.
Telehealth is defined as the use of technology to promote remote health care, health education, public health, and health management. The term telemedicine first originated in 1977. 14 It is a subset of telehealth. It refers to the provision of remote clinical services for patients and/or informal nurses through information and communication technologies.15,16 Due to its relatively low cost, large-scale target population, more convenient access, and personalized services, it has been widely used in pain management. 17 Telephone follow-ups, automatic symptom monitoring systems, and online consultation have strengthened the communication between patients and health professionals.18–20 Multimodal nursing based on mobile Internet is superior to conventional nursing, and it innovatively solved the problem of distance in nursing service. 21 Oldenmenge et al. realized online communication between patients and nurses through pain diaries, eConsult, patient pain education, and other Internet applications, and achieved good pain management. 10 Through a mobile application called Pain Guard, pharmacists can regularly educate patients about pain, give them guidance about the use of different drugs, improve drug compliance, strengthen pain management, thus improving their quality of life. 22 Mobile Pain Coping Skills Training (mPCST) allows therapists in medical centers to provide patients with pain management through video conference, which also demonstrates a highly accessible, feasible and acceptable prospect.
These studies seemed to have shown a positive side. When cancer pain becomes difficult to manage, telemedicine intervention may have potential advantages, and it is an important supplement to cancer pain management programs. There are few meta-analyses on the effectiveness of telemedicine in supporting cancer pain at the moment, and there is a lack of evidence. Therefore, we conducted this meta-analysis study to test the feasibility, acceptability, and initial efficacy of telemedicine intervention for pain relief in patients with cancer. To our knowledge, this is the first meta-analysis to study telemedicine in terms of intervention type, delivery mode, intervention, or follow-up time.
Materials and methods
Search strategy
The present study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and has been registered in Prospero in advance (https://www.crd.york.ac.uk/PROSPERO/; CRD42022361990). PubMed, Embase, Web of Science, Cochrane Library, and Clinical Trials were searched. The time limit for the search was set from 1977 to 16 August 2022. Only articles published in English were included. The subject terms Telemedicine, Neoplasms, and Pain as well as free terms related to these subject terms were used for retrieval. For specific retrieval strategies, see the supplementary materials. We reviewed the list of references of all major studies, as well as the references of other review articles. When duplicate publications of the same trial were found, the most complete, recent, and updated version was included.
Inclusion and exclusion criteria
The studies meeting the following criteria were included in the analysis: (1) the participants were patients with cancer, including all tumor types and disease stages, without age limit; (2) intervention measures were any form of telemedicine (including but not limited to telephone, video, mobile application, or Internet-based nursing) for cancer symptom monitoring and management; (3) the control group was provided with some conventional medical services without any form of telemedicine intervention; (4) the main outcomes were pain intensity and pain interference; (5) randomized controlled trial limited to English only.
Exclusion criteria were as follows: (1) review, meta-analysis, commentary, consensus, conference summary, animal experiment, case report, letter, and so on; (2) systematic design models and research protocols were not published, and studies that only provided test data (which did not involve real data of the patients); (3) there were no outcome indicators regarding pain, or studies with data that could not be extracted.
The screening, evaluation, data extraction, and quality evaluation were all conducted independently by two authors, and the results were compared. If any disagreement arose, the issue was resolved through discussion with a third author.
Data extraction
We extracted the following characteristic information from each study: study author, publication year, country, participants (sample size, cancer type), intervention measures, control measures, pain measurement methods, remote delivery method, outcomes (pain intensity, pain interference) and design (study design, intervention time, follow-up time). If these data were not reported in the original article, we proceeded to extract them from the accompanying charts or ClinicalTrials.gov.
Quality assessment
We used the Cochrane risk-of-bias tool to assess the bias risk of each study. The quality and bias risk of each included study were evaluated from the perspectives of allocation sequence generation, concealment of allocation, blinding of participants and investigators, incomplete outcome data, selective outcome reporting, and other sources of bias. Each field was rated as low risk of bias, high risk of bias, or unclear risk of bias.
Data analysis
We used the Review Manager software (version 5.4) for statistical analysis. Because different studies had different methods for measuring the results, we used the standard mean deviation (SMD) and the corresponding 95% confidence interval (CI) as the effect measure of the outcomes. Statistical heterogeneity was evaluated by Q test and I2 statistics. If the I2 value was greater than 50%, the heterogeneity was considered significant, and the random effects model was used. Otherwise, the fixed effects model was used. The type of telemedicine intervention, delivery mode, intervention time, and follow-up time were analyzed by subgroup analysis. The sources of heterogeneity were analyzed by subgroup analysis and sensitivity analysis. A p value < 0.05 indicates that the difference is statistically significant.
Results
Study selection
A total of 1810 articles were retrieved, including 2 studies that were manually retrieved. 567 repetitive articles were deleted, and 122 articles were included in the preliminary screening. After reading the full texts, 21 studies were included in the final analysis.18,19,21,23–40 See Figure 1 for the flowchart of the detailed screening process.

Flowchart of the screening process.
Study and patient characteristics
In the included studies, a total of 1454 patients received telemedicine intervention and 2213 received conventional medical services. Among all the interventions used in the studies, eight were based on web, five were based on telephone, five were based on applications, and three were based on video conferences. The studies included a variety of pain assessment methods, Brief Pain Inventory (BPI) pain score being the main one. Specific intervention and control measures, intervention and follow-up time, as well as pain assessment methods are shown in Table 1.
Characteristics of included studies.

BPI, Brief Pain Inventory; EORTC, the European Organization for Research and Treatment of Cancer; FACT-By 4.0, Functional Assessment of Cancer Therapy-Breast version 4.0; PROMIS, Patient Reported Outcomes Measurement Information System; QOL, quality of life; QOL-C30, Quality of Life Questionnaire-Core 30; RCT, randomized controlled trial; SF-36v2, Short Form-36.
Quality assessment
According to the Cochrane instrument, the risk of bias of most studies was considered to be low. Of the 21 studies, 13 reported details regarding randomization protocols, and 7 reported allocation concealment, which were considered to have a low risk of selection bias. Eight studies had a pretty high risk regarding the blinding of the participants and researchers, while 10 studies had no mention and were considered to have unclear risk. In terms of measurement bias, nine studies were considered low risk, nine studies were without mention, and three studies were high risk. In terms of follow-up bias, reporting bias, and other biases, most studies were evaluated as low risk. The methodological quality assessment results of the included studies are shown in Figures 2 and 3. By eliminating each study, the recalculated combined effect size had no significant change, indicating that there was no outlier study that significantly affected the overall results.

Risk of bias summary.

Risk of bias graph.
Effects on pain intensity
All studies have reported on the effectiveness of telemedicine interventions on the intensity of pain in patients with cancer. The heterogeneity test showed that there was significant heterogeneity among the studies (I2 = 83%, p < 0.00001); therefore, the random effects model was used. The summary of the results showed that telemedicine intervention can significantly improve the pain intensity of patients with cancer, with statistical significance (SMD = −0.28, 95% CI: −0.49 to −0.06, p = 0.01; Figure 4).

Effects of different telemedicine intervention types on cancer pain intensity meta-analysis forest plot.
Effects on pain interference
Six trials evaluated the impact of telemedicine interventions on pain interference in cancer survivors. Heterogeneity test showed that there was moderate heterogeneity among the studies (I2 = 49%, p = 0.08); therefore, the fixed effects model was used. The analysis results showed that telemedicine intervention can significantly improve the pain interference of cancer survivors, with significant statistical significance (SMD = −0.41, 95% CI: −0.54 to −0.28, p < 0.00001, Figure 5).

Effects of telemedicine intervention on cancer pain interference meta-analysis forest plot.
Subgroup analysis
We conducted subgroup analysis on the different types of telemedicine interventions and found that the application-based telemedicine subgroup had more advantages regarding effectiveness in improving pain intensity (SMD = −0.54, 95% CI: −0.91 to −0.18, p = 0.004, Figure 4). In contrast, there was no significant difference between the two groups in the subgroup analysis based on web pages (SMD = −0.14, 95% CI: −0.37 to 0.10, p = 0.25), telephone (SMD = −0.13, 95% CI: −0.51 to 0.25, p = 0.51) and video conferences (SMD = −0.29, 95% CI: −1.69 to 1.10, p = 0.68) (Figure 4). In the subgroup analysis of interaction mode, it was found that there was no significant statistical difference between the synchronous (SMD = −0.40, 95% CI: −0.85 to 0.05, p = 0.08) and the asynchronous (SMD = −0.17, 95% CI: −0.36 to 0.03, p = 0.09) subgroups (Figure 6).

Effects of different interaction modes of telemedicine interventions on cancer pain intensity meta-analysis forest plot.
Subgroup analysis for the telemedicine intervention time was conducted, and it was found that in the two subgroups with an intervention time of < 3 months (SMD = −0.53, 95% CI: −0.97 to −0.09, p = 0.02, Figure 7(a)) and ⩾ 6 months (SMD = −0.33, 95% CI: −0.52 to −0.13, p = 0.001, Figure 7(b)), results regarding the improvement of pain intensity in patients with cancer were shown, and they were statistically significant. There was no significant difference between the two subgroups with an intervention time of ⩾ 3 months (SMD = −0.11, 95% CI: −0.29 to 0.08, p = 0.27, Figure 7(a)) and < 6 months (SMD = −0.26, 95% CI: −0.51 to 0.00, p = 0.05, Figure 7(b)).

Effect of telemedicine intervention duration (a) (time ⩾3 months and time < 3 months) and (b) (time ⩾ 6 months and time <6 months) on cancer pain intensity meta-analysis forest plot.
We also conducted a subgroup analysis for the follow-up time and found that compared with the subgroup of < 3 months (SMD = −0.25, 95% CI: −0.77 to 0.28, p = 0.36, Figure 8(a)), when the follow-up time was ⩾ 3 months (SMD = −0.28, 95% CI: −0.53 to −0.04, p = 0.02, Figure 8(a)), results in improving the intensity of pain in patients with cancer were shown, and they were statistically significant. However, no significant statistical difference was found between the two subgroups with a follow-up time of ⩾ 6 months (SMD = −0.24, 95% CI: −0.55 to 0.07, p = 0.13, Figure 8(b)) and < 6 months (SMD = −0.28, 95% CI: −0.57 to 0.01, p = 0.06, Figure 8(b)).
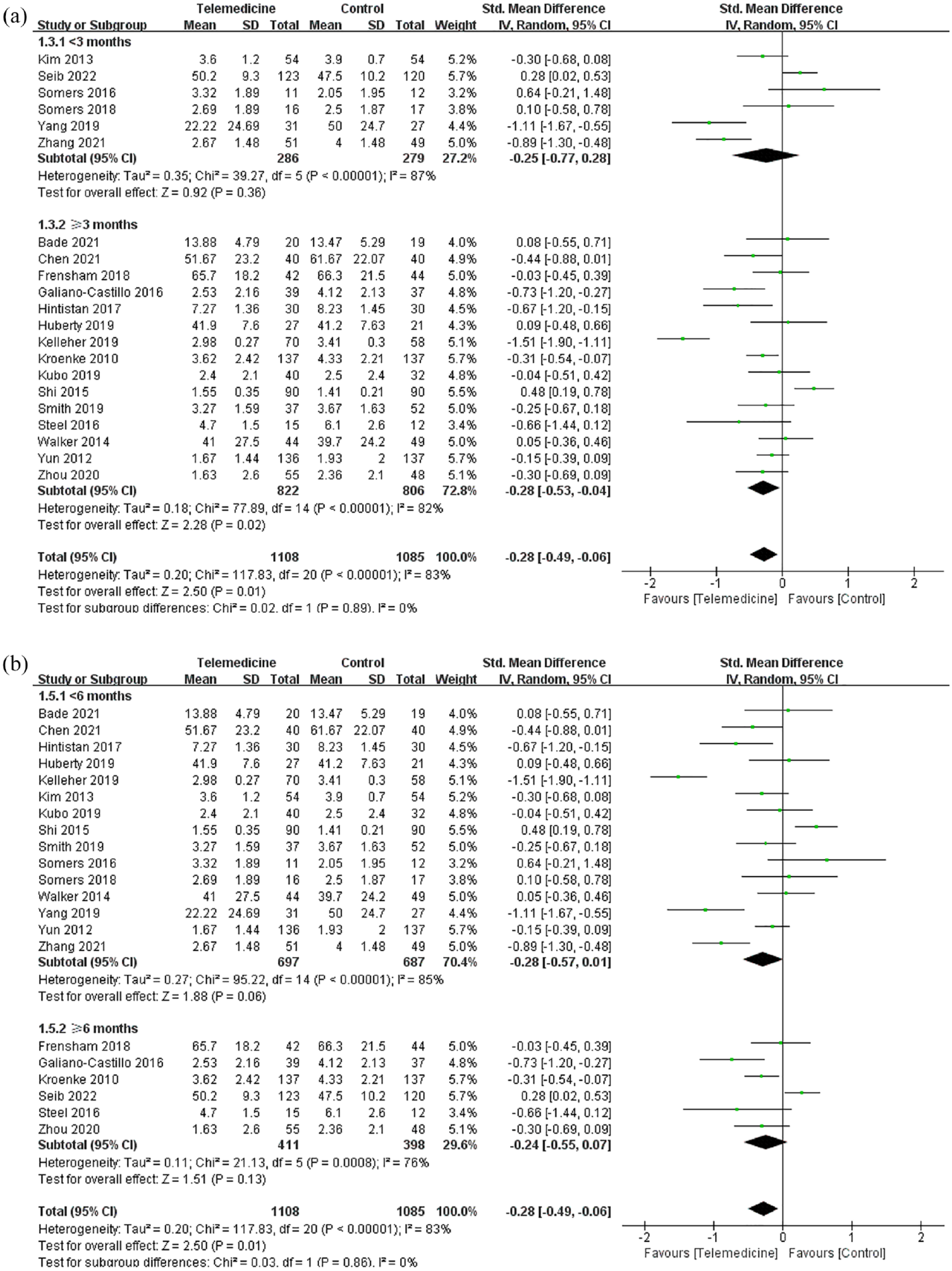
Effect of telemedicine follow-up duration (a) (time ⩾3 months and time < 3 months) (b) (time ⩾6 months and time< 6 months) on cancer pain intensity meta-analysis forest plot.
Discussion
Pain is the most common and treatable cancer-related symptom, but it is often unrecognized or undertreated. Therefore, it is necessary to explore effective, low-cost, and convenient pain interventions to meet the needs of patients and medical personnel. The outbreak of COVID-19 has brought obstacles to the traditional face-to-face medical services. The remote, noncontact way of telemedicine has unique opportunities and challenges. 41 However, the effectiveness of telemedicine for cancer pain is still unknown. Although the meta-analysis from Buonanno et al. showed that telemedicine has advantages regarding the reduction of cancer pain, and can ensure high-quality assistance similar to traditional medicine, there is little difference between the two. 42 Also, the number of studies included in their study was small, and the accessibility and acceptability of telemedicine were not discussed from the aspects of intervention type and delivery mode. In this present study, we aimed to evaluate the effectiveness and difference of different modes of telemedicine intervention in cancer pain management. This is an important supplement to the formulation of cancer pain management plans and the selection of telemedicine modes in the future.
Compared with traditional medicine, telemedicine is no longer limited by space, time, and other obstacles, increasing the opportunities for patients with cancer to obtain medical services. The overall satisfaction rate from the patients is also pretty high. 43 Using telemedicine technology can effectively and timely monitor and manage pain symptoms and make up for the communication gap found with traditional medicine. Multimodal nursing based on mobile Internet can better achieve good pain management through online connection between patients and nurses. This kind of nursing is more accessible than conventional nursing.10,21,44 Collaboration between the joint team of doctors, nurses, and pharmacists has strengthened the communication and collaboration between medical personnel and patients, and improved the management of cancer pain symptoms.21,32,33 Similar to these research results, our study found that, compared with conventional medical services, telemedicine intervention is beneficial in improving the pain intensity and pain interference of patients with cancer. Although the difference between the two groups was statistically significant, the clinical effect of this improvement was not very remarkable and was not considered to be clinically relevant. The heterogeneity was relatively high in our study. Therefore, we conducted subgroup analyses to explore some potential factors affecting the intervention effect.
With the popularization and wide coverage of mobile Internet access, mobile medical services based on mobile phone applications have attracted more and more attention. The study by Yang et al. confirmed that better results can often be obtained by using mobile pain applications for intervention. 33 The use of the WeChat-based MediHK and multimodal nursing softwares to conduct pain intervention21,32 also resulted in good feedback. A mobile app called Pain Guard also helps pharmacists to better deliver pain management. 22 However, in the early researches, technologies based on telephones and web pages were mostly used because of their wide accessibility and familiarity.19,34,45 In previous literature, researches regarding the different intervention types of telemedicine were also lacking. Whether there are differences in effectiveness regarding pain symptom management between the different kinds of interventions, is an issue discussed in our study. Our research found that the telemedicine intervention mode based on mobile phone APP has obvious advantages in managing the pain symptoms of tumor patients. We believe that this is closely related to the advantages of telemedicine, such as being free from time and space, convenient, low cost, and rapid to respond to patients’ needs. This may indicate that using mobile technologies to develop remote applications could enhance the accessibility of cancer pain management, which holds certain prospect in the future cancer research field.
Health care providers, by being able to stay updated about the pain status of tumor patients in time, can decide whether to change their pain treatment plan. Therefore, whether telemedicine intervention can provide real-time message transmission, and whether patients’ needs regarding pain can be responded in time, play an important role in cancer pain management. Synchronization technology is provided through real-time interaction between healthcare providers and patients, which includes video conferences, phone calls, or web-based real-time chat. mPCST showed to be highly feasible for the therapists in medical centers to provide cancer pain management for patients with cancer through video conference. Asynchronous technology refers to an automatic message storage, or delivery system, without real-time interactive components. No research on this aspect was conducted in the previous literature. Although our study did not show the difference between these two different interaction modes when it comes to cancer pain management, we still think that with the widespread use of mobile applications, the development of user-friendly, intuitive and real-time interactive applications, the dynamic management efficiency of cancer pain may be improved. Of course, this needs to be further verified by more randomized controlled trials with longer follow-up periods in the future.
In addition, our research found that with the extension of telemedicine intervention time, the effectiveness of intervention becomes more obvious. Compared with 3 months, when the intervention time reached 6 months, the effectiveness of telemedicine on cancer pain control was more prominent. This is also consistent with the research results from Buonanno et al. We suspect that the longer the duration of telemedicine intervention, the greater the impact on patients’ behavior change and treatment compliance, which are often important factors affecting pain management. In the studies we included, some of the results were obtained through follow-ups after the interventions had stopped. The study from Kelleher et al. showed that the self-efficacy of pain management in the 4 weeks mPCST group continued to increase, and the long-term impact was greater, while that in the traditional PCST group decreased. 28 Seib’s research also supported the view that the effect could last within the follow-up period. 35 However, Galiano Castillo et al. found that, although the telemedicine intervention lasting for 8 weeks could significantly improve the severity of pain after the intervention ended, the effectiveness was not maintained at the 6-month follow-up. 26 Our study also found that the effect of telemedicine intervention on cancer pain control did not last effectively at 6-month follow-up when compared with 3 months. Therefore, how long of telemedicine intervention can achieve optimal efficacy and sustained effect through the follow-up period? This still needs to be further studied in the future, with more large sample randomized controlled trials with longer follow-up periods.
In addition, chronic pain experienced by cancer survivors is related to other problematic symptoms, such as depression and fatigue. 46 Pain can cause these symptoms, and these symptoms can also cause pain, thus affecting the quality of life. However, the studies we have included lack data in this area. Only Walker et al. reported some research results on cancer pain combined with depression in patients with cancer, 45 which require more study data to support and demonstrate in the future.
There are some limitations to this study. (1) The number of selected studies and participants was small, and recent clinical researches are still in progress. (2) Due to the nature of electronic health interventions, most studies lacked the use of blinding for participants and evaluators. (3) In terms of technical media, pain assessment methods, intervention, and follow-up durations, there were great differences between the different studies. Important heterogeneity was also present. Therefore, validation from more large sample studies in the future is still needed.
Conclusion
In summary, telemedicine interventions can improve the pain control of patients with cancer, which is beneficial in cancer symptom management. When cancer pain becomes difficult to manage, telemedicine intervention may have potential advantages and could be an important supplement to cancer pain management programs. Its long-term effects still need to be further confirmed by more high-quality randomized controlled trials in the future.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231153097 – Supplemental material for The efficacy of telemedicine for pain management in patients with cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-1-taj-10.1177_20406223231153097 for The efficacy of telemedicine for pain management in patients with cancer: a systematic review and meta-analysis by Wenyu Chen, Jie Huang, Zhifang Cui, Lei Wang, Liang Dong, Weifeng Ying and Ye Zhang in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.