
Abstract
Background:
Atrial fibrillation (AF) has affected millions of adults in the world. It is important to monitor and manage blood pressure (BP) in AF patients. The accuracy of BP monitoring in AF patients with noninvasive methods remains questionable, however.
Objectives:
To compare the accuracy of different noninvasive BP devices (oscillographic sphygmomanometer and pulse wave device) for BP measurement in elderly patients with AF, with a mercury sphygmomanometer as a reference.
Design:
This study was an observational study.
Methods:
Patients with AF from the inpatient department of cardiology were included from 1 January to 31 December 2020. BP measurements were performed by two trained nurses using a tee junction connection on the cuff to connect three sphygmomanometers. The Bland–Altman plot analysis was conducted to compare the agreement of BP measurements. We also compared the agreement of BP measurements through metrics such as accuracy, bias, and precision.
Results:
A total of 202 patients (54.5% female) were included. The Bland–Altman plot analysis showed that the lower and upper limits of agreement (LoAs) of pulse wave/reference were similar to the predefined acceptable clinical limits (10/5 mmHg). The bias and precision in both systolic and diastolic BP were significantly less in pulse wave/reference (a bias of 1.8 and 0.77 mmHg and a precision of 5.20 and 4.66 mmHg, respectively), with corresponding higher accuracy readings (98.51% for P10 in systolic BP and 85.64% for P5 in diastolic BP).
Conclusion:
A novel noninvasive sphygmomanometer – pulse wave device has a good concordance with a mercury sphygmomanometer in BP monitoring, and may be applicable to perform BP measurements in the elderly with AF.
Keywords
Introduction
Atrial fibrillation (AF), the most common cardiac arrhythmia, has affected millions of adults in the world. 1 AF can raise the risk of stroke, heart failure, disability, and mortality, thus portending a significant burden to patients and society. 1 It is now established that elevated blood pressure (BP) is one of the most important risk factors for AF.1–4 Studies also showed that better BP control was associated with lower cardiovascular outcomes in AF. 4 Therefore, it is important to monitor and manage BP in AF patients.
The accuracy of BP monitoring in AF patients with noninvasive methods remains questionable, however. Currently, noninvasive BP measurement methods include mercury sphygmomanometer, mechanical sphygmomanometer (e.g. spring-based devices), and oscillographic sphygmomanometer. Owing to the potential environmental pollution of mercury, mercury sphygmomanometers will be deprecated gradually. The mechanical sphygmomanometers are not widely used and the accuracy of the readings will be affected by the change of spring elastic with the increase of measurement times and may be not suitable in out-of-clinic settings, especially for the elderly. Oscillographic devices detect oscillations (or movement) of the arterial vessel wall during each cardiac contraction and calculate the BP via an internal algorithm. Current studies on the accuracy of BP measurement of oscillographic devices in AF showed inconsistent results.5–10 With the rapid development of electronic technology, the pulse wave sphygmomanometer, a novel BP monitor device, has been widely used in clinical practice in China. Previous studies had demonstrated the accuracy of pulse wave sphygmomanometer in patients undergoing coronary angiography and children aged 3–12 years. 11 Limited studies were performed on AF patients with the pulse wave devices, however.
Therefore, we conduct this observational study to compare the accuracy of two different noninvasive BP devices (oscillographic sphygmomanometer and pulse wave device) for BP measurement in elderly patients with AF, with a mercury sphygmomanometer as reference.
Methods
Study population and design
This observational study was approved by the ethics committee of Shunde Hospital of Southern Medical University (no. 20190601). This study was performed according to the ethical standards as the Declaration of Helsinki. We recruited participants from the inpatient department of cardiology from 1 January to 31 December 2020 in Shunde Hospital, Southern Medical University, with the following inclusion criteria: (1) aged 60–90 years; (2) with electrocardiogram (ECG)-confirmed AF at admission; (3) having provided written informed consent; (4) compliance with BP measurements; and (5) no severe skin, muscle, or bone damage at the measurement and auscultation sites. Patients who were restored to sinus rhythm, not suitable for the standard cuff (with a bladder of 12 cm wide and 22–26 cm long), and suffering from tremor disease (such as Parkinson’s disease, fever, epilepsy, and so on) were excluded.
BP measurement and devices
The features and BP determination methods of the pulse wave device were described in the previous study. 11 In brief, the pulse wave device collected the pulse wave curve from the cuff to calculate the systolic BP. The diastolic BP was confirmed when the ‘delay time’ stay constant, which was defined as the constant interval of the pulse wave signal from top to bottom of the cuff when the cuff pressure was going down.
After enrollment, we first performed cardiac auscultation and palpation of pulse to confirm the diagnosis of AF again. BP measurements were performed by two trained nurses using tee junction connections on the cuff to connect three sphygmomanometers (Mercury sphygmomanometer 19160027, Jiangsu Yuwell Medical Equipment & Supply Co., Ltd, China; Pulse wave BP-88G, Shenzhen Ruiguang Kangtai Co., Ltd, China; Oscillographic WBP202, Guangdong Biolight Meditech Co., Ltd, China). BP measurements were conducted in accordance with the 2018 Chinese guidelines for hypertension prevention and treatment, 12 and performed on the right upper arm. Participants were asked to rest for at least 10 min before measurements and be in a straight sitting position with the measured upper arm exposed and the elbow kept at the same level as the heart at the time of measurements. When measuring the BP, one nurse took readings from the mercury sphygmomanometer, while the other took readings from the electronic devices at the same time, and the readings were taken by two nurses independently. Phases I and V Korotkoff sounds were used to determine systolic BP and diastolic BP for the mercury sphygmomanometer. Each sphygmomanometer was measured twice, and each measurement would be taken after 1–2 min intervals. The average of the two readings will be recorded as the final BP values of each device. In some cases, the automated devices reported error readings but not BP data, we performed the measurement using tee junction connections again, and only BP data were all available from the three devices in the same measurement, they were recorded.
Statistical analysis
Statistical analysis was performed using SPSS 20.0 (IBM Corporation, Armonk, NY, USA) and MedCalc 21.0 (MedCalc Software Ltd, Ostend, Belgium). All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
BP readings were expressed as mean value ± standard deviation. Intraclass correlation coefficients (ICCs) were calculated as two-way random ICCs for an absolute agreement based on two measurements within the BP devices. The Bland–Altman plot analysis was conducted to compare the agreement of BP measurements, including the 95% confidence interval (CI) of the lower and upper limits of agreement (LoAs), the mean difference, and the predefined acceptable clinical limits of ±10/5 mmHg for measurements difference of systolic/diastolic BP values, with mercury sphygmomanometer as reference. In our preliminary study, we obtained data from 30 AF patients to predict an estimated sample size needed in the Bland–Altman plot analysis according to the method proposed by Lu et al., using the sample size calculation function of MedCalc. 13 Because we focused on the clinical use of a novel noninvasive sphygmomanometer – pulse wave device, and we paid more attention to systolic BP in the usual clinical setting, the value of systolic BP by pulse wave and mercury sphygmomanometer was used to calculate the sample size. Our data showed that the mean difference of two devices of preliminary 30 AF patients is 3.08 mmHg (we conservatively predicted it as 4–5 mmHg, which would need a larger sample size), and the standard deviation of the difference is 2.35 mmHg (we predicted it as 2.3–2.4 mmHg). We set the maximum allowed difference for systolic BP between two methods as 10 mmHg. A sample size of 61–217 patients was required to provide 80% study power to detect a type I error at 0.05.
We also compared the agreement of BP measurements through metrics such as accuracy, bias, and precision. 14 Accuracy was expressed as the percentage of participants’ BP difference between pulse wave device or oscillographic device and mercury sphygmomanometer less than 10% and 15% (P10, P15) for systolic BP and 5% and 10% (P5, P10) for diastolic BP. The bias and precision of the individual measured BP by the pulse wave device or oscillographic device compared with the mercury sphygmomanometer (BP reference) were evaluated by the following equations

Results
A total of 202 patients (54.5% female) with AF were included, with an average age of 73.5 years. Among these participants, 62.4% had concurrent hypertension. The mean systolic BP in the oscillographic group, pulse wave group, and reference group was 115.66 ± 17.22 mmHg, 121.09 ± 20.54 mmHg, and 122.86 ± 19.03 mmHg, respectively, and the mean diastolic BP in the above groups was 69.3 ± 10.45 mmHg, 73.97 ± 11.65 mmHg, and 73.2 ± 10.43 mmHg, respectively.
The comparison of repeated measurements’ consistency of BP in each sphygmomanometry was conducted, which showed that the ICC of systolic BP was 0.943 (95% CI = 0.914–0.961) in oscillographic, 0.947 (95% CI = 0.930–0960) in pulse wave, and 0.956 (95% CI = 0.942–0.967) in the reference group. For diastolic BP, the corresponding ICC was 0.923 (95% CI = 0.896–0.942), 0.869 (95% CI = 0.827–0.901), and 0.903 (95% CI = 0.871–0.927), respectively (Table 1). The Bland–Altman plot analysis showed that the systolic and diastolic BP’s LoAs of oscillographic/reference (95% CI = 5.4 to 19.9 mmHg for systolic BP and −6.5 to 14.3 mmHg for diastolic BP) were outside the maximum tolerated difference. In contrast, the LoAs of pulse wave/reference were within the predefined acceptable clinical limits (10/5 mmHg), revealing the more acceptable agreement of BP readings by pulse wave sphygmomanometry and mercury sphygmomanometry (Figure 1).
Comparison of repeated measurements’ consistency of blood pressure intra groups.
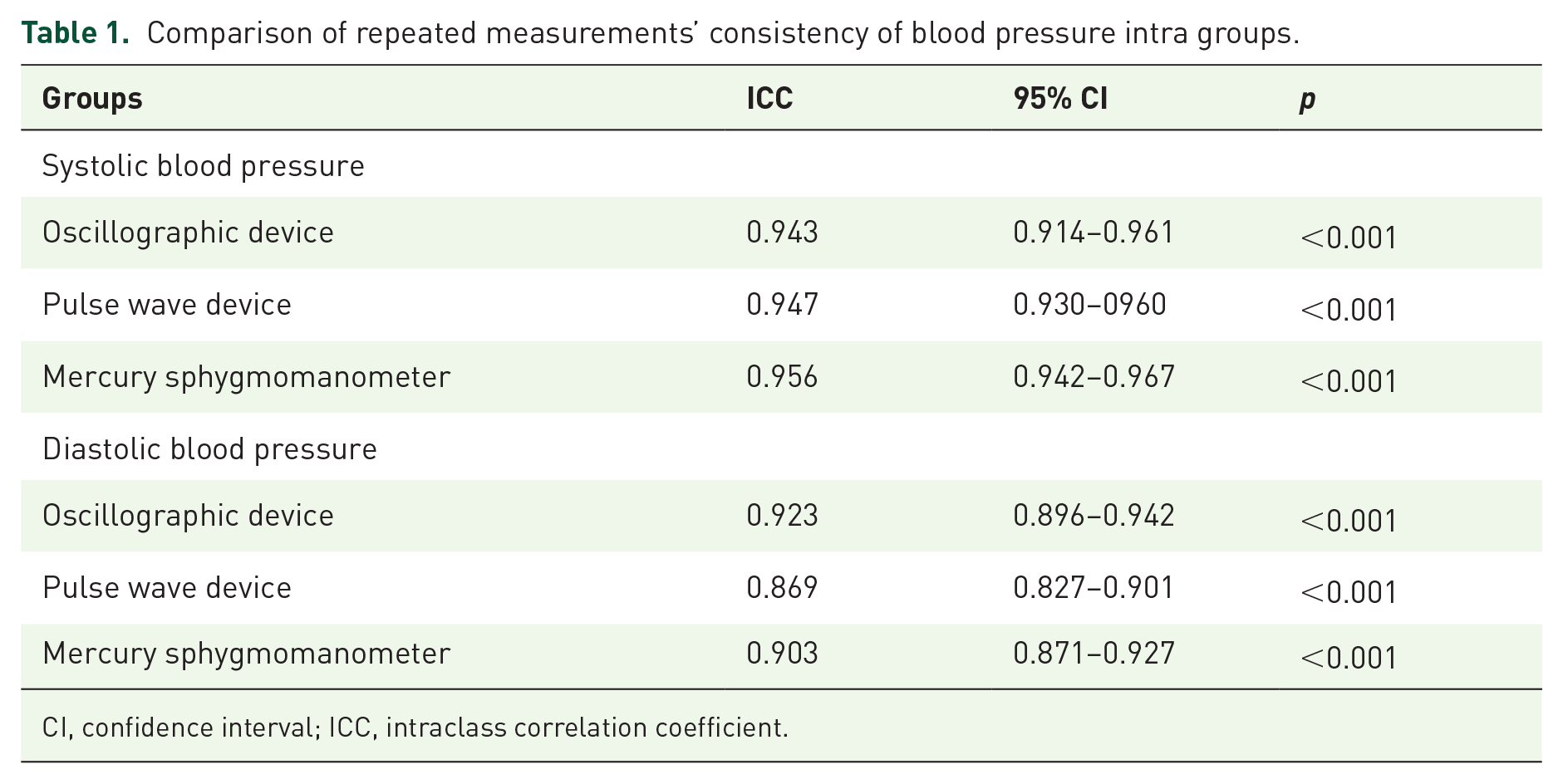
CI, confidence interval; ICC, intraclass correlation coefficient.

Bland–Altman analysis of BP differences among electronic devices and reference group. Bland–Altman plots include the mean difference (blue), limits of agreement (red dotted line) with an approximate 95% CI of the limits of agreement, and the maximum tolerated difference (green line). (a) The differences of systolic BP between oscillographic device and reference group. (b) The differences of diastolic BP differences between oscillographic device and reference group. (c) The differences of systolic BP differences between pulse wave device and reference group. (d) The differences of diastolic BP differences between pulse wave device and reference group.
Table 2 showed the bias, precision, and accuracy of BP for the oscillographic/reference and pulse wave/reference groups. The bias and precision in both systolic and diastolic BP were significantly less in pulse wave/reference (a bias of 1.8 and 0.77 mmHg and a precision of 5.20 and 4.66 mmHg, respectively), with corresponding higher accuracy readings (98.51% for P10 in systolic BP and 85.64% for P5 in diastolic BP), which indicated that pulse wave device has a good concordance with mercury sphygmomanometry.
Bias, precision, and accuracy of blood pressure for different sphygmomanometry.

Reference group refers to mercury sphygmomanometer group.
Discussion
Noninvasive devices are important for BP measurements. 15 In the presence of AF, however, the variation in contractility, ventricular filling time, and stroke volume can increase beat-to-beat BP variability, thus affecting the accuracy of BP measurements using noninvasive devices. 16 Currently, some international guidelines do not have specific recommendations for BP measurement in patients with AF,13,17–19 while others recommended the use of a mercury sphygmomanometer for BP measurements in patients with AF,20–22 for which multiple measurements are required to ensure relative accuracy.20,22 Owing to the potential environmental pollution of mercury, mercury sphygmomanometer will be deprecated gradually, and has been recommended to be replaced by electronic devices.13,18,19 Thus, it is necessary to figure out the agreement of BP measurements using electronic devices in AF. In this study, we had two major findings. First, we found significant differences in diastolic and systolic BPs between the oscillometric device and mercury sphygmomanometer, while the pulse wave device had a good concordance with the mercury sphygmomanometer. Second, automated devices appeared to be more accurate in measuring systolic BP but not diastolic BP.
Similar to this study, previous studies also found significant differences in BP values obtained with oscillometric devices and mercury sphygmomanometer.23–25 In addition, a study conducted in China showed better accuracy of BP measurement in pulse wave devices than oscillometric ones in patients undergoing coronary angiography and children aged 3–12 years. 11 There are limited studies on the accuracy of BP measurements of the pulse wave devices in AF, however. In this study, we found that the pulse wave device had a distinct advantage over the oscillometric device in the accuracy of BP measurement in the Bland–Altman plot analysis, ICCs, or other metrics such as bias, precision, and accuracy. What’s more, from ICC analyses, we found that each device showed better agreement in systolic BP than its diastolic BP, reflecting a better accuracy in systolic BP than diastolic BP in noninvasive devices. AF and arterial hypertension frequently coexist; clinically, hypertension in most elderly patients with AF is systolic hypertension. Therefore, for the elderly with AF, automatic devices may be applicable to perform BP measurements. 26
There are some limitations in this study. First, the reference group in this study was the mercury sphygmomanometer, which is the gold standard for noninvasive BP measurements, but its accuracy has been questioned in patients with AF. In this study, however, invasive BP is difficult to obtain in people with a nonsevere illness. Recent guidelines recommended the use of manual auscultatory methods for BP measurements in patients with AF.20–22 Second, we did not perform a third measurement in this study, only two readings of BP maybe not enough to reflect the true BP value. In this study, however, we aimed to perform in ‘real clinical practice’ to compare the accuracy, precision, and bias between the two automated devices and mercury sphygmomanometers when BP was measured twice. Third, the heart rates measured in this study were primarily in the normal ranges, with only a few participants had elevated heart rates greater than 100 beats per minute. Future studies should include patients with heart rates in the abnormal ranges to test device performance in that situation. Fourth, this study’s subjects were limited to only elderly patients to perform the comparison of noninvasive BP devices, which cannot be generalized to AF patients in all age categories. Thus, in future studies, patients of a younger age should be included to further explore the issue. Finally, the performance of automated devices in AF may differ per brand, model, and so on; thus, our results cannot be extended to apply to other oscillometric or pulse wave techniques in general. Further studies are needed to confirm our findings using other manufacturers’ devices.
Conclusion
A novel noninvasive sphygmomanometer – pulse wave sphygmomanometer has a good concordance with a mercury sphygmomanometer in BP values monitoring and may be applicable to BP measurements in elderly with AF.