
Abstract
Anticoagulation is vital for stroke and systemic embolism prevention in patients with atrial fibrillation. Current therapy with the vitamin K inhibitor warfarin has many inherent limitations in clinical practice. With the potential of broadening anticoagulation therapy to a larger population, new classes of anticoagulants have recently emerged with the potential for improved efficacy, safety and convenience. Direct thrombin inhibitor and Factor Xa inhibitor classes are showing promise for both patients and clinicians.
Introduction
The incidence of atrial fibrillation, the most common cardiac arrhythmia, is increasing [Singer et al. 2008], especially with the rapid expansion of the elderly population. Although the cause of nonvalvular atrial fibrillation is multifactorial, the serious sequelae remain the same: stroke and death. With a 23.5% attributable risk of stroke at age 80–89 years, the elderly with atrial fibrillation are at the highest risk of stroke and death [Lin et al. 1996].
Anticoagulant therapy has proven benefits in decreasing stroke risk in patients with nonvalvular atrial fibrillation [Hart et al. 1999], but it has inherent risks. For atrial fibrillation, adequate therapy with the vitamin K antagonist warfarin is challenging, as warfarin has a difficult therapeutic range to maintain due to its variable pharmacodynamics from medication interactions and diet. Owing to the high-risk profile of warfarin and difficulty of management, only approximately half of those patients with nonvalvular atrial fibrillation who should be anticoagulated are anticoagulated [Connolly et al. 2007]. To compound this undertreatment, of those patients’ eligible and anticoagulated with warfarin, analysis shows that such patients are only in the therapeutic range approximately 50% of the time, and in order to obtain maximum benefit, patients must have a minimum threshold of time in the therapeutic range of at least 60% [Connolly et al. 2008].
Warfarin has been the mainstay anticoagulant for over half a century. Its efficacy in the prevention of stroke in patients with atrial fibrillation has been well validated. Its limitations, however, have stimulated the search for new oral anticoagulants. In this review we summarize and evaluate several new classes of oral anticoagulants, with a focus on the direct thrombin inhibitors and Factor Xa inhibitors which are furthest along in development.
Direct thrombin inhibitors
Oral direct thrombin inhibitors are small molecules that bind specifically to the active enzymatic site of either free or clot-bound Factor IIa (thrombin) [Cabral et al. 2010]. Thrombin’s major function is to convert fibrinogen to fibrin. It also plays important positive feedback roles by activating coagulation factors upstream and initiating platelet aggregation. Alternatively, it has negative feedback roles by activating the protein C system and inhibiting fibrinolysis. The first oral direct thrombin inhibitor, ximelagatran, was studied for stroke prevention in atrial fibrillation in two large phase III studies (SPORTIF III and V) and showed noninferiority to warfarin [Olsson, 2003]. Despite development being stopped due to hepatic toxicity, ximelagatran proved the utility of direct thrombin inhibitors as viable therapeutic agents for stroke prevention in atrial fibrillation.
The US Food and Drug Administration (FDA) recently approved the direct thrombin inhibitor, dabigatran etexilate, for stroke prevention in patients with atrial fibrillation. Dabigatran etexilate is a prodrug that is converted to the active anticoagulant, dabigatran, by blood esterases (Table 1). It has an absolute bioavailability of 6.5%, is excreted 80% unchanged by the kidney, and is not metabolized by the liver, thus not interacting with the cytochrome P450 system. It does, however, act as substrate in the P-glycoprotein transport system and may potentially be affected by P-glycoprotein inhibitors or inducers [Yasuda et al. 2002]. Dabigatran has a serum half-life of 12–17 hours depending on renal function. It is administered twice daily and does not require regular monitoring [Stangier, 2008]. The sentinel phase III clinical study of dabigatran, the Randomized Evaluation of Long-term anticoagulation therapY (RE-LY), evaluated patients with nonvalvular atrial fibrillation at moderate to high risk of stroke or systemic embolism [Connolly et al. 2009]. In this multicenter, prospective, randomized trial, 18,113 patients were enrolled into three treatment groups: blinded dabigatran 110 or 150 mg twice daily versus open-label warfarin, with a goal International Normalized Ratio (INR) of 2.0–3.0 measured at least monthly. Exclusion criteria included depressed renal function with a creatinine clearance at or below 30 ml/min, active liver disease, history of heart valve disease, stroke within 14 days or a severe stroke within the past 6 months, conditions causing an increased risk of bleeding, and pregnancy. Inclusion criteria included electrocardiographic evidence of atrial fibrillation within the past 6 months and either a left ventricular ejection fraction less than 40%, New York Heart Association class II or higher, heart failure symptoms within the past 6 months, or previous stroke or transient ischemic attack.
Overview of salient pharmacokinetic and other parameters of Factor IIa and Xa inhibitors compared with warfarin.
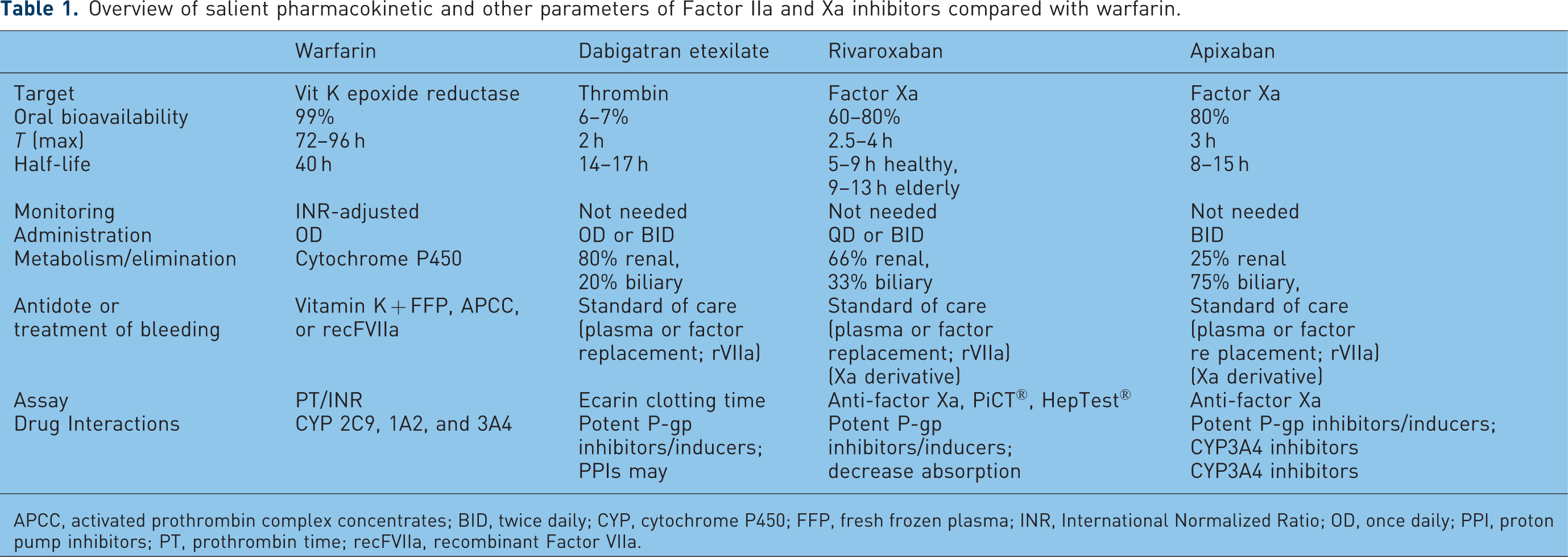
APCC, activated prothrombin complex concentrates; BID, twice daily; CYP, cytochrome P450; FFP, fresh frozen plasma; INR, International Normalized Ratio; OD, once daily; PPI, proton pump inhibitors; PT, prothrombin time; recFVIIa, recombinant Factor VIIa.
The primary outcome of the RE-LY trial was stroke or systemic embolism with secondary outcomes of stroke, systemic embolism and death. Analysis was performed to satisfy the noninferiority hypothesis that dabigatran was noninferior to warfarin. Of the over 18,000 patients enrolled for 2 years, the mean age was 71 years, 63.6% were male, and all had a mean CHADS2 score (clinical predictor scoring scheme based on congestive heart failure, hypertension, age >75 years, diabetes mellitus, and prior stroke) of approximately 2.1 (Table 2). About 20% of all patients were on low-dose aspirin (<100 mg daily). The warfarin arm was relatively well managed with a mean time in the therapeutic range of 64%. With regard to the study’s primary outcome of stroke or systemic embolism, the 110 mg dose of dabigatran proved to be noninferior to warfarin (1.53% versus 1.69%; relative risk [RR] 0.91; 95% confidence interval [CI] 0.74–1.11), while the 150 mg dose proved to be superior (1.11% versus 1.69%; RR 66; 95% CI 0.53–0.82; p < 0.001) (Figure 1). Major bleeding occurred significantly less with dabigatran 110 mg compared with warfarin (2.71% versus 3.36%; 95% CI 0.69–0.93; p = 0.003) and the 150 mg dose was noninferior to warfarin (3.11% versus 3.36%; 95% CI 0.81–1.07; p = 0.31) Of note, rates of intracranial hemorrhage were significantly reduced with both the 110 and 150 mg doses of dabigatran compared with warfarin (0.12% and 0.10% versus 0.38%, respectively).
Selected characteristics of the treatment groups in the RE-LY (Randomized Evaluation of Long-term anticoagulation therapY) trial.

ASA, acetylsalicylic acid; CHADS2, clinical predictor scoring scheme based on congestive heart failure, hypertension, age >75 years, diabetes mellitus, and prior stroke.

Primary efficacy and safety outcomes in Randomized Evaluation of Long-term anticoagulation therapy (RE-LY) trial.Dabig, dabigatran; ICH, intracerebral hemorrhage; Non Inf, noninferior; Sup, superior; Syst Emb, systemic embolism; warf, warfarin.
The RE-LY trial showed a slight increase in myocardial infarction in both dabigatran groups: 0.72% per year in the 110 mg group (RR 1.35; 95% CI 0.98–1.87; p = 0.07) and 0.74% per year in the 150 mg group (RR 1.38; 95% CI 1.00–1.91; p = 0.048) compared with 0.53% per year with warfarin. However, in a subsequent re-analysis of published data, several additional primary efficacy and safety outcome events were identified, thereby adjusting the incidence of myocardial infarction in the 110 mg group (RR 1.29; 95% CI 0.96–1.75; p = 0.09), and the 150 mg group (RR 1.27; 95% CI 0.94–1.71; p = 0.12) thus making the relative increase in myocardial infarction nonsignificant [Connolly et al. 2010b]. Patients taking dabigatran also experienced dyspepsia at a rate of approximately 11% versus roughly 6% for warfarin which is attributed to the acidic tartaric acid core of the tablet. Subsequent subgroup analyses from the RE-LY trial revealed similar results from patients who were warfarin naïve versus warfarin experienced [Diener et al. 2010]. This was also evident in patients with a previous transient ischemic attack or stroke versus those without, and for a number of other variables [Ezekowitz et al. 2010].
The RE-LY trial is the largest antithrombotic therapy randomized trial for stroke prevention in atrial fibrillation to date. It may lead to a substantial shift in the oral anticoagulant paradigm. The efficacy of dabigatran to prevent stroke versus warfarin is highly dependent on how well warfarin therapy is managed. The uncertainty of both efficacy and safety that has constrained appropriate antithrombotic therapy for stroke prevention with warfarin is potentially reduced with dabigatran. This has in turn opened a pipeline for new oral direct thrombin inhibitors in the wake warfarin therapy.
Factor Xa inhibitors
Inhibiting coagulation more upstream from direct thrombin inhibitors, oral Factor Xa inhibitors bind directly to the enzymatic pocket of activated Factor X, either free or located within the prothrombinase complex [Perzborn et al. 2010]. The Factor Xa inhibitor rivaroxaban is currently approved in Europe and Canada to prevent venous thromboembolism in the orthopedic patient population [Cabral et al. 2010]. It has predictable pharmacokinetics and does not require monitoring (Table 1). Maximal plasma concentrations are reached within 3.0–4.0 hours [Patel, 2010] and about one third is renally excreted unchanged, with two thirds metabolized by the liver partially through the cytochrome P450 system.
In 2010, the Rivaroxaban once daily Oral direct Factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) trial compared rivaroxaban 20 mg once daily and warfarin dose adjusted to an INR of 2.5 for thromboembolic prevention in nonvalvular atrial fibrillation (rivaroxaban 15 mg used for patients with a creatinine clearance of 30–49 ml/min) [Patel, 2010]. As with the RE-LY trial, the ROCKET AF trial’s primary endpoint was stroke and systemic embolism. Over 14,000 subjects enrolled with a mean CHADS2 score of approximately 3.5 for each group (Table 3). Over half of the subjects had a history of stroke and 62% fulfilled heart failure criteria. The time in therapeutic range in the warfarin arm was lower than in the RE-LY trial, at 57.8%. In the intention-to-treat analysis, non-inferiority to warfarin was achieved with the primary endpoint occurring in 2.12% of rivaroxaban patients versus 2.42% of warfarin patients (hazard ratio [HR] 0.88; CI 0.74–1.03; Figure 2). Rivaroxaban showed significantly decreased rates of hemorrhagic stroke at 0.26% versus 0.44% for the warfarin group (HR 0.58; CI 0.38–0.89), as was the case for dabigatran. It is interesting to note that although noninferiority was met, superiority was only met by an ‘on-treatment’ analysis. However, unlike the RE-LY trial, participants in the ROCKET AF trial were medically more complex.
Selected characteristics of the treatment groups in the ROCKET AF trial (Rivaroxaban once daily Oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation).

CHADS2, clinical predictor scoring scheme based on congestive heart failure, hypertension, age >75 years, diabetes mellitus, and prior stroke.

Primary efficacy and safety outcomes in the ROCKET trial.HR, hazard ratio; ICH, intracerebral hemorrhage; SE, systemic embolism.
There are several other oral Factor Xa inhibitors in the pipeline. Results from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial, anticipated this year, will compare oral apixaban 5 mg twice daily to warfarin with an INR goal of 2.0–3.0 [Lopes et al. 2010]. As with the RE-LY and ROCKET AF trials, ARISTOTLE is a double-blind, double-dummy, noninferiority trial with over 18,000 subjects with at least one risk factor for stroke enrolled. The Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment (AVERROES) trial, is a trial with apixaban versus aspirin in patients not considered candidates for treatment with a vitamin K antagonist or who refused vitamin K antagonist treatment. A total of 5599 patients were randomized to either apixaban 5 mg twice daily or aspirin 84–325 mg once daily [Connolly et al. 2011] (Table 4). The primary outcome of stroke or systemic embolism was 1.6% per year for the apixaban group and 3.7% per year for the aspirin group (HR 0.45; CI 0.32–0.62; p < 0.001; Figure 3). Although the rates of death were not statistically different between the two groups, 3.5% per year for the apixaban group versus 4.4% for the aspirin group (HR 0.79; CI 0.62–1.02; p = 0.07), a significant reduction in cardiovascular hospitalizations was observed in the apixaban group. Rates of major bleeding were not significantly increased in the apixaban group versus the aspirin group at 1.4% per year and 1.2% per year, respectively (HR 1.13; CI 0.74–1.75; p = 0.57). This study targeted patients who were considered unsuitable for vitamin K antagonist therapy thereby suggesting new alternative therapy with apixaban as a potential safe alternative.
Selected characteristics of the treatment groups in the AVERROES (Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment) trial.

ASA, acetylsalicylic acid; CHADS2, clinical predictor scoring scheme based on congestive heart failure, hypertension, age >75 years, diabetes mellitus, and prior stroke; TIA, transient ischemic attack; CHF, congestive heart failure.

Primary efficacy and safety outcomes in the AVERROES trial.ICH, intracerebral hemorrhage; NS, not significant; Syst Emb, systemic embolism.
A third inhibitor of Factor Xa, Endoxaban (DU-176b), is currently under phase III investigation in the Evaluation of the novel Factor Xa inhibitor endoxaban compared with warfarin in patients with atrial fibrillation Design and rationale for the Effective aNticoaGulation with Factor xA next Generation in Atrial Fibrillation-Thrombolysis In Myocardial Infarction study 48 (ENGAGE AF-TIMI 48) trial [Ruff et al. 2010]. The dose finding phase II trial on endoxaban was a randomized, parallel group, multicenter, international study of 1146 patients with nonvalvular atrial fibrillation with a minimum CHADS2 score of at least 2. The study compared the safety of four fixed-dose regimens of endoxaban (30 mg once daily, 30 mg twice daily, 60 mg once daily, or 60 mg twice daily) with open-label warfarin; the primary safety outcome measures being major bleeding and secondary outcomes of major cardiovascular events. This 12-week study suggested doses of 30 or 60 mg once daily had similar or less bleeding rates versus warfarin. Rates of bleeding were significantly higher with twice daily dosing than once daily dosing [Weitz et al. 2010]. Thus, edoxaban 30 mg and 60 mg once daily will be compared with warfarin for the prevention of stroke and systemic embolism in the ENGAGE AF-TIMI 48 phase III trial. Over 20,000 participants in this randomized, double-blind, double-dummy trial, with diagnosed nonvalvular atrial fibrillation and a CHADS2 score at or greater than 2 were assigned to either the endoxaban 30 mg, endoxaban 60 mg, or the warfarin arm with a goal INR 2.0–3.0. The outcome of the phase III study will be forthcoming in the near future.
Another promising Factor Xa inhibitor, betrixaban, is under phase II investigation [Connolly et al. 2010a]. The randomized, parallel group phase II EXPLORE-Xa trial studied over 500 patients with nonvalvular atrial fibrillation with a mean CHADS2 score of 2.2 with three blinded doses of betrixaban (40, 60, or 80 mg once daily) versus open-label warfarin. Primary endpoints were major bleeding, with secondary endpoints of major cardiovascular events. Initial results suggest major bleeding and incidence of stroke at 60 and 80 mg does to be comparable to that of warfarin. Betrixaban has minimal renal excretion and a half-life of 20–24 hours. Further larger clinical trials are needed to evaluate both efficacy and safety of betrixaban.
Reversibility and drug interactions
The short half-life of these inhibitors relative to warfarin is beneficial when discontinuation of anticoagulation is needed. Emergent reversibility, however, is a limitation. Although no specific reversal agent is currently available, prothrombin complex concentrates, fresh frozen plasma, and recombinant Factor VIIa are empiric emergent reversal therapies currently available.
Drug interactions with Factor IIa inhibitors are currently limited to only the P-glycoprotein system. Most interactions with substrates of the P-glycoprotein system, including atorvastatin and digoxin have not shown significant effects, with interactions appreciated only with the P-glycoprotein inducer, rifampin [Walenga and Adiquzel, 2010]. Strong inhibitors of the CYP3A4 and P-glycoprotein system, such as azole antimycotics and protease inhibitors reduce clearance of rivaroxaban and are thus not recommended [Perzborn et al. 2010]. Perceptibly, inducers of the CYP3A4 system may reduce plasma levels of rivaroxaban. Co-administration of rivaroxaban with other CYP3A4 substrates including atorvastatin and midazolam revealed no significant interactions, as did co-administration with P-glycoprotein substrate digoxin. Pharmacokinetic changes were appreciated when P-glycoprotein inhibitors such as verpamil, clarithromycin, quinidine and amiodarone were co-administered with dabigatran, however were not significant to change dosing recommendations [Cabral et al. 2010].
Conclusion
Clinicians have turned to warfarin for decades. Over the years, the vitamin K antagonists have achieved a significant decrease of new strokes in patients with nonvalvular atrial fibrillation. Warfarin is a relatively inexpensive and widely available drug that has a well-understood pharmacodynamic profile. The pharmacokinetics of warfarin therapy, however, brings to light many limitations in practice. Maintaining a narrow therapeutic window and the need for constant, lifelong monitoring is challenging. An adequate time to therapeutic range is very difficult, with many patients achieving this less than 60% of the time [Baker et al. 2009]. These aforementioned restraints lead to many patients with nonvalvular atrial fibrillation not being effectively anticoagulated with warfarin. New oral anticoagulants, by directly inhibiting sentinel parts of the coagulation cascade, are a promising and emerging new therapy. Both Factor IIa and Factor Xa inhibitors demonstrate ease of dosing, monitoring, and more favorable pharmacokinetics and pharmacodynamics. Given their lower risk profile, the new oral anticoagulants can be used in patients who cannot tolerate or are not favorable candidates for warfarin therapy. Further, the scope of utilization can be broadened to incorporate more patients at moderate risk for stroke. New risk stratification schemes are being investigated with the advent of new anticoagulants to appropriately incorporate more at risk populations without the restrains of warfarin therapy.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
J. Ansell is a consultant for Boehringer Ingelheim, Ortho McNeil, Bristol Myers Squibb, Daiichi Sankyo; DSMB Chair for a number of studies by Bristol Myers Squibb; Executive Steering Committee for ARISTOTLE study.