
Abstract
Objective
The efficacy of ultrasound-guided stellate ganglion block (SGB) in alleviating postoperative pain remains unclear. This meta-analysis was performed to determine the efficacy of ultrasound-guided SGB in relieving acute postoperative pain in patients undergoing surgery with general anesthesia.
Methods
This systematic review and meta-analysis focused on randomized controlled trials comparing SGB with control or placebo. The primary outcome was the pain score at 24 hours after surgery. A random-effects model was used to calculate the mean difference (MD) or risk ratio with a confidence interval (CI) of 95%.
Results
Eight studies involving 470 patients were included in the meta-analysis. The results revealed that ultrasound-guided SGB was significantly associated with a lower pain score at 24 hours after surgery (MD = −0.74; 95% CI = −1.39, −0.08; I2 = 86%; low evidence) and at 8 hours after surgery (MD = −0.65; 95% CI = −1.03, −0.28; I2 = 29%; moderate evidence).
Conclusion
Ultrasound-guided SGB is effective in alleviating acute postoperative pain. However, considering the limited number of trials performed to date, more large-scale and high-quality randomized controlled trials are required to confirm these findings.
Keywords
Introduction
Acute postoperative pain is one of the most common complaints after surgery, with nearly 50% of patients experiencing moderate to severe pain within the first 24 hours postoperatively.1,2 Inadequate management of postoperative pain may increase the risk of autonomic instability, poor mobilization, chronic pain, and a longer hospital stay.3,4
Traditionally, opioids have been used as the primary pharmacological treatment for postoperative pain, although high doses of opioids can lead to postoperative nausea and vomiting, pruritus, and respiratory depression. 5 Multimodal analgesia techniques, such as regional nerve blocks and intravenous patient-controlled analgesia (PCA), have been proven effective in minimizing the stress response, pain intensity, and opioid consumption.
The stellate ganglion, also referred to as the cervicothoracic ganglion, is a sympathetic ganglion formed upon fusion of the inferior cervical ganglion with the first thoracic ganglion. 6 The stellate ganglion delivers sympathetic innervation to the upper extremities, head, neck, and heart. 7 Ultrasound-guided stellate ganglion block (SGB) is used to treat chronic neuropathic pain of the upper extremity, complex regional pain syndrome, and postherpetic neuralgia.8–10 However, the efficacy of ultrasound-guided SGB in relieving acute postoperative pain remains uncertain because of conflicting study results.11–17 In this context, the present meta-analysis was conducted to evaluate the efficacy of ultrasound-guided SGB in relieving acute postoperative pain after surgery under general anesthesia. The study hypothesis was that ultrasound-guided SGB can effectively alleviate acute postoperative pain.
Methods
This meta-analysis was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions 18 and the updated PRISMA 2020 statement guideline. 19 The study was prospective in nature and registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY202350022).
Literature search and participant selection criteria
PubMed, the Cochrane Library, and EMBASE were searched from their respective dates of inception until 6 April 2023, with the language restricted to English. The following queries were used in the PubMed search: (stellate ganglion OR cervicothoracic ganglion OR cervicothoracic ganglia OR stellate ganglia) AND (pain OR analgesia). The reference lists of the retrieved articles were also examined to identify other potentially eligible trials for inclusion.
Trials fulfilling the following criteria were included in the study: (1) population: adult patients undergoing surgery under general anesthesia, (2) intervention: ultrasound-guided SGB prior to surgery, (3) comparison: control or placebo, (4) design: randomized controlled trial (RCT), and (5) outcomes: acute pain score after surgery (visual analogue scale or numerical rating scale). The primary outcome used in the meta-analysis was the pain score at 24 hours after surgery. The secondary outcomes were acute postoperative pain at other time points (0, 2, 4, 6, 8, and 12 hours after surgery) and postoperative nausea and vomiting.
Data extraction and quality assessment
The data were extracted by Yan Zhao and confirmed by Xiangli Xiao. The following extracted data were systematically recorded and arranged in a pre-existing Excel spreadsheet: first author, year of publication, population, number of patients, American Society of Anesthesiologists physical status, surgical procedure, intervention (specific type and concentration of local anesthetic, vertebral puncture), comparison, and outcomes. For reports with only graphical data, the GetData Graph Digitizer was employed to interpolate the data. 20 The median and interquartile range were approximated to the mean and respective standard deviation using the following formula: median = mean and standard deviation = quartile distance/1.35. 21
The methodological quality of the trials included in the present meta-analysis was assessed using a risk-of-bias table. 22 Each item in the table was categorized as having a low, unclear, or high risk of bias based on sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other potential sources of bias.
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool was used to evaluate the certainty of the main results of all included studies. 23 The evidence quality was classified as very low, low, moderate, or high based on the following factors: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Any uncertainty that emerged was resolved by consensus.
Statistical analysis
The mean difference (MD) with 95% confidence interval (CI) was estimated for continuous outcomes, and the relative risk with 95% CI was estimated for dichotomous outcomes. A random-effects model was adopted to obtain the most conservative effects estimate. The Cochrane Q test and I2 statistic were adopted to calculate the heterogeneity across the included trials, and p < 0.1 or I2 > 50% indicated significant heterogeneity.24,25 Further, subgroup analyses involving stratification based on the surgical procedure were performed to evaluate the robustness of the results. Publication bias was assessed using funnel plots and Begg’s and Egger’s tests.26,27 Review Manager Version 5.4 (Nordic Cochrane Centre, Copenhagen, Denmark) and Stata Version 12.0 (StataCorp LLC, College Station, TX, USA) were employed to perform the meta-analyses, considering p < 0.05 to be statistically significant.
Results
Study identification and characteristics
In total, 2021 articles were retrieved in the initial comprehensive search. Among these articles, 1182 were excluded because of duplication and 496 were excluded after screening the titles and abstracts. Finally, seven RCTs fulfilling all the inclusion criteria were retained for the meta-analysis.11–17 The entire selection process is illustrated in Figure 1.

PRISMA flow diagram of study selection. RCT, randomized controlled trial.
The trials included in the present study were published between the years 2004 and 2022, and their sample sizes ranged from 30 to 90. The trials investigated the effects of SGB in patients who underwent various kinds of surgeries: breast surgeries in three studies,15–17 abdominal surgeries in two studies,13,14 and upper limb and thoracoscopic surgeries in the remaining studies.11,12 Five studies compared SGB with placebo,11,13,14,17,18 and two studies compared SGB with multimodal systemic analgesia or PCA.12,15 Two studies used lidocaine for SGB,11,14 two studies used bupivacaine,12,15 and three studies used ropivacaine.13,16,17 The concentration of the local anesthetic drugs differed across the included studies. The characteristics of the RCTs included in the present study are summarized in Table 1.
Characteristics of included studies.

ASA, American society of Anesthesiologists; PCA, patient-controlled analgesia; PONV, postoperative nausea and vomiting; NA, not reported.
Acute postoperative pain scores
Pain score at 24 hours after surgery
As presented in Figure 2, all seven studies reported the postoperative pain scores.11–17 Ultrasound-guided SGB was associated with a lower pain score at 24 hours after surgery (MD = −0.74; 95% CI = −1.39, −0.08; p = 0.03; I2 = 86%). The subgroup analysis (Figure 3) indicated that the use of ultrasound-guided SGB alone reduced postoperative pain in abdominal surgeries (MD = −1.42; 95% CI = −2.21, −0.63; p = 0.009; I2 = 63%) and breast surgeries (MD = −1.31; 95% CI = −2.31, −0.31; p = 0.01; I2 = 72%). Among patients who underwent upper limb and thoracoscopic surgeries, the postoperative pain scores were not lower in the SGB group.

Forest plot of pain score at 24 hours after surgery. SD, standard deviation; CI, confidence interval; SGB, stellate ganglion block.
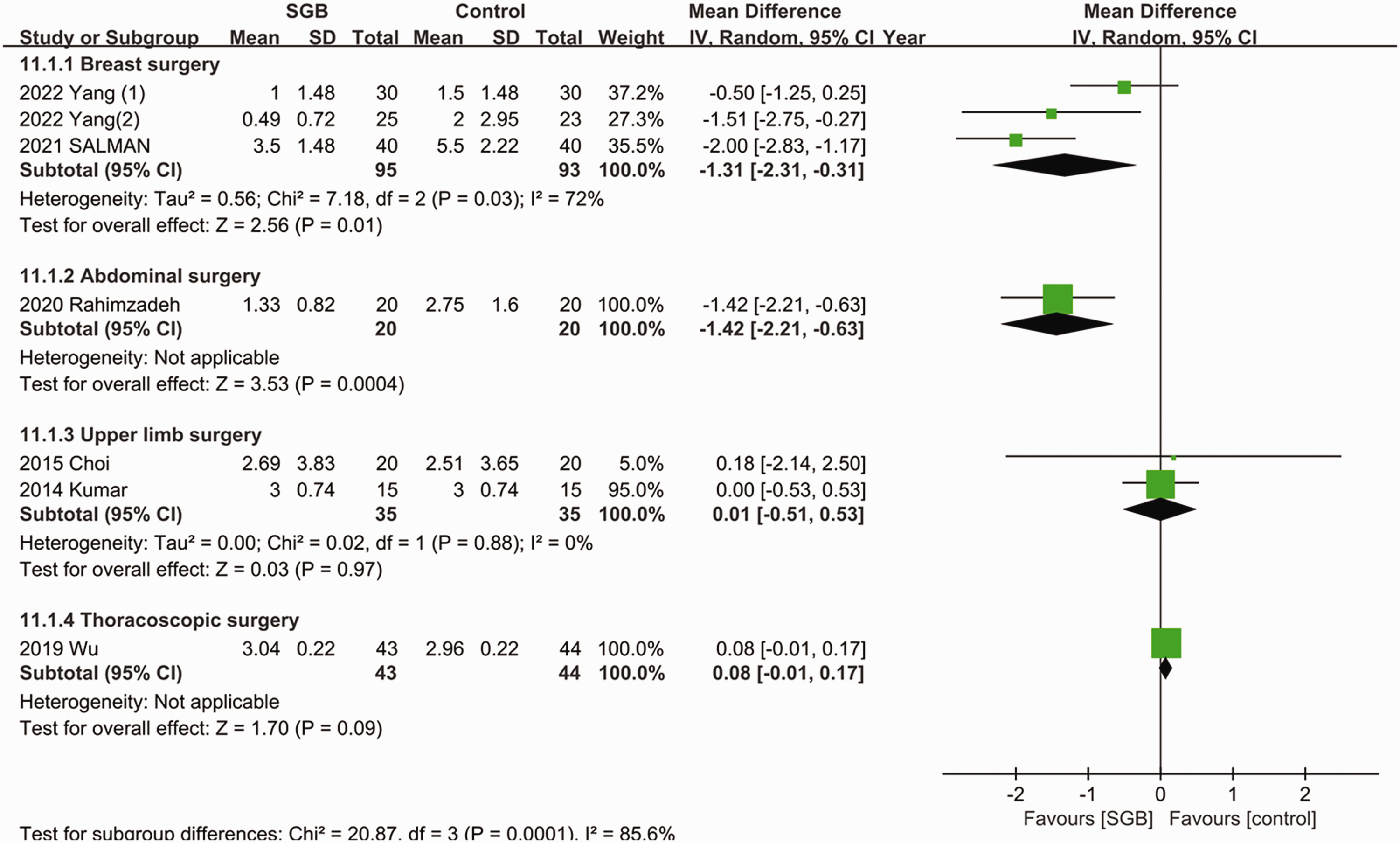
Forest plot for subgroup analysis of pain score at 24 hours after surgery. SD, standard deviation; CI, confidence interval; SGB, stellate ganglion block.
Pain score at other time points after surgery
No difference in pain scores was noted between the SGB group and the control group at 0, 2, 4, 6, and 12 hours after surgery, although a trend toward lower pain scores was observed at 2 hours after surgery (MD = −0.22; 95% CI = −0.54, 0.11) and 6 hours after surgery (MD = −0.54; 95% CI = −0.19, 0.12) (Supplementary Figures 1 and 2). Ultrasound-guided SGB was associated with a lower pain score at 8 hours after surgery (MD = −0.65; 95% CI = −1.03, −0.28; p = 0.01) without significant heterogeneity (I2 = 29%).
Quality assessment and publication bias
The quality assessment results revealed an unclear risk of bias for four of the included studies 11,12,14,15 and a low risk of bias for three studies.13,16,17 The risk-of-bias assessment results are summarized in Figure 4. Table 2 provides an overview of the level of certainty for the primary findings. The level of evidence of all studies evaluated using the GRADE tool was classified as very low to moderate. Specifically, the pain scores at 0, 12, and 24 hours after surgery were categorized as low, while the pain scores at 8 hours after surgery were classified as moderate.

Risk-of-bias summary.
GRADE profile.

Some of the included trials had an unclear risk of bias.
Heterogeneity across trials was observed.
The included trials had wide 95% CIs.
CI, confidence interval; MD, mean difference; RCT, randomized controlled trial; GRADE, Grading of Recommendations, Assessment, Development, and Evaluation.
No publication bias was detected by visual inspection of the funnel plots or by the formal statistical tests (Begg’s test and Egger’s test) (Supplementary Figures 3 and 4).
Discussion
The present meta-analysis indicated, with a moderate to low level of certainty, that ultrasound-guided SGB is associated with alleviation of acute postoperative pain at 8 and 24 hours after surgery.
Previous studies have indicated that ultrasound-guided SGB reduces the intensity of pain by inhibiting the sympathetic nervous system.8,28 Sympathetic excitation may lead to catecholamine release and exacerbate the inflammatory response during the perioperative period. 29 Inflammation and sympathetic nervous system activation are critical contributors to postoperative pain. 30 According to recent theories, the pain relief experienced upon ultrasound-guided SGB is linked to the regulation of nerve growth factor (NGF), which plays a crucial role in several signaling pathways associated with acute stress. 31 In addition, NGF activates sympathetic nerves and increases the release of norepinephrine, which promotes sensitization of the peripheral nociceptors and increases the perception of pain. 32 Ultrasound-guided SGB blocks the injurious afferent sympathetic pathways, thereby effectively reducing the NGF level and decreasing sympathetic activity, resulting in pain reduction. 33
Several previous studies showed that ultrasound-guided SGB was associated with reduced postoperative pain scores in patients undergoing upper limb surgery.11,30,34 However, Choi et al. 12 indicated that ultrasound-guided SGB was not associated with a reduction of the postoperative pain score at any time point after arthroscopic shoulder surgery. One possible explanation for this is that the intensity of pain experienced during arthroscopic shoulder surgery is not as high as that experienced after open upper limb surgery. In addition, tramadol was administered intravenously when the patients’ visual analogue scale score was >4, 12 which might have interfered with the postoperative pain score to a certain extent, and minor differences might not have been detected in the small patient population. Similarly, in another study included in the present meta-analysis (the study by Wu et al. 13 ), ultrasound-guided SGB did not reduce the acute postoperative pain score in patients undergoing thoracoscopic surgery. This might have occurred because the small incisions used in thoracoscopic surgery and the routine use of PCA after the surgery decreased the difference in the pain scores between the SGB group and the control group.
Postoperative pain alleviation is of great concern to clinicians. In the present study, therefore, we sought to provide further useful information to clinicians in their attempts to improve the surgical and anesthetic techniques used for postoperative pain relief. Ultrasound-guided SGB is superior to traditional nerve blocks because it does not produce motor or sensory blockade, thereby enabling the surgeon to assess the motor function immediately after surgery. 11 A small amount of injectate is sufficient for a successful block. According to a previous study, 4 mL of 0.2% ropivacaine used in ultrasound-guided SGB was effective in maintaining good analgesia. 35 All studies included in the present meta-analysis used low-dose local anesthetics, and no local anesthetic toxicity was recorded. However, anatomic variation and incorrect identification of relevant structures can lead to failure of the block. 36 Moreover, the stellate ganglion is situated close to the inferior thyroid artery, carotid artery, and vertebral artery, necessitating vigilance on the part of clinicians to avoid intravascular injection and post-pharyngeal hematoma. 37 However, these complications were not reported in the studies included in the present meta-analysis. In addition, enhancing clinicians’ proficiency is crucial to minimizing errors and complications during the ultrasound-guided SGB procedure. Whether SGB can replace or serve as an adjunct to certain traditional nerve blocks, such as the brachial plexus block, is a valuable focus of further research. Although a few studies have addressed this question, it seems unlikely that SGB can entirely supplant the brachial plexus block. This is because the efficacy of SGB in alleviating postoperative pain through sympathetic nerve blockade may be limited. Our meta-analysis suggests that SGB may only reduce postoperative pain in some surgeries. Because of the limited number of studies and their small sample sizes, future high-quality research is needed to better understand the role of SGB in various surgical settings.
To the best of our knowledge, the present meta-analysis is the first to evaluate the efficacy of ultrasound-guided SGB in relieving acute postoperative pain. The meta-analysis was conducted strictly in accordance with the Cochrane Handbook and the PRISMA statement. However, a few limitations must be noted. First, significant heterogeneity was detected across the included studies. This heterogeneity can be attributed to the different surgeries performed and the diverse types, concentrations, and dosages of local anesthetics used in these studies. The differences in the surgical duration and the proficiency of the SGB procedure could also have contributed to the heterogeneity. Second, although our analysis showed statistically significant reductions in pain scores at 24 hours after surgery, the mean difference was small. Considering the small sample size in most of the trials included in the present meta-analysis, the findings of the present study must be interpreted with caution. Further large-scale and high-quality research is needed to confirm the analgesic effect of SGB. Third, the GRADE analysis revealed that most outcomes had a very low to moderate level of evidence, and the risk-of-bias analysis showed that more than half of the included studies had unclear risk. Finally, the effect of ultrasound-guided SGB in terms of reducing the consumption of opioids and the safety of using SGB were not evaluated in the present meta-analysis because of the unavailability of sufficient relevant data across the included studies.
Conclusion
Ultrasound-guided SGB is effective in alleviating acute postoperative pain. However, considering the low evidence of outcomes and limited number of trials, more studies are warranted to definitively determine the analgesic effect of ultrasound-guided SGB on patients undergoing surgery under general anesthesia.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241252237 - Supplemental material for Efficacy of ultrasound-guided stellate ganglion block in relieving acute postoperative pain: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241252237 for Efficacy of ultrasound-guided stellate ganglion block in relieving acute postoperative pain: a systematic review and meta-analysis by Yan Zhao and Xiangli Xiao in Journal of International Medical Research
Footnotes
Authors’ contributions
YZ: Study conception and design, data acquisition and analysis, drafting of the article, and critical revision of the article for important intellectual content;
XX: Study conception and design, data analysis and confirmation, and revision of the article.
Availability of data and materials
All data relevant to the study are included in the article or have been uploaded as supplementary information.
Consent for publication
Consent for publication was not applicable because of the nature of this study (systematic review and meta-analysis).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
Ethics approval and consent to participate were not applicable because of the nature of this study (systematic review and meta-analysis).
Funding
The study was supported by the Beihai City Science and Technology Planning Project (201995060).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.