
Abstract
Background:
Bisphosphonates are a type of medication that prevents the loss of bone density. Secondary childhood osteoporosis reduces bone strength and results in an increased risk of fragility fracture. This meta-analysis aims to explore the efficacy and safety of bisphosphonates on secondary childhood osteoporosis.
Methods:
We performed a systematic search of PubMed, Cochrane library, and Web of Science databases up to 31 July 2022 to screen for random clinical trials (RCTs) on bisphosphonate treatment for childhood secondary osteoporosis. Data from selected studies, mainly changes in lumbar spine (LS) bone mineral density (BMD), changes in LS BMD Z-scores, fracture events, and adverse events (AEs), were extracted and analyzed.
Results:
Nine RCTs (n = 429 in total) were included in our meta-analysis. The meta-analysis indicated that bisphosphonates improved the changes in LS BMD [mean difference (MD) = 0.04, 95% confidence intervals (CIs) = 0.01–0.07, p < 0.01] and LS BMD Z-scores [MD = 0.52, 95% CI = 0.23–0.81, p < 0.01]. Use of bisphosphonates did not increase the risk of AEs [odds ratio (OR) = 1.61, 95% CI = 0.87–2.99, p = 0.13]. Subgroup analysis showed that routes of administration, but not causes of secondary osteoporosis, might influence the efficacy of bisphosphonates. IV bisphosphonates close to significantly improved the incidence of fracture (OR = 0.34, 95% CI: 0.11–1.08, p = 0.07).
Conclusions:
The use of bisphosphonates improves LS BMD without increasing AE rates, which supports the clinical use of bisphosphonates in secondary childhood osteoporosis. Further large RCTs are still warranted, especially for their long-term effects on fracture rates.
Introduction
Osteoporosis is a metabolic bone disease characterized by low bone mass and microarchitectural deterioration of bone tissue. Osteoporosis is generally divided into primary and secondary osteoporosis. 1 Osteoporosis in children is usually secondary osteoporosis, which is caused by chronic illness or its treatment, especially the use of steroids. 2 Secondary osteoporosis in childhood reduces bone strength and results in an increased risk of fragility fractures.
Bisphosphonates are a type of medication that prevents the loss of bone density, and hence are widely used to treat osteoporosis. 3 With regard to secondary osteoporosis in children, a previous Cochrane review in 2007 4 includes six random clinical trials (RCTs), two controlled clinical trials, and one prospective cohort, but the heterogeneity among these included studies precluded statistically combining the results. This Cochrane review 4 concludes that short-term (3 years or less) bisphosphonate use appears to be well-tolerated, but its efficacy still needs further evaluation. Since then, an increased number of RCTs have been conducted to evaluate the efficacy and safety of bisphosphonate therapy for secondary osteoporosis in children. However, the evidence for bisphosphonate therapy in secondary childhood osteoporosis remains inadequate. Thus, here we conducted a meta-analysis to evaluate the efficacy and safety of bisphosphonate therapy in children with secondary osteoporosis.
Materials and methods
This meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. The protocol was registered in PROSPERO (registration number: CRD42022309845). Because the current research was based on the published data, no consent statement and ethical approval are required.
Searching strategy
Following the PRISMA guidelines, we searched the PubMed, Cochrane library, and Web of Science databases on 31 July 2022, using the following keywords: ‘osteoporosis’ AND (‘bisphosphonate’ OR ‘bisphosphonates’ OR ‘alendronate’ OR ‘clodronate’ OR ‘etidronate’ OR ‘ibandronate’ OR ‘olpadronate’ OR ‘risedronate’ OR ‘tiludronate’ OR ‘zoledronate’ OR ‘phosphoric acid’) AND (child OR child* OR pediatric OR adolescent OR juvenile). The detailed search strategy can be found in Supplementary Tables 1–3.
Inclusion and exclusion criteria
Inclusion criteria: (1) children or adolescents who suffered from osteoporosis secondary to chronic illness or its treatment; (2) treatment with bisphosphonates; (3) bone mineral density (BMD) should be measured by dual-energy X-ray absorptiometry (DEXA); (4) the study design should be RCT.
Exclusive criteria: (1) studies without controls or only self-control; (2) data were not available or were repeated; (3) reviews, editorials, single cases and case series, letters, and commentaries; (4) studies focused on primary osteoporosis; (5) studies focused on osteogenesis imperfecta.
Study selection
Two reviewers (H.Z. and Y.D.) independently reviewed studies to extract potentially eligible studies. Any disagreements regarding articles were resolved through discussion by all authors and resolved by consensus with the corresponding author (Z.X.).
Data extraction
The collected data included the author’s name, publication year, countries, sample size, participant characteristics (age and sex), secondary cause, intervention (drug type, mode of administration, drug dose), follow-up duration, and outcomes. To assess the efficacy, we collected the changes in lumbar spine (LS) BMD and LS BMD Z-score as the main outcomes and the incidence of fracture as a secondary outcome. To assess the safety, we collected the adverse events (AEs).
Quality assessment
Study quality was assessed using Cochrane’s Collaboration tool. 5 For each RCT, bias was estimated qualitatively by independent reviewers as low risk, unclear, or high risk, including items of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. In addition, to assess publication bias, funnel plots were performed.
Statistical analysis
The comprehensive meta-analysis was performed to calculate odds ratios (OR) or mean difference (MD) and their 95% confidence interval (CI) by RevMan 5. Statistical heterogeneity was assessed by Cochran’s Q statistic and the I2 statistic. I2 values of 25%, 50%, and 75% represent low, moderate, and high degrees of heterogeneity, respectively. Similar to our previous study, 6 a random-effects model (Mantel–Haenszel method for dichotomous data or inverse-variance method for continuous data) was employed for the meta-analysis because the included studies in the analysis are not functionally identical (especially the use of different kinds of bisphosphonates). For the sensitivity analysis, included studies were excluded one by one. Subgroup analyses according to the route of bisphosphonate administration [intravenous (IV) versus oral] and the cause of secondary osteoporosis (steroid-associated versus others) were also performed. P value <0.05 was revealed statistically significant.
Results
Study selection
The study selection process is depicted in Figure 1. Totally, 2155 potentially relevant articles were identified initially. Finally, nine RCTs (n = 429 in total) were included in our meta-analysis.7–15 Of note, we excluded three articles because of no available outcome data16–18 and another one article because of data not consistent with other studies 19 when assessing the full articles. The details of included studies are shown in Table 1.

Flow diagram of the study selection process.
Details of included studies.

25OHD, 25-hydroxyvitamin D; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMC, bone mineral content; BMD, bone mineral density; GGT, gamma glutamyl transferase; HIV, human immunodeficiency virus; iv., intravenous; M, month; NA, not available; po., per os, means oral; PTH, parathyroid hormone; SLE, systemic lupus erythematosus; VD, vitamin D.
Among the nine included RCTs, six trials8–13 used oral bisphosphonates, and the other three7,14,15 trials used IV bisphosphonates. Placebo was used for the control group in two RCTs.13,15 Calcium or calcium plus vitamin D were used in both control and bisphosphonate groups in eight RCTs.7–12,14,15 The follow-up duration was 12 months in six RCTs,8–10,12,13,15 3 months in one RCT, 11 18 months in one RCT, 7 and 24 months in the other one RCT. 14
Quality assessment
All trials were generally considered to have high quality according to criteria, despite a bias in allocation concealment and blinding of participants and personnel in the trial of Zacharin et al. 14 (Figure 2).
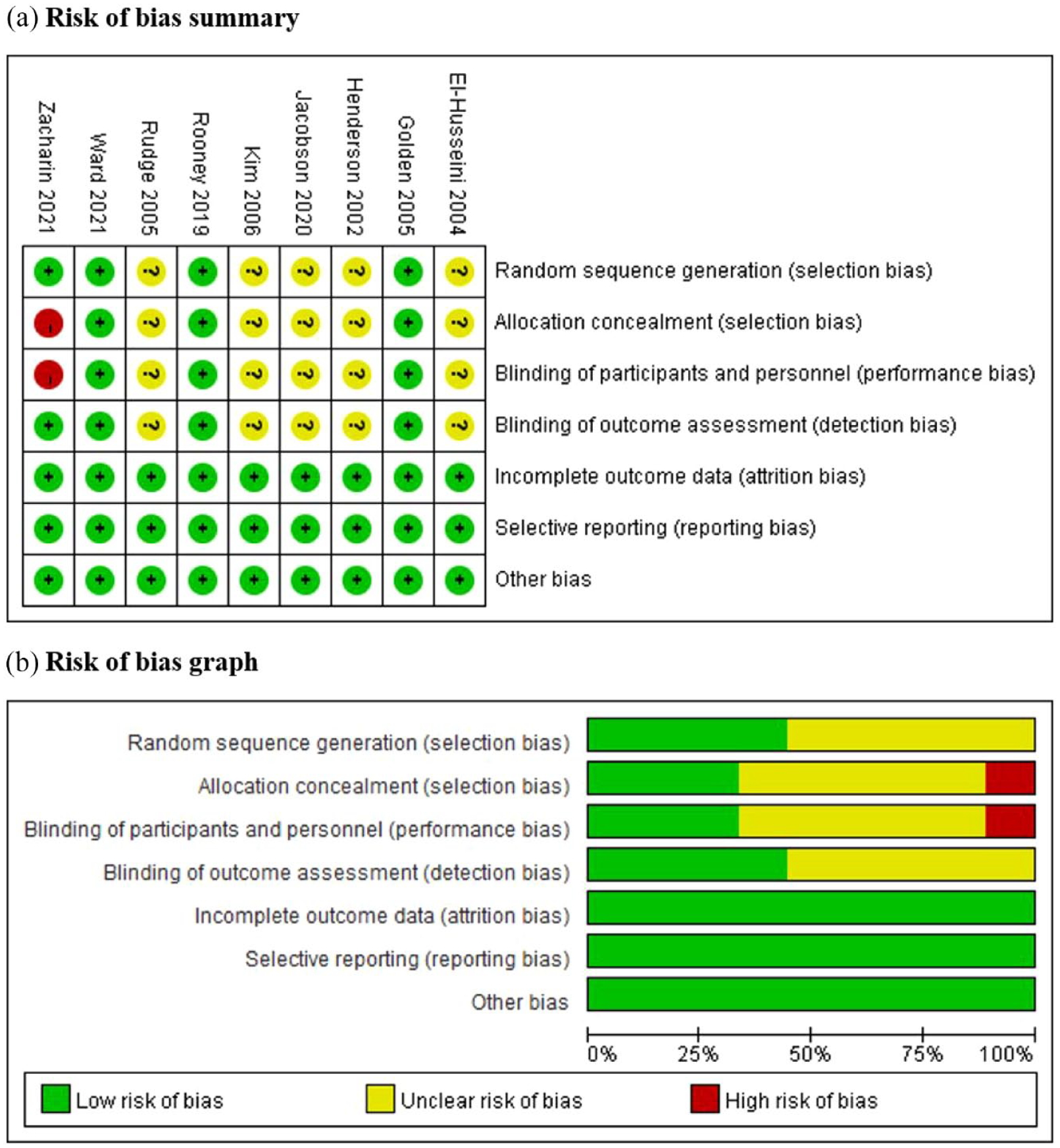
Risk of bias assessment: (a) assessments about each risk of bias item for each included study; (b) assessments about each risk of bias item were presented as percentages across all included studies.
Efficacy
Changes in LS BMD
Five included RCTs with a total of 303 individuals measured the changes in LS BMD.9,11–14 Among them, four RCTs9,11–13 used oral bisphosphonates and one RCT 14 used IV bisphosphonate. As shown in Figure 3, the meta-analysis showed that the changes in LS BMD in the bisphosphonate group were higher than those in the control group (MD = 0.04, 95% CI = 0.01–0.07, p < 0.01, I2 = 63%).

Forest plots indicating bisphosphonates improved the changes in LS BMD.
For the sensitivity analysis, five studies were excluded one by one (Supplementary Table 4). When the study of Rooney et al. 12 was excluded, the results became almost significant (MD = 0.05, 95% CI = 0.00–0.10, p = 0.05). When the rest of the studies were excluded by turns, the result remains significant. Of note, when the study of Zacharin et al. 14 (the only one RCT that used IV bisphosphonate) was removed, the I2 changed from 63% to 0% (but the results remain significant, MD = 0.03, 95% CI: 0.02–0.05, p < 0.0001, I2 = 0%). When the rest of the studies were excluded by turns, the I2 remains high (50–75%).
Changes in LS BMD Z-scores
Seven included RCTs with a total of 355 individuals that measured the changes in BMD Z-scores of the LS.7,9,10,12–15 Among these included RCTs, three RCTs7,14,15 used IV bisphosphonates and four RCTs9,10,12,13 used oral bisphosphonates. As shown in Figure 4, the meta-analysis showed that the changes in LS BMD Z-scores in the bisphosphonate groups were higher than those in the control groups (MD = 0.52, 95% CI = 0.23–0.81, p < 0.01, I2 = 86%).

Forest plots indicating bisphosphonates with different administration routes improved the LS BMD Z-scores.
Subgroup analysis according to the route of bisphosphonate administration (IV versus oral) showed that (1) IV bisphosphonates significantly improved the BMD Z-scores (MD = 0.86, 95% CI = 0.47–1.25, p < 0.001, I2 = 0%), while oral bisphosphonates almost significantly improved the BMD Z-scores (MD = 0.37, 95% CI = 0.00–0.73, p = 0.05, I2 = 92%; Figure 4); (2) the efficacy of IV bisphosphonates was close to significantly better than oral bisphosphonates (χ² = 3.23, p = 0.07, I2 = 69%; Figure 4).
Subgroup analysis according to the cause of secondary osteoporosis (steroid-associated versus others) showed that (1) bisphosphonates improved the BMD Z-scores in children with osteoporosis secondary to both causes (steroid-associated: MD = 0.52, 95% CI = 0.11–0.94, p = 0.01, I2 = 59%; others: MD = 0.52, 95% CI = 0.04–1.00, p = 0.04, I2 = 87%; Supplementary Figure 1); (2) the efficacy of bisphosphonates has no statistical difference between the two groups (χ² = 0.00, p = 0.99, I2 = 0).
For the sensitivity analysis, the result did not change significantly when studies were excluded one by one (Supplementary Table 4).
Fracture rate
Seven included RCTs with a total of 335 individuals measured fracture incidence.7–9,12–15 As shown in Figure 5, the meta-analysis showed that bisphosphonates did not affect the incidence of fracture significantly (OR = 0.71, 95% CI: 0.27–1.83, p = 0.48, I2 = 23%).
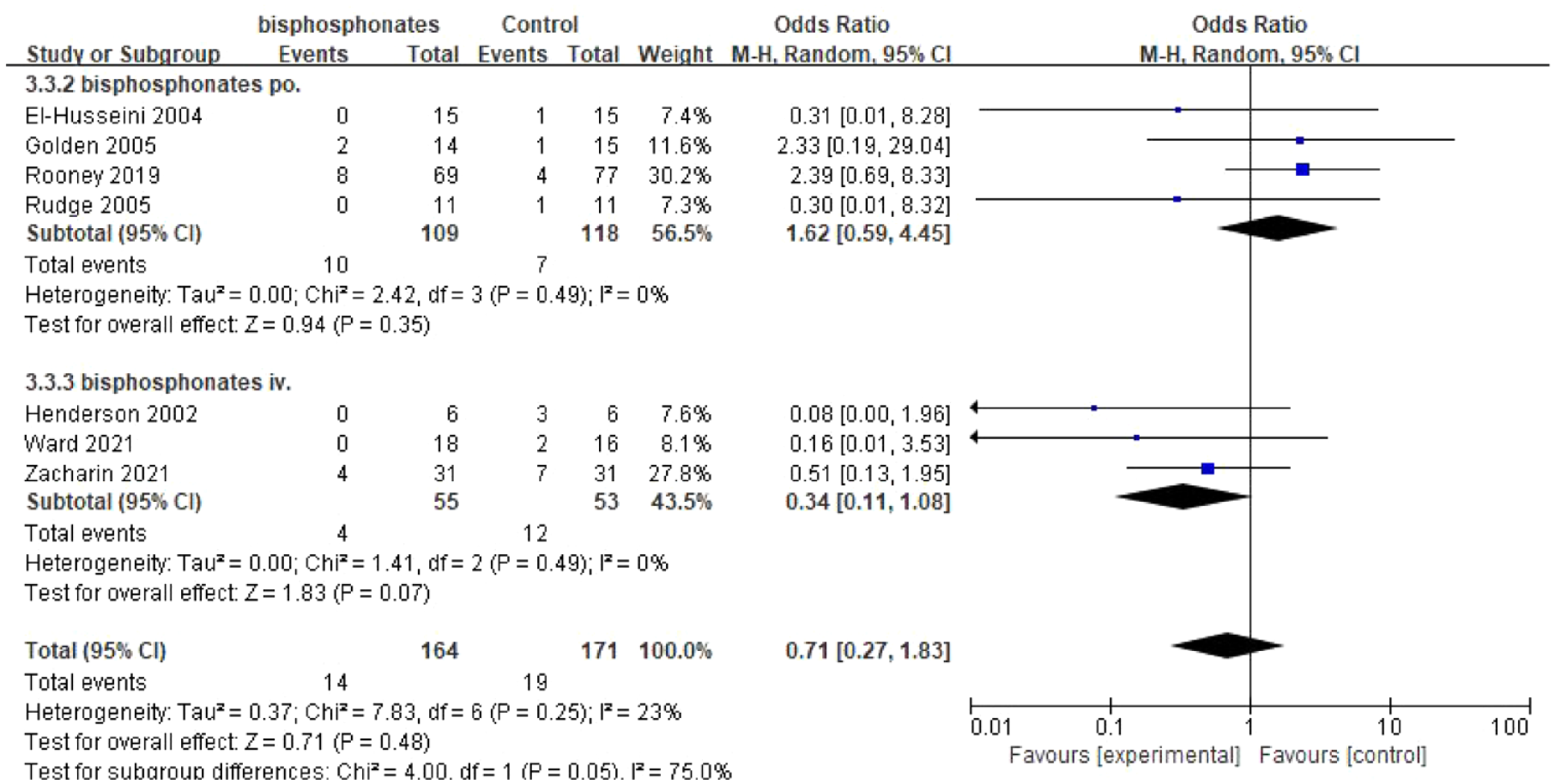
Forest plots of fracture.
Subgroup analysis according to the route of bisphosphonate administration (IV versus oral) further showed that (1) IV bisphosphonates close to significantly reduced the incidence of fracture (OR = 0.34, 95% CI: 0.11–1.08, p = 0.07, I2 = 0%; Figure 5); (2) the effect of IV bisphosphonates on reducing the incidence of fracture was almost significantly stronger than that of oral bisphosphonates (χ² = 4.00, p = 0.05, I2 = 75%; Figure 5).
Subgroup analysis according to the cause of secondary osteoporosis (steroid-associated versus others) showed that bisphosphonates did not affect the incidence of fracture significantly in both groups (steroid-associated: OR = 0.76, 95% CI = 0.28–2.08, p = 0.59, I2 = 21%; others: OR = 0.49, 95% CI = 0.02–14.11, p = 0.68, I2 = 63%; Supplementary Figure 2).
For the sensitivity analysis, the result did not change significantly when studies were excluded one by one (Supplementary Table 4). The result also did not change significantly when the trial of Zacharin et al. 14 was removed (OR = 0.71, 95% CI: 0.20–2.47, p = 0.59, I2 = 30%).
Safety
Seven included trials reported AEs, and a total of 173 out of 363 patients experienced at least one kind of AE.7–10,12,14,15 Among these included RCTs, four RCTs8–10,12 used oral bisphosphonates and the other three RCTs7,14,15 used IV bisphosphonates. As shown in Figure 6, the meta-analysis showed that bisphosphonates did not increase the total AE rate significantly (OR = 1.61, 95% CI: 0.87–2.99, p = 0.13, I2 = 0%).

Forest plots indicating bisphosphonates did not increase the risk of AEs.
Subgroup analysis showed the AE rate was not significantly affected by the routes of bisphosphonate administration (IV bisphosphonates: OR = 1.45, 95% CI = 0.71–2.96, p = 0.31, I2 = 0%; oral bisphosphonates: OR = 2.44, 95% CI = 0.51–11.60, p = 0.26, I2 = 33%; Figure 6) or the cause of secondary osteoporosis (steroid-associated: OR = 1.86, 95% CI = 0.85–4.11, p = 0.12, I2 = 5%; others: OR = 1.22, 95% CI = 0.38–3.87, p = 0.74, I2 = 0%; Supplementary Figure 3). The details of the AEs are described in Table 2.
Details of adverse events.

AEs, adverse events; B, bisphosphonate group; C, control group.
Study that did not report detailed AEs.
For the sensitivity analysis, the result did not change significantly when studies were excluded one by one (Supplementary Table 4).
Publication bias
According to Figure 7, no significant publication bias was found among these included studies evaluating the LS BMD (Figure 7(a)), LS BMD Z-scores (Figure 7(b)), fracture rate (Figure 7(c)), and AE rate (Figure 7(d)).
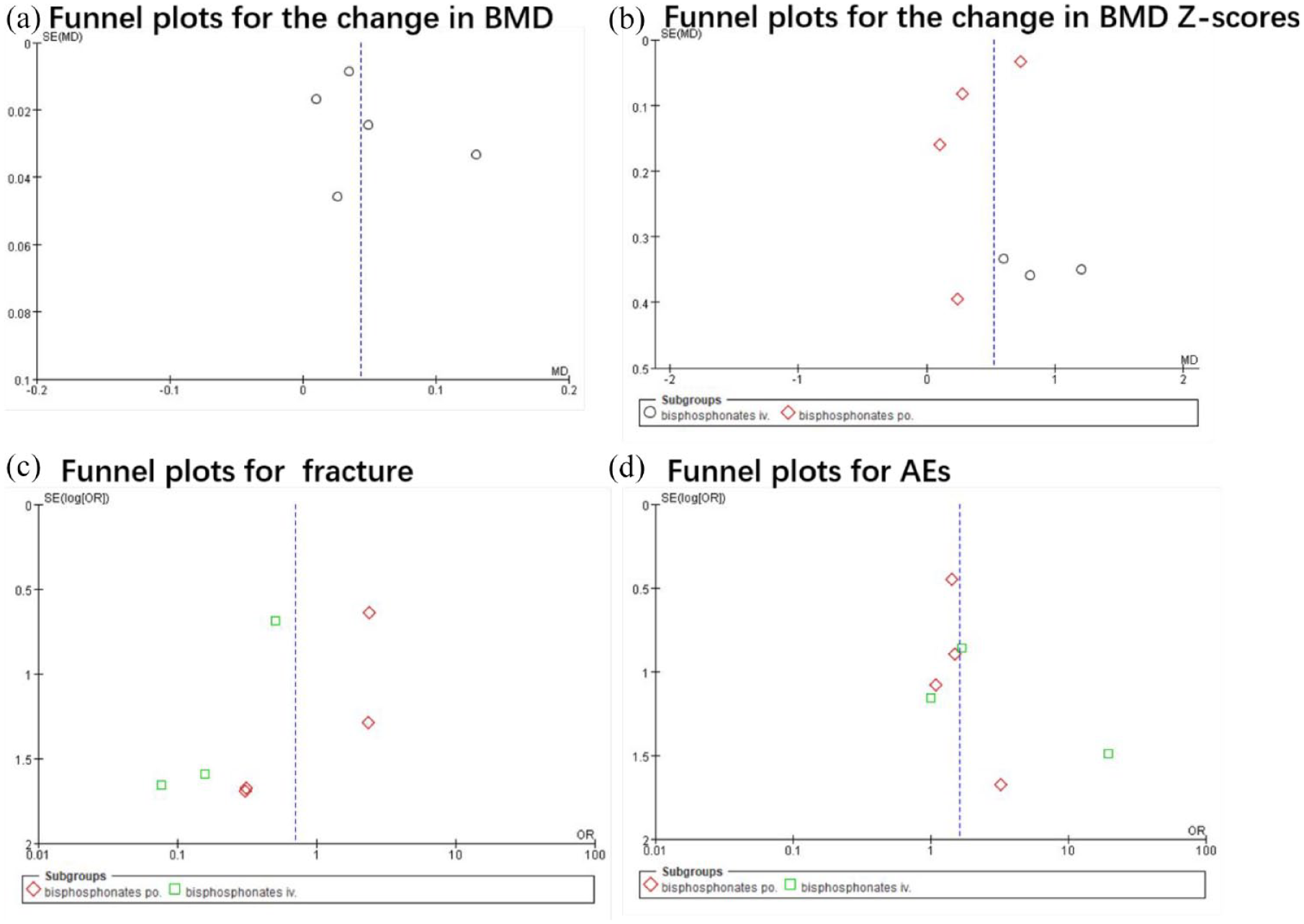
Funnel plots: (a) funnel plots for the changes in BMD of the LS; (b) funnel plots for the changes in BMD Z-scores of the LS; (c) funnel plots of fracture; (d) funnel plots of AEs.
Discussion
The incidence of secondary osteoporosis in children is on the rise due to the increased survival rate of chronically ill patients and the use of bone-damaging drugs. 20 Bisphosphonate therapy is a common treatment for osteoporosis. 21 However, safety concerns have to be considered because bisphosphonate may result in AEs in growing individuals with high bone metabolism. 22 These concerns are largely due to the lack of dependable efficacy and safety data in children with secondary osteoporosis. This meta-analysis evaluated bisphosphonate therapy in secondary childhood osteoporosis, and the findings were as follows: (1) bisphosphonate treatment improved LS BMD and BMD Z-scores over 3–24 months of follow-up; (2) the efficacies of IV bisphosphonates on BMD Z-score and fracture rate were close to significantly better than oral bisphosphonates; (3) the efficacy of bisphosphonates may not be influenced by causes of secondary childhood osteoporosis (steroid-associated versus others); (4) bisphosphonates, either orally or intravenously, did not increase the risk of AEs. Thus, our results suggest bisphosphonates are efficacious and safe for the treatment of secondary childhood osteoporosis.
Because of the limited number of included studies and the existence of heterogeneity, the previous Cochrane review in 2007 4 indicates that the efficacy of bisphosphonates on secondary childhood osteoporosis still needs further evaluation. Compared with the Cochrane review of 2007, 4 here we collected and included four new RCTs10,12,14,15 and did quantitative meta-analyses. We excluded one RCT 19 which was included in the Cochrane review 2007 4 because it reported bone mineral content (BMC) but not BMD. BMD measurement is one of the main bases for the diagnosis of secondary osteoporosis in children. The BMD in our included RCTs was all measured by dual-energy X-ray absorptiometry (DEXA), which is the gold standard for determining BMD. Finally, all included studies used a relatively standardized approach to BMD reporting, which support us to do the quantitative meta-analyses. Based on five included RCTs and a total of 303 patients,9,11–14 we reveal that bisphosphonates improved the change of LS BMD. Based on seven included RCTs and a total of 355 patients,7,9,10,12–15 we reveal that bisphosphonates improved the change of LS BMD Z-scores. Besides, as suggested by the Cochrane review in 2007, 4 we additionally did a preliminary quantitative meta-analysis on the fracture rates, which partly represents the functional bone health outcomes. We found only IV bisphosphonates might slightly but not significantly improve the fracture rates (OR = 0.34, 95% CI: 0.11–1.08, p = 0.07, I2 = 0%). Of note, the type of fracture varied from study to study, and all these included studies may be not powered to study the impact of bisphosphonates on fracture rates (such a trial might require several thousand participants for each kid of bisphosphonates). Thus, taken together, our study provides potentially more solid and comprehensive evidence supporting the use of bisphosphonates in secondary childhood osteoporosis than previous studies. Further RCTs are still warranted to investigate the effect of bisphosphonates on the fracture rates and other functional bone health outcomes in children with secondary osteoporosis.
Heterogeneity is high in the analyses for both LS BMD and BMD Z-scores. Sensitivity analysis shows that the study of Zacharin et al. 14 may be the source of heterogeneity in the analysis of LS BMD. The study of Zacharin et al. 14 is the only one included study that used IV bisphosphonates in the analysis of changes in LS BMD, suggesting drug delivery route may be an important interference factor. Thus, we further did the subgroup analysis according to the route of bisphosphonate administration (IV versus oral). We found the efficacy of IV bisphosphonates on BMD Z-scores was close to significantly better than oral bisphosphonates (p = 0.07 for IV versus oral). Similarly, the efficacy of IV bisphosphonates on fracture rates was almost significantly better than oral bisphosphonates (p = 0.05 for IV versus oral). On the other hand, causes for secondary osteoporosis were also quite diverse among the nine included RCTs. Six of nine included RCTs8,11–15 are mainly due to the use of steroids, while the other three7,9,10 are probably caused by chronic diseases. We found bisphosphonate treatment improved the LS BMD or BMD Z-score in both conditions of secondary osteoporosis (p = 0.99 for steroid-associated versus others). In addition, because of the limited included studies, other interference factors, such as bisphosphonates types, drug delivery frequency, and follow-up duration, were not further analyzed here. Thus, our results suggest the efficacy of bisphosphonates might be influenced by the route of bisphosphonate administration (IV versus oral) rather than the cause of secondary osteoporosis (steroid-associated versus others). The efficacy of IV bisphosphonates may be slightly better than that of oral bisphosphonates for the treatment of secondary childhood osteoporosis. Further RCTs are still warranted to investigate the effect of specific types of bisphosphonates in secondary childhood osteoporosis.
Bisphosphonates may cause abdominal discomfort and abnormal blood tests, and other adverse events. Based on the included seven RCTs and a total of 363 patients,7–10,12,14,15 our analysis interestingly showed that the use of bisphosphonates did not increase the risk of AEs compared with control. Subgroup analysis showed that (1) both IV and oral bisphosphonates are well-tolerated; (2) the causes for secondary osteoporosis also did not influence the safety of bisphosphonates. Thus, our results indicate that bisphosphonates are well-tolerated in children over 3–24 months of follow-up.
Several limitations in our meta-analysis should be considered. (1) Methodology limitations existed in some included RCTs, such as unclear randomization and inadequate allocation concealment. (2) The case number of most RCTs is low. This may be because of the rigorous standard to include the patient with secondary osteoporosis. For example, 86 out of 118 persons did not meet the criteria in the study of Golden et al. 9 Besides, the criterion for osteoporosis in children was not consistent among the included RCTs. (3) The follow-up duration in these included studies ranged from 3 to 24 months. The long-term efficacy and safety of bisphosphonates remain unclear. (4) the existence of unexplained high heterogeneity indicates that other interference factors may still exist (such as different kinds of bisphosphonate and different dosages). Causes for secondary osteoporosis were quite diverse among the studies, which may still contribute to heterogeneity and other bias. (5) As mentioned above, there are obvious limitations for analyzing the data of fracture. These included studies were underpowered to detect the effect of fracture and did not use a standardized approach to fracture reporting.
Conclusion
This meta-analysis suggests that bisphosphonates use is efficacious and safe for the treatment of secondary childhood osteoporosis. The use of bisphosphonates may improve the change in LS BMD and BMD Z-scores without affecting the risk of AEs over 3–24 months of follow-up, which supports the use of bisphosphonates for secondary childhood osteoporosis for clinicians. However, because of the existence of potential biases, high heterogeneity, and other interfering factors, high-quality RCTs are still required to assess the efficacy and safety of the bisphosphonate treatment for secondary osteoporosis in children. In addition to a standardized approach to BMD reporting, fracture and other functional bone health outcomes should be also measured with a uniform standard in future RCT trials. Besides, it still needs to be further confirmed whether the efficacy of IV bisphosphonates was better than that of oral bisphosphonates for the treatment of secondary childhood osteoporosis.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221129163 – Supplemental material for Efficacy and safety of bisphosphonates on childhood osteoporosis secondary to chronic illness or its treatment: a meta-analysis
Supplemental material, sj-docx-1-taj-10.1177_20406223221129163 for Efficacy and safety of bisphosphonates on childhood osteoporosis secondary to chronic illness or its treatment: a meta-analysis by Huawei Zhao, Yunfei Ding, Jufei Yang, Yijun Luo, Zhenghao Xu and Jing Miao in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.