
Abstract
Objectives:
To explore the optical coherence tomography (OCT) biomarkers to predict the transition to chronic central serous chorioretinopathy (cCSC) after retinal laser photocoagulation.
Methods:
Patients enrolled in this study were from a 12-week clinical trial comparing the efficacy and safety of subthreshold micropulse laser (SML) with threshold conventional laser (TCL) for CSC and had extended follow-up for more than 1 year. They were divided into two groups, transited to cCSC group (cCSC group) and did not transited to cCSC group (non-cCSC group) according to fundus examination at the extended follow-up. Collect the best-corrected visual acuity (BCVA) and OCT characteristics of patients at baseline and 12 weeks after laser treatment.
Results:
Twenty-seven patients were enrolled (42.6 ± 7.7 years old), and duration of follow-up was 178.9 ± 88.8 (57.0–312.0) weeks. Nine patients (33.3%) were assigned to cCSC group, and the other 18 patients (66.7%) were assigned to the non-cCSC group. Twelve weeks after the laser treatment, subretinal fluid (SRF) of 15 patients (83.3%) in non-cCSC group and 5 patients (55.6%) in cCSC group absorbed completely; the height of SRF had statistical difference between two groups (p = 0.035); rough RPE was less common in cCSC group (p = 0.030); hyper reflective mass (HRM) was more common in cCSC group (p = 0.024); more number of hyper reflective foci (HRF) in outer segment of photoreceptor layer were detected in cCSC group (p = 0.035). From baseline to 12 weeks after laser treatment, the number of HRF in outer segment photoreceptor layer did not change significantly in cCSC group (p = 0.665) but decreased significantly in non-cCSC group (p = 0.000). A total of five patients suffered binocular CSC, three of them in the non-cCSC group occurred later than the other two in the cCSC group (129.9–278.3 weeks vs 96.1–114.9 weeks after baseline).
Conclusion:
SRF, rough RPE, HRM, and number of HRF in outer segment photoreceptor layer 12 weeks after laser treatment, and change in the number of HRF in outer segment photoreceptor layer from baseline to 12 weeks after laser treatment may predict the transition to cCSC.
Keywords
Introduction
Central serous chorioretinopathy (CSC) is characterized by serous detachment of retina. 1 It belongs to pachychoroid disease spectrum, 2 and the subretinal fluid (SRF) is the result from a hyperpermeable choroid together with increased hydrostatic pressure which induces a dysfunctional of retinal pigment epithelium (RPE). 3 CSC is divided into acute CSC (aCSC) and chronic CSC (cCSC) according to the duration of SRF and the resulting structural changes of retina. 1
Patients with aCSC usually presents with one or several focal leakage points with few atrophic changes of RPE, and the SRF may resolve spontaneously. 4 However, the spontaneous resolution of SRF does not always occur in patients with aCSC, 5% of them progressed to cCSC. 5 Patients with cCSC are characterized by long-term persistent SRF and irreversible structural damage including diffuse RPE leakage, wide spread areas of atrophic RPE alterations and photoreceptor damage. 6 Some patients even accept retinal laser photocoagulation at early stage, SRF still persists. 7
Patients with cCSC have poorer visual prognosis than aCSC; however, so far, little was known about the procession from aCSC to cCSC, especially patients with CSC accepted laser treatment. In this study, we explored the optical coherence tomography (OCT) biomarkers to predict the transition to cCSC after laser treatment by analyzing the OCT image at baseline and 12 weeks after laser treatment.
Materials and methods
Participants
Patients enrolled in this study were all from a ClinicalTrials.gov registered clinical trial (NCT02735213), which was a single-center, prospective, randomized, double-masked, non-inferiority, 12-week clinical trial comparing the efficacy and safety of subthreshold micropulse laser (SML) with threshold conventional laser (TCL) in the treatment of patients with CSC, whose leakage points were limited in Early Treatment Diabetic Retinopathy Study (ETDRS) ring 2 or 3, within 6 months of onset. 7 Some patients enrolled in this study continued to follow-up and be observed after the study ended. This study followed the guideline of observational study. The start date of the study was 12 April 2016, and the end date was 18 May 2022. Twenty-nine patients had extended follow-up in our center for more than 1 year from baseline. One woman of them transited to choroidal neovascularization (CNV), one man transited to polypoidal choroidal vasculopathy (PCV), and the other 27 patients were included in this study.
Participants divided into two groups, transited to cCSC group (cCSC group) and did not transited to cCSC group (non-cCSC group), according to the multimodal imaging of fundus at the last follow-up. The patients in cCSC group had active diffuse RPE leakage and persistent SRF accompanied with wide-spread areas of atrophic RPE alterations according to fundus examination, otherwise they were included in non-cCSC group.
Examinations
The OCT images, fundus fluorescein angiography (FFA) images, and best-corrected visual acuity (BCVA) of baseline and 12 weeks after laser treatment were all from the ClinicalTrials.gov registered clinical trial (NCT02735213). OCT images were from the examinations of spectral-domain optical coherence tomography (SD-OCT) (Spectralis; Heidelberg Engineering, Heidelberg, Germany), including 9-mm horizontal and vertical B-scan of macular with and without enhanced depth imaging (EDI) technology, volume mode (25-line consecutive scans, 20° × 20°, 5.8 × 5.8 mm) of the macula, and dense volume mode of leakage points. Leakage location and the number of leakage points of baseline were measured by FFA images (Spectralis, Heidelberg Engineering, Heidelberg, Germany). BCVA was in the form of ETDRS letters.
Whether the patient transited into cCSC was according to the multimodal imaging including OCT, FFA, indocyanine green angiography (ICGA) (Spectralis, Heidelberg Engineering, Heidelberg, Germany) and fundus autofluorescence (FAF) (Spectralis, Heidelberg Engineering, Heidelberg, Germany) during extended follow-up.
Some patients with pigment epithelium detachment (PED) need to exclude CNV through OCTA (Spectralis; Heidelberg Engineering, Heidelberg, Germany).
Outcome measurements
Central retinal thickness (CRT) defined as the average thickness of 1 mm in diameter centered on fovea was automatically determined by OCT mapping software by macular volume mode. The height of SRF was measured as the maximum vertical distance between the outermost hyper reflective line of the neurosensory retina and the innermost hyper reflective RPE line by B-scan of macular. 8 Choroid thickness (CT) was calculated under the fovea by EDI B-scan of macular. Hyper reflective foci (HRF) was divided into outer segment of photoreceptor HRF and intraretinal HRF according to the location (Figure 1). The number of HRF was determined by the horizontal B-scan through fovea of OCT (centered on fovea, 1500 μm temporally and nasally). 8 RPE alterations included rough RPE (only rough RPE without any other RPE alterations), flat irregularity PED, hyper reflective mass (HRM), and bulge PED (Figure 2), and determined by macula volume mode of OCT.

HRF on OCT: (a) HRF in outer segment photoreceptor layer (black arrow). (b) HRF in outer segment photoreceptor layer (black arrow) and intraretinal layer (red arrow).

RPE alterations on OCT: (a) rough RPE (only rough RPE without any other RPE alterations) (black arrow), (b) flat irregularity PED (black arrow), (c) HRM (black arrow), and (d) bulge PED (black arrow).
Laser treatment
For SML treatment, yellow (577 nm) micropulse laser model was used (Supra Scan 577; Quantel Medical, Cournon D’auvergne, France). The parameter: 5% duty cycle, 160 μm spot size, 9-spot matrix without spacing, 50% threshold power, and 150–200 burns. 7
For TCL treatment, yellow (577 nm) continuous laser mode was used (Supra Scan 577; Quantel Medical, Cournon D’auvergne, France). The laser parameter: 0.05 s duration time, 100 μm spot size, 9-spot matrix with one burn space, threshold power, and 18–27 burns. 7
Statistical analysis
All values are presented as the mean ± standard deviation (SD). Statistical analysis was performed with SPSS 24.0 (IBM, Chicago, IL) and a two-sided alpha level of 0.05. For univariate comparisons, analysis of variance (ANOVA) was used to compare the mean values of two groups of measurement data, such as age, BCVA, CRT, CT, height of SRF, and the number of HRF. Fisher exact test was used to analyze the significant differences in enumeration data, such as sex, leakage location, and the kind of RPE alterations. Logistic regression analysis was conducted for risk factors, and receiver operating characteristic (ROC) curve was drawn.
Results
Twenty-seven patients were included in this study, all males, average age was 42.6 ± 7.7 years old, and the average duration of follow-up was 178.9 ± 88.8 (57.0–312.0) weeks.
Nine patients (33.3%) transited to cCSC (cCSC group), whose average age was 44.3 ± 7.3 years old and average duration of follow-up was 112.8 ± 60.1 (57.0–214.3) weeks. The other 18 patients (66.7%) did not transite to cCSC (non-cCSC group), whose average age was 41.7 ± 7.9 years old and average duration of follow-up was 211.9 ± 83.1 (58.9–312.0) weeks. Patient demographics and baseline characteristics including BCVA, leakage points, and OCT biomarkers were in Table 1. Both groups were very similar in terms of the patient demographics and baseline characteristics.
Patient demographics and baseline characteristics at baseline prior to laser treatment.

BCVA, best-corrected visual acuity; cCSC, chronic central serous chorioretinopathy; CRT, central retinal thickness; CT, choroid thickness; HRF, hyper reflective foci; HRM, hyper reflective mass; PED, pigment epithelium detachment; RPE, retinal pigment epithelium; SRF, subretinal fluid.
Characteristics and OCT biomarkers 12 weeks after laser treatment are provided in Tables 2, and the change of OCT biomarkers from baseline to 12 weeks after laser treatment are provided in Table 3. Fibrous exudation was absorbed completely of both patients. Laser treatment has obvious effect to patients with CSC. Twelve weeks after laser treatment, BCVA improved, CRT and CT declined in both cCSC group and non-cCSC group (Figure 3). SRF of 15 patients (83.3%) in cCSC group and 5 patients (55.6%) in non-cCSC group absorbed completely, the average height of SRF significantly declined to 52.7 ± 67.8 μm and 11.4 ± 29.2 μm in cCSC group and non-cCSC group, respectively, 12 weeks after laser treatment, and there was statistical difference between two groups.
Characteristics and OCT biomarkers 12 weeks after laser treatment.
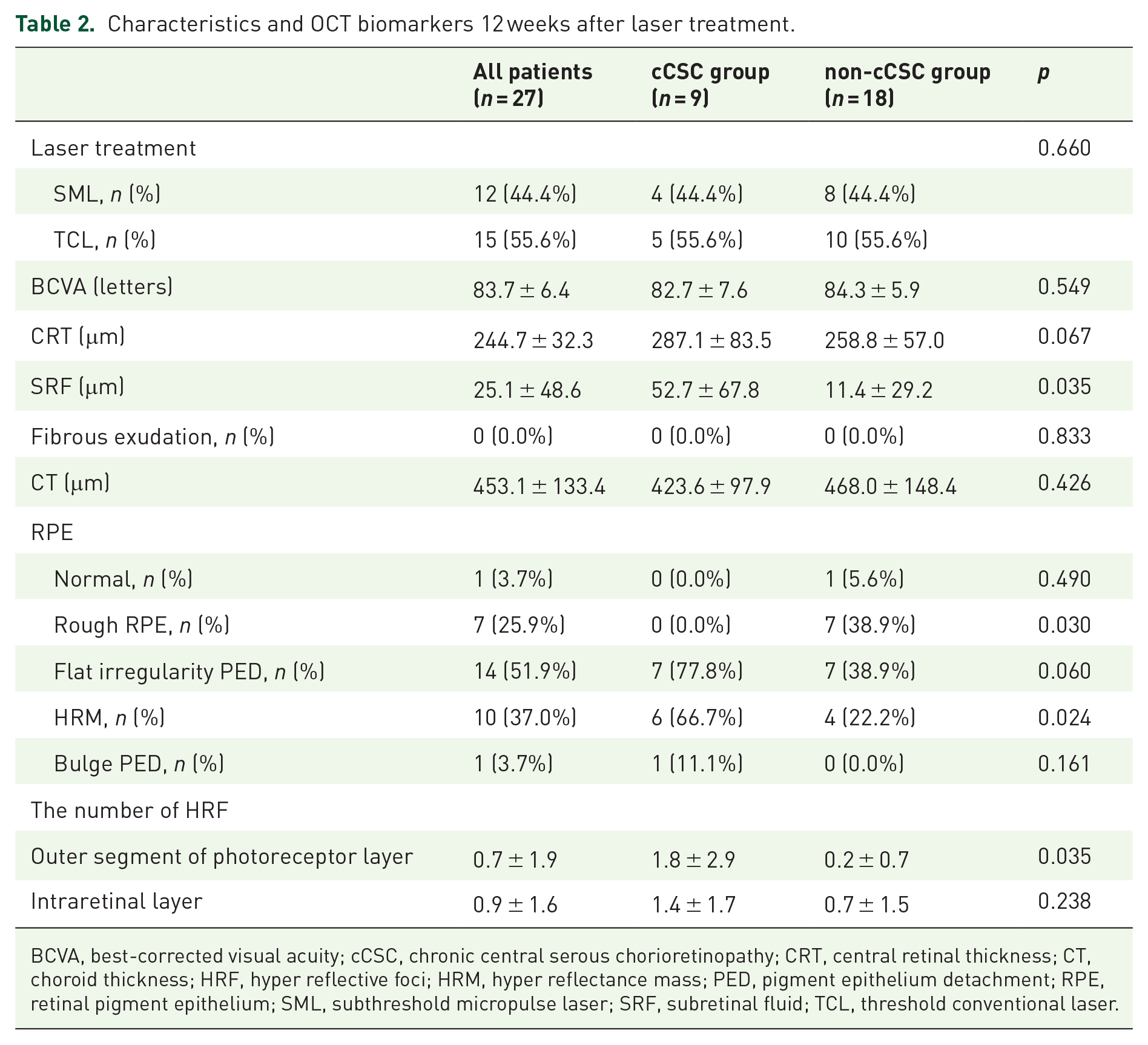
BCVA, best-corrected visual acuity; cCSC, chronic central serous chorioretinopathy; CRT, central retinal thickness; CT, choroid thickness; HRF, hyper reflective foci; HRM, hyper reflectance mass; PED, pigment epithelium detachment; RPE, retinal pigment epithelium; SML, subthreshold micropulse laser; SRF, subretinal fluid; TCL, threshold conventional laser.
The change of BCVA and OCT biomarkers from baseline to 12 weeks after laser treatment.

cCSC, chronic central serous chorioretinopathy; BCVA, best-corrected visual acuity; CT, choroid thickness; CRT, central retinal thickness; HRF, hyper reflective foci; SRF, subretinal fluid.

ROC curve. AUC = 0.772.
There were significant differences in SRF, rough RPE, HRM, and the number of HRF in outer segment of photoreceptor layer 12 weeks after laser treatment, and the change in number of HRF in outer segment of photoreceptor layer from baseline to 12 weeks after laser treatment, between CSC and non-CSC groups. ROC curve was drawn for the above parameters which were equivalent to predictors, and the area under ROC (AUC) was 0.722 (Figure. 3).
There were statistical differences of rough RPE, HRM, and the number of HRF in outer segment of photoreceptor layer between two groups 12 weeks after laser treatment. Seven patients (38.9%) presented rough RPE in non-cCSC group after laser treatment, and five of them (71.4%) accepted TCL. Both the number of HRF in outer segment photoreceptor layer and intraretinal layer did not change significantly in cCSC group, but decreased significantly in non-cCSC group (Figure 4). The occurrence probability of flat irregularity PED in cCSC group is about twice than that in non-cCSC group.

BCVA and OCT biomarkers at baseline and 12 weeks after laser treatment (*p < 0.05): (a) BCVA, (b) CRT, (c) SRF, (d) CT, (e) HRF in outer segment photoreceptor layer, and (f) HRF in intraretinal layer.
There was one patient with binocular CSC at baseline, and we chose the right eye of this patient for research eye. This patient transited to cCSC during the follow-up. During the extended follow-up period, a total of five patients developed binocular CSC, which occurred 178.4 ± 89.5 (96.1–178.3) weeks from the baseline. Three of them in non-cCSC group, occurred 278.3, 129.9, and 272.9 weeks from baseline, respectively; and two in cCSC group, occurred 114.9 and 96.1 weeks from baseline, respectively.
Discussions
One-third patients transited to cCSC in an average duration period of 112.8 ± 60.1 (57.0–214.3) weeks in this study. One previous study reported that 36% of eyes began as typical aCSC showed a progression of RPE alterations to appear a tendency toward chronic disease over an average time of 27 months, 9 which was inconsistent with the result of our study. Another study reported that around 60% of patients with aCSC showed progression of RPE alterations in at least 5 years, 10 the much higher progression to cCSC may be due to the much longer follow-up period.
CSC belongs to pachychoroid disease spectrum. 2 Pathological choroid affects the overlying RPE, gradually causing structural changes of retina, especially RPE. 11 There was statistically significant difference in RPE alterations 12 weeks after laser treatment between the two groups, including HRM and rough RPE. The HRM which was more common in cCSC group after laser treatment may be a predictor of whether CSC would transit to chronic disease. Rough RPE was defined only as unevenness of RPE without flat irregularity PED, HRM, bulge PED, and any other pathological changes in RPE. Rough RPE was more common in non-cCSC group after laser treatment. About 70% patients with rough RPE accepted TCL. Mild RPE depigmentation was detected in 12% patients 12 weeks after SML treatment by fundus photograph, whereas laser-induced changes were detected in 33% of patients after TCL treatment. 7 It was unclear that whether the change of RPE in this study was from laser treatment. Kulikov et al. 12 found that granular RPE changes and lucency of the RPE/choroid complex at the leak of CSC displayed the loss of pigmentation in both RPE and the choroid using dark-field scanning laser ophthalmoscopy (DF-SLO). Pigmented tissue is the target tissue of laser, and the loss of pigmentation may reduce the effect of laser on the retina. In addition, altered RPE may produce fewer biologically active molecules after laser treatment, which are responsible for the healing of the leak. 12
Spaide et al. 13 reported that the HRF in subretinal layer was the macrophages which phagocytosed the outer segments of photoreceptors, and it would migrate progressively into the neuroretina. We divided human fetal retina (HFR) into outer segment photoreceptor layer HFR and intraretinal layer HFR in this study (Figure 1). In cCSC group, the number of HRF in outer segment photoreceptor layer was decreased after laser treatment; however, the number of HRF in intraretinal layer was increased, which may due to the HRF in outer layer migrated to intraretinal layer with the persistent disease. The number of HRF after laser treatment and the variation in cCSC group was not as obvious as that in non-cCSC group, showing that the chronic transformation of CSC could be predicted from the number of HRF after laser treatment and the variation, especially the HRF in outer segment photoreceptor. Previous study showed that a higher number of HRF was associated with a longer duration of SRF, 14 which was in concordance with the results of our study.
The aCSC is usually suffered only in one eye, unfortunately, up to 42% of patients with cCSC have bilateral involvement. 15 There was only one patient with binocular CSC at baseline in this study, who was a 46-year-old man. Previous study showed the prevalence of bilateral CSC was 28% in patients under 50 years old, and increased to 50% in patients of 50 years or older; bilateral CSC was more common in older patients. 16 The only one bilateral CSC patient at baseline transited to cCSC during the follow-up in this study. A total of five patients developed binocular CSC during the extended follow-up period in this study, three of which in non-cCSC group occurred significantly longer than the two patients in cCSC group. It was speculated that maybe the earlier the onset of binocular CSC, the greater the possibility of progression to cCSC. Parameswarappa et al. 17 found that fellow eye information was helpful in solving diagnostic dilemmas.
The 577 nm wavelength belongs to yellow laser which is outside the absorption spectrum of retinal xanthophylls and beneficial to the treatment of leakage points close to fovea. 18 SML acted on leakage point instead of SRF area in this study. SML is the form of pulse, very short intervals of active impulses warm up RPE together with longer non-active intervals cool the RPE. 19 SML promoted heat shock protein expression of RPE cells without inducing RPE thermal damage. 20 Conventional laser seals the leakage points of CSC and accelerates the resolution of SRF, but its thermal damage may lead to retinal scars and scotoma. 21 TCL was used in this study, which was a threshold laser. Although TCL acting on the leakage point of CSC reduced the thermal damage, but it was still not favorable for the leakage points close to fovea. The leakage points of the patients enrolled in this study at baseline were all located on ring 2 or 3 of ETDRS ring. 7
Small cohort size was one of the limitations of this study. We observed choroid through EDI mode of OCT in this study, besides CT, there were no more choroidal biomarkers in this study, which could be detected by angio-OCT and high-resolution swept source OCT (SS-OCT). 22 RPE biomarkers were mainly read from OCT in this study. Affected by the detection characteristics and resolution of the machine itself in this study, there was no way to further discuss through our data results in the regard of status of RPE and choroid/choriocapillaris. In addition, more biomarkers can be obtained by multimodal imaging from fundus examinations like angio-OCT, SS-OCT, and DF-SLO, to establish machine learning models, but it requires more sample size. After 12 weeks of laser treatment, we did not specify the follow-up time, in the other words, the follow-up interval between the 12th week and the last visit was uncertain, so we cannot make a relatively accurate judgment on the duration of symptoms. That was another limitation of this study. The participants in this study were limited by the previous clinical trial, patients with central leakage and patients accepted photodynamic therapy (PDT) were not enrolled in this study.
Conclusion
In this study, we analyzed OCT biomarkers to predict the transition to cCSC of the CSC patients accepted laser treatment including SML and TCL. More SRF, less rough RPE, more HRM, and more number of HRF in outer segment photoreceptor layer 12 weeks after laser treatment may be risk factors of transition to cCSC.