
Abstract
Background:
Osteoporosis increases the risk of fractures. Visceral fat is associated with cardiovascular disease (CVD). There is inadequate knowledge on the relationship between osteoporosis and visceral fat. The study aimed to evaluate the relationship between bone mineral density (BMD) and visceral fat mass in the elderly.
Methods:
This was a prospective cohort study. Subjects were enrolled from the Rheumatology Clinic. All subjects underwent baseline bone mineral density and body composition measurements using dual-energy X-ray absorptiometry.
Results:
A total of 321 patients including 288 females and 33 males were enrolled in this study. We followed up DEXA for 1 year for fat and muscle mass change and found that 162 (50.5%) had a decrease in fat mass, 129 (40.2%) had decreased visceral fat, and 138 (43%) had decreased muscle mass. Furthermore, we found that the baseline hip T score was correlated with visceral fat decrease. Using visceral fat decrease as the outcome, we found that hip T score could predict visceral fat loss: the higher the T score, the more visceral fat loss was found [p < 0.001, OR: 1.6, CI: (1.3–2.1)].
Conclusion:
A high hip T score was associated with a future decrease in visceral fat, which may decrease the risk of atherosclerosis and CV risk. Therefore, evaluation of visceral fat may be useful for assessing CVD risk in patients with osteoporosis. Effective management of the risk of atherosclerosis and CVD is important in improving the life expectancy of these patients.
Introduction
Osteoporosis is characterized by low bone mineral density (BMD) and deterioration of the bone microarchitecture. It leads to bone fragility and increases the risk of fractures 1 and comorbidities, such as hypertension, deficiency anemias, and fluid and electrolyte imbalances. 2
Visceral fat is associated with diabetes, hypertension, dyslipidemia, atherosclerosis, and cardiovascular disease (CVD).3,4 Patients with an increase in visceral fat mass had an increased overall risk of atherosclerosis when assessed by carotid intima–media thickness and plaque score. 5 Furthermore, visceral fat predisposes patients to sarcopenia 6 and increases the risk of CVD. 7 The role of visceral adiposity in CVD activity and CV outcomes has been studied in rheumatoid arthritis (RA) patients.5,8–10 Studies have revealed that a decrease in visceral fat leads to a decrease in the risk of CVD. 11
Loss of visceral fat might be of great importance in preventing CVD. Visceral adiposity can be decreased with various interventions, such as diet, exercise, drugs, and bariatric surgery.12–17 Therefore, workup for visceral fat is an important issue.
The problem of visceral adiposity is more common in the older age group, which poses a public health issue. In addition, there is inadequate knowledge on the relationship between osteoporosis and visceral fat. The prevalence of both conditions necessitates an attempt to understand the association between them. Furthermore, the role of BMD in visceral fat decrease is not fully understood.
This study aimed to evaluate BMD, fat mass, and visceral fat mass in elderly people. The main objectives of this study were (1) to find out the association between BMD, fat mass, and visceral fat decrease, and (2) to determine whether BMD plays a role in fat mass decrease.
Materials and methods
Study population and design
This interim analysis of osteoporosis/sarcopenia was conducted at Chang Gung Memorial Hospital, Kaohsiung (CGMHK). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 18 In the registry, patients who had visited the Rheumatology Clinic and wanted to accept BMD and body composition evaluation at CGMHK since 1 September 2018 to 31 December 2020. Those who were less than 50 years of age, had any cancer history in the past 5 years, had an estimated life expectancy less than 3 years, or could not cooperate in the study were excluded from the program.
Clinical evaluation included demographic data [height, weight, age, body mass index (BMI)]; comorbidities; duration of disease; daily physical activities; and history of cigarette, alcohol, and smoking consumption. We collected data about current medications including anti-osteoporotic drugs at the time of registration. In addition, previous fragility fractures and lifestyle were also recorded. The participants provided written informed consent and the CGMHK Ethical Review Board approved the study (104-3530B), which was under the principles of the Helsinki Declaration.
Sample size calculation
GPower, version 3.1.2 is used to determine the minimal required sample size with an alpha level of 0.05 (5%), power of 0.95 (95%), 10 predictors, and 0.085 partial R2; the minimal required sample size is 142 patients.
Measurement of body composition and BMD
BMD (g/cm2) of the proximal femur (total hip and femoral neck) and fat mass (kg), visceral adipose tissue, and muscle mass were assessed using dual-energy X-ray absorptiometry (DEXA; Hologic QDR Discovery Wi; software version 12.0). The examinations were performed by trained technicians who were blinded to the participant group. The coefficients of the DEXA measures were 1–1.5%. 19 We followed fat mass, visceral adipose tissue, and muscle mass at baseline and 1 year later.
Statistical analysis
Statistical analysis was performed using SPSS software (version 24.0; SPSS, Chicago, IL, USA). Patient characteristics were reported as simple descriptive statistics [medians and IQR (interquartile range)]. The relationships between categorical variables were evaluated using the chi-square test. Correlation between variables was performed using Pearson’s correlation test. Logistic regression analysis was used to adjust for potential confounding factors, and statistical significance was set at p < 0.05.
Results
A total of 321 patients were enrolled in this study. There were 288 females and 33 males. The median age was 68 years (IQR: 59–78), with 66 years (IQR: 58–75) for males and 69 years (IQR: 60–78) for females. The median BMI was 23.1 kg/m2 (IQR: 21.1–25.0). There were 81% of patients who accepted anti-osteoporotic therapy including alendronate, zolendronic acid, and denosumab, so the T scores were higher. Of the patients, 15% had diabetes, 34.6% had hypertension, and 56.1% had RA. The median total hip T score was –1.2 (IQR: –2.2, –0.5), the median femoral neck T score was –2.4 (IQR: –3.1, –1.2), the median fat mass/height2 was 8.44 (IQR: 7.22, 10.10), the median visceral adipose tissue mass was 541.0 (IQR: 373.0, 748.0), and the median muscle mass/height2 was 5.41 (IQR: 4.76, 5.77). We also found the median decreased fat mass/height2 was 0 (IQR: –0.3, 0.74), the median decreased visceral adipose tissue mass was 27 (IQR: –59, 136), and the median decreased muscle mass/height2 was 0.09 (IQR: –0.09, 0.34). We followed up DEXA for 1 year for fat and muscle mass change and found that 162 (50.5%) had a decrease in fat mass, 129 (40.2%) had decreased visceral fat (female had 39.6% decrease in visceral fat, while male had 45.5% decrease in visceral fat.), and 138 (43%) had decreased muscle mass. (Table 1). In addition, we found that the baseline hip T score was correlated with visceral fat decrease (P < 0.005), not total fat mass decrease (Table 2), and those with high baseline total hip T score had more decrease in visceral adipose fat, as shown in Figure 1. We found physical activities were the same between those with or without visceral adipose decrease. Using visceral fat decrease as an outcome, we found that the hip T score can predict visceral fat loss: the higher the T score, the more visceral fat loss was found [p < 0.001, odds ratio (OR): 1.6, confidence interval (CI): (1.3–2.1)] (Table 3).
Baseline demographic and clinical characteristics of the patients.

IQR, interquartile range.
Correlation of hip T score with the variables.
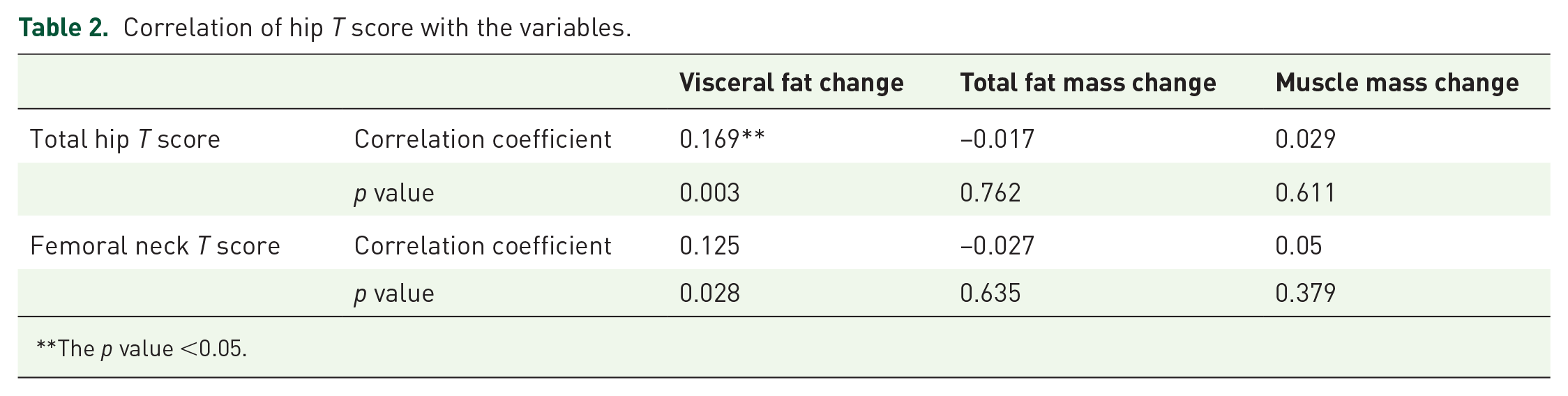
The p value <0.05.

The correlation between total hip T score and changes in visceral adipose tissue after 1 year. We found high T score had more decrease in visceral adipose tissue.
Multiple variable analysis of the risk of visceral fat loss.

CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
Our evaluation of the association between hip T score and the decrease in fat mass, visceral adiposity, and muscle mass revealed a higher association of hip T score with visceral adipose decrease, but not with total fat mass and muscle mass changes. There was a mean visceral adipose increase in those with lower T score; in this registry 61% of the patients had T score below normal (T score <–1), so most of these patients also had increased visceral adipose. Therefore, hip T score is an important factor associated with visceral fat change. As visceral fat is a factor that determines atherosclerosis and CV risk, improvement in visceral fat is important to decrease atherosclerosis and the future CVD risk. 11 Therefore, a higher T score tends to have a future decrease in visceral fat. Does this mean a high T score is associated with a lower risk of CVD? A literature review showed that risk of stroke was associated with low T score, 20 and it has also been found that heart failure often occurs in patients with low femoral BMD. 21 Another report revealed an association between hip BMD and aortic valvular, aortic annular, and mitral annular calcification. 22 In an elderly group, hip BMD was found to be related to subclinical atherosclerotic disease. 23 Therefore, a high T score was associated with a lower risk of CV events. Second, in this study, high hip T score was correlated with visceral fat decrease, but not total fat mass decrease; so, we hypothesized that the main reason for atherosclerosis and CV risk may be visceral fat, and total fat cannot be used as a parameter for future CV risk.
Although the association between adiposity and the risk of atherosclerosis has been reported, visceral fat mass was higher in patients with RA than in a control group.24,25 In another study on RA in Japan, visceral adiposity was found to be an independent predictor of atherosclerosis. 5
Femoral BMD is known to be a predictor of hip fractures, 26 and it can be improved after treatment with zoledronate. 27 Therefore, hip BMD can be used to predict not only the risk of future fractures but also visceral fat change and the related atherosclerosis and CVD.
Although low BMD is associated with low muscle mass, 28 in this study it cannot be used to predict muscle mass changes. Therefore, hip BMD tended to have no connection with changes in muscle density.
It has been reported that visceral adipose tissue can release some adipokines, 29 including tumor necrosis factor (TNF)-α, interleukin (IL)-6, IL-1β, leptin, adiponectin, and resistin, which can lead to inflammation and atherogenesis, and increase the risk of CV. 29 Among them, adiponectin levels were low in obese patients. 30 Adiponectin is also known to exert anti-inflammatory and CV modulating effects. 31 Therefore, adiponectin may have the potential to reduce obesity and its related diseases. 32 Dietary intervention strategies and associated weight loss have been reported to increase adiponectin levels. Further research is needed to investigate the benefits of adiponectin in high CVD risk groups.33–36 More research is also needed to elucidate the potential pathways for increasing adiponectin levels in visceral fat deposition in patients with low hip BMD.
The limitations of our study included the use of DEXA rather than the gold standard abdominal computed tomography (CT) for the measurement of visceral fat mass. In addition, this was a single-center study and that limits its generalization. Furthermore, it was not a randomized control study and that introduced the risk of selection bias, which could have affected the study results. Third, this study did not examine the effects of medications, lifestyle, dietary intake, and physical activity. Fourth, the small sample size was insufficient to make definitive conclusions. Fifth, half of the patients had RA; however, RA disease activity and concomitant disease-modifying anti-rheumatic drugs and biological agents were not evaluated, and these may have affected the results of this study. Despite these limitations, we believe that our findings adequately reflect patients in typical rheumatology clinical practice. To the best of our knowledge, this is the first study to examine the correlation between hip BMD and visceral fat changes.
Conclusion
A high hip T score was associated with a future decrease in visceral fat, which may decrease the risk of atherosclerotic plaques and CVD risk in patients. Therefore, evaluation of visceral fat may be useful in assessing CVD risk in patients with osteoporosis. Effective management of the risk of atherosclerosis and CVD events in those with a low T score of the hip is important in improving the life expectancy of these patients.
Footnotes
Acknowledgements
We are indebted to the Special Interest Group of Osteoporosis in the Taiwan College of Rheumatology and the Taiwan Bone Muscle Joint Total Care Association for instructing the progression of this study. We also appreciate the assistance provided by the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital.