
Abstract
Background:
Primary aldosteronism (PA) is the leading cause of secondary hypertension globally and is associated with adverse cardiovascular outcomes. However, the cardiac impact of concomitant albuminuria remains unknown.
Objective:
To compare anatomical and functional remodeling of left ventricle (LV) in PA patients with or without albuminuria.
Design:
Prospective cohort study.
Methods:
The cohort was separated into two arms according to the presence or absence of albuminuria (>30 mg/g of morning spot urine). Propensity score matching with age, sex, systolic blood pressure, and diabetes mellitus was performed. Multivariate analysis was conducted with adjustments for age, sex, body mass index, systolic blood pressure, duration of hypertension, smoking, diabetes mellitus, number of antihypertensive agents, and aldosterone level. A local-linear model with bandwidth of 2.07 was used to study correlations.
Results:
A total of 519 individuals with PA were enrolled in the study, of whom 152 had albuminuria. After matching, the albuminuria group had a higher creatinine level, at baseline. With regard to LV remodeling, albuminuria was independently associated with a significantly higher interventricular septum (1.22 > 1.17 cm, p = 0.030), LV posterior wall thickness (1.16 > 1.10 cm, p = 0.011), LV mass index (125 > 116 g/m2, p = 0.023), and medial E/e′ ratio (13.61 > 12.30, p = 0.032), and a lower medial early diastolic peak velocity (5.70 < 6.36 cm/s, p = 0.016). Multivariate analysis further revealed that albuminuria was an independent risk factor for elevated LV mass index (p < 0.001) and medial E/e′ ratio (p = 0.010). Non-parametric kernel regression also demonstrated that the level of albuminuria was positively correlated with LV mass index. The remodeling of LV mass and diastolic function under the presence of albuminuria distinctly improved after PA treatment.
Conclusion:
The presence of concomitant albuminuria in patients with PA was associated with pronounced LV hypertrophy and compromised LV diastolic function. These alterations were reversible after treatment for PA.
Plain language summary
Primary aldosteronism and albuminuria has been, respectively, demonstrated to bring about left ventricular remodeling, but the aggregative effect was unknown. We constructed a prospective single-center cohort study in Taiwan. We proposed the presence of concomitant albuminuria was associated with left ventricular hypertrophy and compromised diastolic function. Intriguingly, management of primary aldosteronism was able to restore these alterations. Our study delineated the cardiorenal crosstalk in the setting of secondary hypertension and the role of albuminuria for left ventricular remodeling. Future interrogations toward the underlying pathophysiology as well as therapeutics will facilitate the improvement of holistic care for such population.
Introduction
Primary aldosteronism (PA) is a well-established clinical entity that contributes to elevated blood pressure (BP) and systemic morbidities. Exaggerated aldosterone production in PA has been shown to be the leading cause of secondary hypertension worldwide, and epidemiology studies have demonstrated that 5–15% of individuals with hypertension have an underlying diagnosis of PA. 1 The pathological causes lie in hyperplasia or adenoma of the adrenal gland, which overwhelms renin system regulation leading to excessive aldosterone secretion and subsequently cardiovascular remodeling. Patients with PA have been reported to have a worse prognosis than those with essential hypertension. 2 Nevertheless, the interplay between renal dysfunction and PA as demonstrated by anatomical and functional alterations of the left ventricle (LV) has yet to be elucidated.
The cardiovascular impacts of PA are considered to be multifactorial. The presence of PA has been proposed to influence LV dynamics and dimension, and PA has been correlated with aggravated LV diastolic dysfunction. 3 Adrenalectomy has been shown to eliminate these deleterious effects, further endorsing the role of excessive aldosterone production in compromising LV diastolic performance. In addition, a high serum concentration of PA has been demonstrated to lead to remodeling of the structure of cardiac chambers, of which LV hypertrophy and local fibrosis are the predominant manifestations. 4 These structural changes eventually lead to decompensated heart failure, the onset of arrhythmia, and ischemia. 5 Taken together, these factors underscore that the presence of PA serves as an independent risk factor of a poor cardiovascular prognosis.
The collective clinical effect of comorbidities along with PA is a paramount issue of concern. Among these comorbidities, albuminuria shares a common etiology and is often complicated with PA. Altered renal function has been shown to result in LV hypertrophy, 6 and the urine albumin to creatinine ratio (UACR) has been positively correlated with LV mass. 7 Nevertheless, how concomitant albuminuria influences cardiovascular parameters in PA is unknown. Although the respective impacts of PA and albuminuria on LV configuration have been elucidated separately, the synergistic effect compared with PA alone has not been previously reported. Therefore, the aim of this study was to elucidate how albuminuria affects LV dimension and functionality in the presence of excessive aldosterone.
Materials and methods
Patients
We dynamically enrolled subjects with PA in this prospective cohort study from January 2006 to April 2020 at National Taiwan University Hospital. These individuals were registered in the Taiwan Primary Aldosteronism Investigation (TAIPAI) database.8,9 Individuals with secondary hypertension due to other etiologies, including pheochromocytoma, Cushing’s syndrome, hyperthyroidism, and renovascular causes, were excluded. The demographic characteristics, and laboratory and echocardiographic parameters were manually recorded and reviewed. Serum and urine samples were collected at the first encounter for analysis. Albuminuria was defined as greater than 30 mg/g of urine albumin–creatinine ratio by morning spot urine. The definitions of diabetes mellitus (DM) and hypercholesterolemia were rendered according to guideline and previous study.10,11 Commercially available radioimmune assay kits (Aldosterone Maia Kit; Adaltis Italia, Bologna, Italy; DiaSorin, Stillwater, Minnesota) were used, respectively, to quantify plasma aldosterone concentration (PAC) and plasma renin activity (PRA). The cohort was monitored for 1 year after the treatment. Sample size was determined by employing G-power with alpha error at 0.05 and power at 0.8. Informed consent was obtained from each subject, and approval to conduct this study was obtained from the Institutional Review Board at our center (IRB number: 200611031R).
Diagnostic criteria and management of PA
The diagnosis of PA was confirmed if patients met the following three criteria: (1) aldosterone-to-renin ratio > 35, (2) a TAIPAI score > 60%, and (3) post-saline loading PAC > 10 ng/dl or aldosterone-to-renin ratio > 35 (ng/dl)/(ng/ml/h) in the post-captopril test; or PAC > 6 ng/dl in the fludrocortisone suppression test. Details of the protocol can be found in our previous study. 12
The treatment of PA was either pharmaceutical with mineralocorticoid receptor antagonists or surgical resection with laparoscopic adrenalectomy via a lateral transperitoneal approach performed by experienced operators.
Echocardiographic assessments
An echocardiography system (IE33, Philips; Andover, Massachusetts, USA) was used for all assessments. A transthoracic approach with fundamental two-dimension view, M-mode assessment, and Doppler evaluation was applied. According to the latest American Society of Echocardiography guidelines, 13 LV dimensions and wall thickness were evaluated from a parasternal long axis view. LV mass index was quantified using Devereux and Reichek’s methodology based on body surface area. Under a four-chamber view in tissue Doppler imaging, a 3-mm sample volume at the mitral valve tips was used to examine the transmitral flow velocity as well as early (E) and late (A) diastolic filling velocities. Early diastolic peak velocity at the medial and lateral septal mitral annulus (e′) was also assessed, and E/e′ ratio was obtained to indicate LV filling pressure. 14 All of these parameters were derived from the average of values obtained from three consecutive cardiac cycles.
Statistical analysis
Statistical Package for Social Sciences software (version 21.0, SPSS Inc., Chicago, Illinois, USA) was used for all analyses in this study. Categorical parameters were expressed as number with percentage, and normally distributed continuous variables were expressed as mean ± standard deviation. Propensity scores were estimated using non-parsimonious multiple logistic regression models after considering age, sex, body mass index (BMI), systolic and diastolic BP, duration of hypertension, and number of antihypertensive medications. A 1:1 matching ratio was using in the propensity matching to balance the covariates between the two arms. Non-parametric kernel regression with Epanechnikov kernel function was used to analyze correlations between the level of albuminuria and LV mass index. The two-sample test was used to compare continuous parameters between two groups, and the Student’s t test was applied to evaluate the alteration before and after PA treatment. Bonferroni correction was utilized in the setting of multiple comparisons. A p value < 0.05 was considered to be statistically significant.
Results
Demographic and biochemical characteristics before and after matching
A total of 519 individuals with PA were enrolled in this study, of whom 152 were diagnosed with albuminuria. After 1:1 matching for established cardiovascular risk factors, including age, sex, systolic BP, and DM, there were 132 subjects in each arm (with and without albuminuria) (Figure 1). The demographic characteristics and clinical parameters at baseline before and after propensity score matching are summarized in Table 1. Before propensity score matching, no significant differences were found in age, sex, hypercholesterolemia, use of cholesterol-lowering agents, smoking, BMI, PAC, PRA, and aldosterone–renin ratio. A significantly greater number of patients with albuminuria had DM, elevated BP, elevated initial creatinine level, and hypokalemia, and were prescribed with a greater number of antihypertensive agents.

Flowchart of study design.
Baseline demographic characteristics and laboratory parameters of enrolled patients before and after propensity score matching.
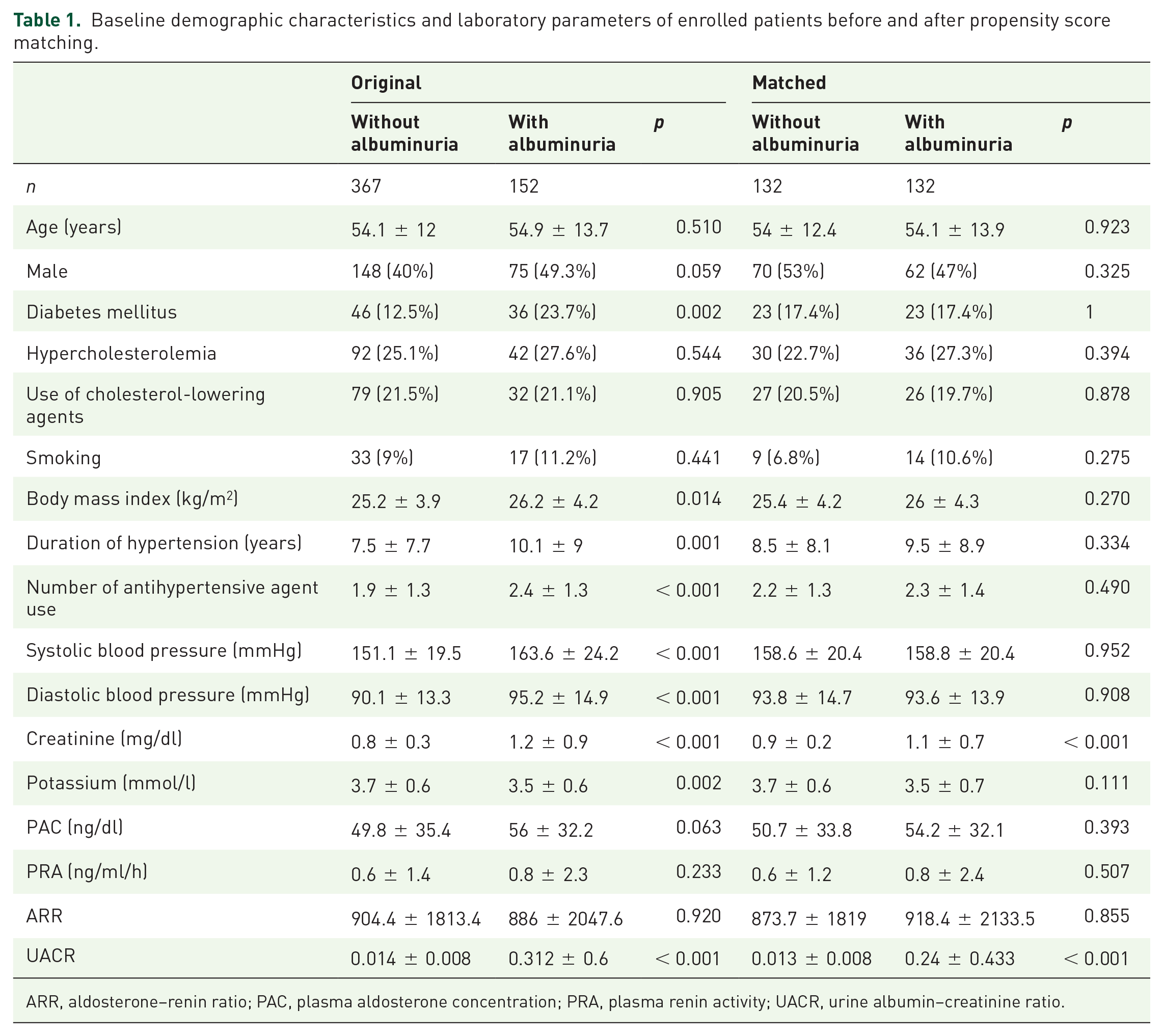
ARR, aldosterone–renin ratio; PAC, plasma aldosterone concentration; PRA, plasma renin activity; UACR, urine albumin–creatinine ratio.
After propensity score matching, there were otherwise no significant differences in baseline demographic and clinical parameters except patients with albuminuria had higher initial serum creatinine level. These findings indicated the considerable similarity in baseline patient profiles.
Echocardiographic parameters before and after matching
With regard to the echocardiographic assessments (Table 2), after propensity score matching, the albuminuria group had a significantly greater end-diastolic interventricular septum (IVSD) (1.17 ± 0.19 versus 1.22 ± 0.21 cm; p = 0.03) and LV posterior wall thickness (LVPWd) (1.10 ± 0.15 versus 1.16 ± 0.19 cm; p = 0.011). In addition, the LV mass index (116.81 ± 27.36 versus 125.61 ± 34.61 g/m2; p = 0.023) was significantly higher in the albuminuria group. Non-parametric kernel regression also revealed a positive correlation between albuminuria and LV mass index (Figure 2). However, there were no significant differences in LV volume and internal diameter at either end-diastolic or end-systolic phase. In addition, LV diastolic function was compromised in the albuminuria group. There were significant differences in mitral valve A wave velocity (81.52 ± 16.23 versus 87.77 ± 19.14 cm/s; p = 0.005) and medial early diastolic peak velocity (6.36 ± 2.15 versus 5.7 ± 1.54 cm/s; p = 0.016), but not E wave velocity (73.55 ± 18.86 versus 74.47 ± 19.08 cm/s; p = 0.695).
Echocardiographic assessments of left ventricle before and after propensity score matching.

ie, inappropriately excessive; IVSD, interventricular septal end-diastole thickness; LV, left ventricle; LVEDD, LV end-diastolic diameter; LVESD, LV end-systolic internal diameter; LVMI, LV mass index.

Correlation between the level of albuminuria and left ventricular mass index.
Furthermore, the patients were stratified based on the level of UACR (0, 30–300, >300 mg/g) and assessed the impacts on LV mass and LV mass index. Statistical significance was present among the groups (Bonferroni p all < 0.001) (Supplementary Table 1).
Factors associated with LV hypertrophy and diastolic dysfunction
Both univariate and multivariate analyses were performed to further analyze the correlations between albuminuria and LV characteristics. The results showed that DM, smoking, BMI, duration of hypertension, number of antihypertensive agents, BP, creatinine level, potassium level, PAC, and UACR were independently associated with the alteration of LV mass index, while additionally age but not duration of hypertension diastolic BP, potassium level, and PAC remarkably impacted medial E/e′ ratio (Table 3). In the multivariate analysis, six models were established to eliminate possible confounding factors, which included age, sex, BMI, systolic BP, duration of hypertension, smoking, DM, number of antihypertensive agent, and aldosterone level. After adjustments, albuminuria remained significantly associated with LV mass index, medial E/e′ ratio (Table 4), as well as LV hypertrophy (Supplementary Table 2).
Univariable regression for the association between clinical or laboratory variables and left ventricular mass index or medial E/e’ ratio.
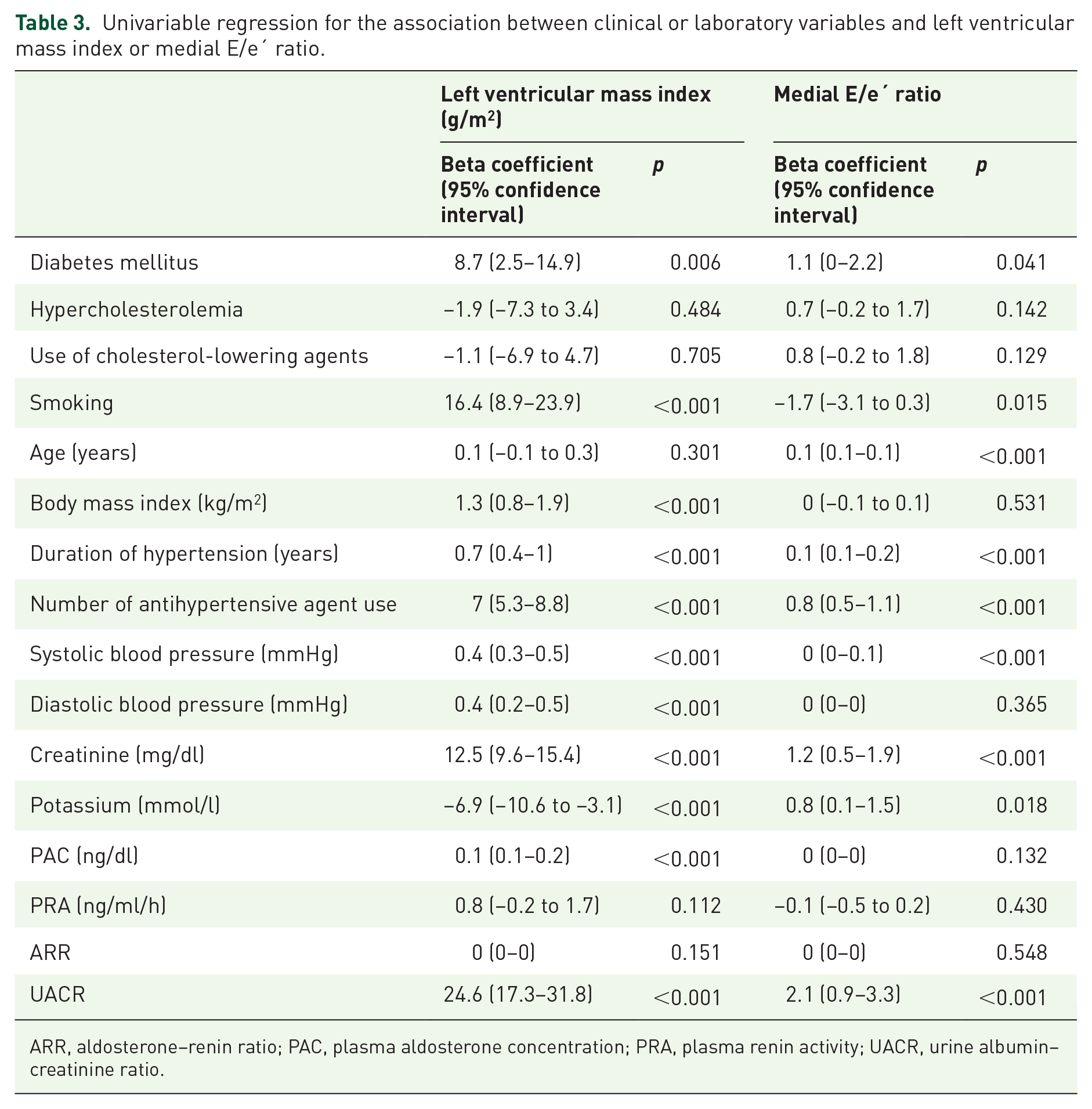
ARR, aldosterone–renin ratio; PAC, plasma aldosterone concentration; PRA, plasma renin activity; UACR, urine albumin–creatinine ratio.
Multivariable regression analysis for the association between albuminuria and left ventricular mass index or medial E/e’ ratio.
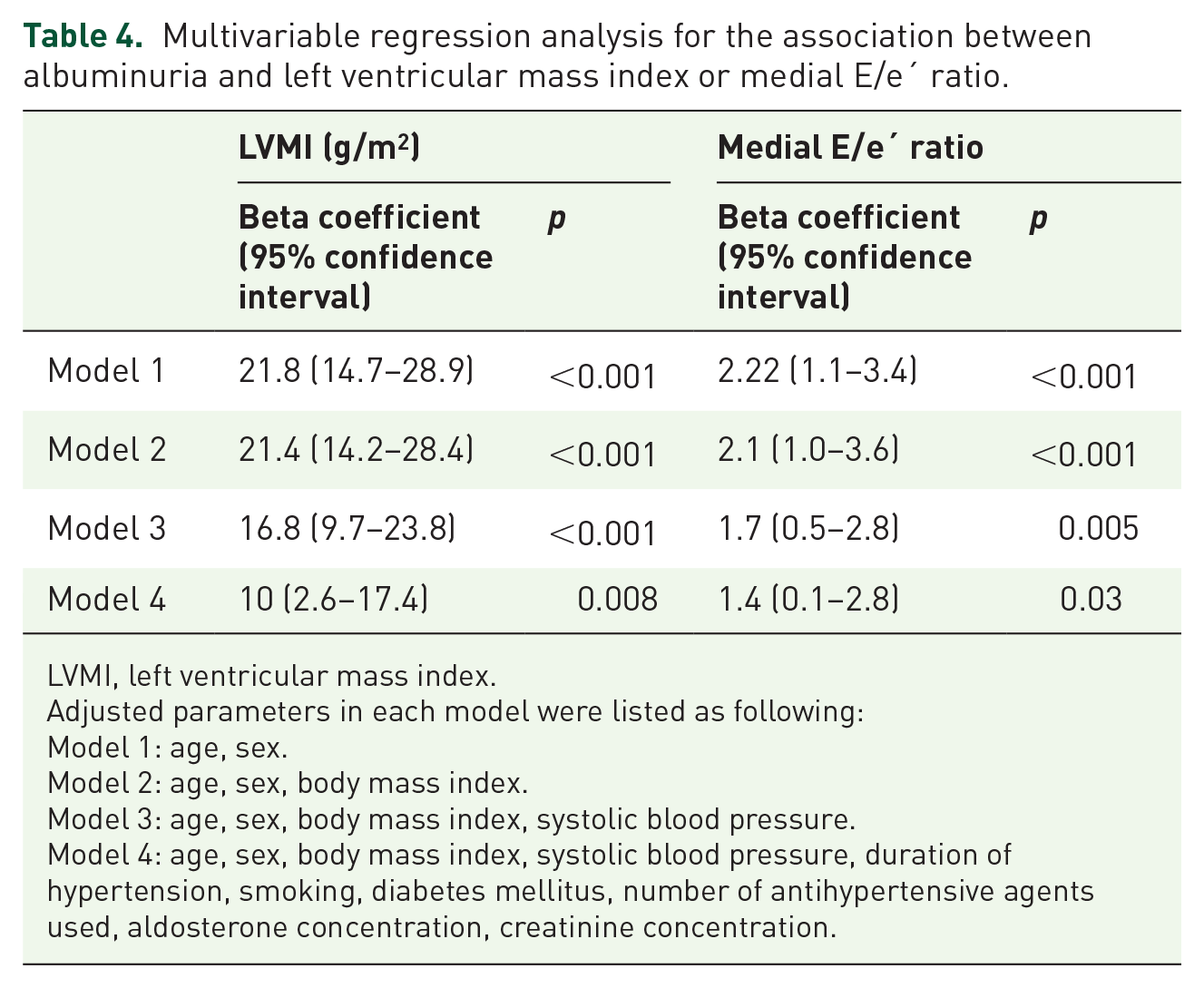
LVMI, left ventricular mass index.
Adjusted parameters in each model were listed as following:
Model 1: age, sex.
Model 2: age, sex, body mass index.
Model 3: age, sex, body mass index, systolic blood pressure.
Model 4: age, sex, body mass index, systolic blood pressure, duration of hypertension, smoking, diabetes mellitus, number of antihypertensive agents used, aldosterone concentration, creatinine concentration.
Alteration of demographic and clinical parameters after PA treatment
Alteration of UACR level was compared before and after PA treatment. The difference all reached significance in overall population as well as in patients with or without baseline albuminuria. Moreover, the systolic BP and diastolic BP were effectively improved by PA treatment in the cohort (Supplementary Table 3). Interestingly, PA treatment resulted in significant decreases in IVSD (p < 0.001), LVPWd (p < 0.001), LV mass (p < 0.001), and LV mass index (p < 0.001) regardless of albuminuria status. However, diastolic dysfunction was only reversed in the patients with albuminuria. A significant increase in medial peak early diastolic velocity (5.63 ± 1.53 versus 6.04 ± 1.74 cm/s; p = 0.025) and decrease in medial E/e′ ratio (13.60 ± 4.16 versus 12.37 ± 3.52; p = 0.020) were observed only in the patients with albuminuria (Figure 3).

Dimension and diastolic function of LV before and after treatment of primary aldosteronism: (a) IVS, (b) LV mass index, and (c) E/e’ ratio.
Discussion
Individuals with PA have been shown to have an increased prevalence of LV remodeling; however, the synergistically deleterious effect of albuminuria has rarely been reported in previous investigations. In this prospective cohort study with propensity score matching, we demonstrated that the presence of albuminuria was significantly associated with anatomical and functional LV remodeling. Moreover, these alterations were considered to be reversible as they were ameliorated after PA treatment. These results implied that compromised renal function in addition to excessive aldosterone may be correlated with LV hypertrophy and dysfunction.
Albuminuria is a significant morbidity in patients with PA. An early observational study suggested that PA may be related to excessive urinary excretion of albumin. 15 In the PAPY (Primary Aldosteronism Prevalence in Italy) study, the prevalence of albuminuria was significantly higher in individuals with PA than in those with essential hypertension. 16 A subsequent epidemiological phenotype study found that the incidence of albuminuria in individuals with PA was 27%. 17 The pathogenesis has been proposed to be through hypokalemia and elevated serum aldosterone level, leading to compromised reabsorption over proximal renal tubules. 18 A stimulated renin-angiotensin system has also been associated with nephropathy, and relative hyperfiltration has been associated with PA-related renal dysfunction. 19 From a mechanistic perspective, the excessive accumulation of aldosterone has been shown to damage the endothelial glycocalyx through matrix metalloproteinases, eventually inducing albuminuria. 20 These findings suggest that albuminuria may be the manifestation of functional renal sequelae secondary to PA. In addition, adrenalectomy has been shown to improve albuminuria status, and resection of aldosterone-producing adenoma has been demonstrated to rescue the progression of renal function decline. 21 The findings of our study echo the interplay between PA and albuminuria, and both cardiac anatomical remodeling and diastolic function were significantly improved after either medical or surgical anti-aldosterone treatment.
PA per se has been demonstrated to alter the cardiac architecture. Pathologically accumulated concentrations of serum aldosterone not only lead to electrolyte imbalance but also to ventricular fibrosis and hypertrophy. The Randomized Aldactone Evaluation Study demonstrated that the administration of a mineralocorticoid receptor antagonist remarkably ameliorated the turnover of extracellular matrix by reducing the level of procollagen type III N-terminal peptide. 22 Another possible mechanism was the activated inflammatory status secondary to PA, in which the generation of superoxide and hydrogen peroxide activated the nuclear factor kappa B pathway and Ca2+/calmodulin-dependent protein kinase II, 23 thereby remodeling the anatomy of the LV. In vitro studies have shown that accumulating concentrations of serum aldosterone can activate the signaling transduction of protein kinase C, extracellular signal-regulated kinase 1/2, and c-Jun N-terminal kinase. 24 In addition, aldosterone has been shown to play a key role in inducing fibrosis. Classic profibrotic molecules associated with aldosterone include transforming growth factor-β1 and endothelin 1. 25 Another pivotal factor is tissue inhibitor of metalloproteinases-1 (TIMP-1). Our previous study delineated the positive correlation between TIMP-1 and LV mass in both a mouse model and in 54 enrolled individuals with PA. 26 These findings support the clinical implication of PA in remodeling of the LV.
LV remodeling has been related to the presence of albuminuria in various clinical backgrounds. The Appropriate Blood Pressure Control in Diabetes trial reported that UACR was an independent predictive factor for increased LV mass and cardiovascular mortality. 27 A slightly elevated UACR, even if the elevation is not over the conventional threshold of proteinuria, has been demonstrated to alter LV diastolic function and cause LV hypertrophy in hypertensive individuals. 28 In addition, in patients progressing to heart failure, albuminuria has still been associated with cardiac chamber remodeling and a poor prognosis. 29 Echoing this finding, the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist) study enrolled 1175 individuals and suggested that patients with albuminuria are at a higher risk of major adverse cardiovascular events. 30 Furthermore, correction of the UACR was associated with an improved prognosis, implying that albuminuria may serve as a therapeutic target.
Previous studies have mostly excluded subjects with secondary hypertension, and the cardiovascular outcomes of patients with PA and albuminuria have not been reported. The rationale of this study was therefore to focus on this specific population to understand both anatomical and functional adaptations of the LV. The strength of this study lies in the comprehensive assessments of echocardiographic parameters with regard to both LV anatomy and diastolic performance in patients with PA and albuminuria. We also found that albuminuria was correlated with the extent of hypertrophic LV mass. As for future perspectives, elucidating changes in the molecular landscape caused by the presence of albuminuria would be pivotal to explain the cardiorenal crosstalk in PA. Such investigations will also lead to the identification of potential therapeutic targets to rescue cardiac remodeling and diastolic dysfunction.
There are several limitations to this study. First, even though this is the largest study on this topic to date, the sample size was limited. Future large-scale studies are needed to validate our findings. Second, although propensity score matching was used to eliminate the established confounding factors, other unidentified parameters may have led to bias between the two arms of this study. Third, the chamber dimension and mechanical properties were evaluated using echocardiography only, and other imaging modalities such as cardiac magnetic resonance imaging for further structural assessments were not performed. Fourth, the diagnosis of albuminuria was based on single assay of spot urine at initial encounter without further repetition of the test weeks after.
Conclusion
This prospective cohort study provides insights into cardiorenal interplay in a specific patient group with secondary hypertension. The presence of albuminuria predisposed LV hypertrophy and remodeling in individuals with PA. Thickened interventricular septum and enlarged LV dimension may be related to impaired renal function, and the management of PA may be able to ameliorate such alterations. Detailed investigations on the bidirectional cardiorenal crosstalk will advance the understanding of cardiac remodeling and eventually to improved holistic care for this population.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221143253 – Supplemental material for Anatomical and functional remodeling of left ventricle in patients with primary aldosteronism and concomitant albuminuria
Supplemental material, sj-docx-1-taj-10.1177_20406223221143253 for Anatomical and functional remodeling of left ventricle in patients with primary aldosteronism and concomitant albuminuria by Ting-Wei Kao, Xue-Ming Wu, Che-Wei Liao, Cheng-Hsuan Tsai, Zheng-Wei Chen, Yi-Yao Chang, Bo-Ching Lee, Yu-Wei Chiu, Tai-Shuan Lai, Vin-Cent Wu, Yen-Hung Lin and Chi-Sheng Hung in Therapeutic Advances in Chronic Disease
Footnotes
Appendix 1
Membership of the TAIPAI (Taiwan Primary Aldosteronism Investigation) study group: Che-Hsiung Wu, MD (Chi-Taz Hospital, PI of Committee); Vin-Cent Wu, MD (NTUH, PI of Committee); Yen-Hung Lin, MD (NTUH, PI of Committee); Hung-Wei Chang, MD, PhD (Far Eastern Clinics, PI of Committee); Lian-Yu Lin, MD, PhD (NTUH, PI of Committee); Fu-Chang Hu, MS, ScD (Harvard Statistics, Site Investigator); Kao-Lang Liu, MD (NTUH, PI of Committee); Shuo-Meng Wang, MD (NTUH, PI of Committee); Kuo-How Huang, MD (NTUH, PI of Committee); Yung-Ming Chen, MD (NTUH, PI of Committee); Chin-Chen Chang, MD (NTUH, PI of Committee); Shih-Cheng Liao, MD (NTUH, PI of Committee); Ruoh-Fang Yen, MD, PhD (NTUH, PI of Committee); and Kwan-Dun Wu, MD, PhD (NTUH, Director of Coordinating Center).
Acknowledgements
We are greatly thankful to I-Ju Chang, Fang-Yu Yang, and Lung-Chun Lin for their assistance and advices for echocardiography.
Declarations
Supplemental material
Supplemental material for this article is available online.