
Abstract
Objective
To investigate the association between creatinine to cystatin C ratio (CCR) and bone mineral density (BMD) in middle-aged and older adults.
Methods
This cross-sectional study investigated participants aged 50–85, using National Health and Nutrition Examination Survey (NHANES) data from 1999 to 2002. The correlation between CCR and total BMD was assessed by multivariate linear regression models, using stratified analysis by age, sex and race (Mexican American, other Hispanic, non-Hispanic White, non-Hispanic Black, and other race) to distinguish various special populations.
Results
Among 2992 patients, multiple regression models revealed a significant positive correlation between CCR and total BMD: model 1, 0.030 (95% confidence interval [CI] 0.029, 0.031); model 2, 0.009 (95% CI 0.008, 0.010); model 3, 0.010 (95% CI 0.009, 0.013). After controlling for all covariates, a positive correlation was observed between CCR and total BMD in both men and women, and was further strengthened in older age groups. When stratifying by race, the positive correlation was most significant among ‘other Hispanic’ participants; there was no significant correlation among those of ‘other race’.
Conclusions
A positive correlation was demonstrated between CCR and total BMD in middle-aged and older adults aged 50–85 years, with the most significant positive correlation in the older ‘other Hispanic’ population. No significant correlation was observed among participants of ‘other race’.
Introduction
Osteoporosis is a bone disease that affects the microarchitecture and density of bone tissue, making bones more fragile and prone to fractures.1,2 As the population ages, osteoporosis is becoming more prevalent,3,4 affecting approximately 200 million people worldwide. 5 Currently, osteoporosis is clinically indicated by measuring bone mineral density (BMD) through dual-energy X-ray absorptiometry (DXA).6,7 However, further exploration of biomarkers related to bone health and density might aid in the early diagnosis, prevention, and treatment of osteoporosis.
Sarcopenia, a syndrome commonly observed in the elderly, is characterized by a gradual decline in skeletal muscle mass and strength over time. This decline is often accompanied by a decrease in muscle function, making it more difficult for individuals to perform daily activities. 8 According to research, there is a correlation between sarcopenia and reduced BMD, leading to an increased risk of osteoporosis. 9 Given that both muscle and bone originate from the mesoderm, share a common mesenchymal precursor, and belong to the motor system, there may be a correlation between muscle mass and bone health. 10 Creatinine is a byproduct of normal muscle tissue breakdown that is often used as an indicator of muscle mass. However, since creatinine levels can be influenced by renal function and other factors, muscle mass cannot be solely determined by creatinine. 11 Serum cystatin C is an endogenous marker that accurately reflects glomerular filtration rate and is not influenced by factors such as gender, age, diet, or muscle mass, making it a reliable indicator of kidney function. Therefore, cystatin C is commonly used for early evaluation of renal function damage.12–14 The ratio of creatinine to cystatin C (CCR) is used to assess muscle mass and skeletal muscle mass adjusted for renal function, and it also has the potential to predict BMD as a marker of sarcopenia. 15
The study by Gao et al. 11 suggests that CCR might influence muscle mass and BMD in elderly Chinese people with type 2 diabetes. In another study, the calcaneal bone velocity of sound was used as a substitute for BMD to validate CCR as a simple measure of bone mass that is independent of muscle mass. 16 However, the mechanisms that link CCR to BMD have not been fully explained. The objective of the present study was to investigate the correlation between CCR and total BMD in individuals aged 50 years and older, using National Health and Nutrition Examination Survey (NHANES) data obtained between 1999 and 2002, from the Centers of Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS).
Participants and methods
Study population and STROBE statement
This cross-sectional study was conducted using de-identified NHANES datasets for participants aged ≥50 years that were collected between 1999 and 2002, as cystatin C data was only collected during this period. Participants aged ≥50 years were enrolled in the study. Participants with missing creatinine data, missing cystatin C data, or missing total BMD data were excluded. The National Center for Health Statistics provided Institutional Review Board approval for NHANES 1999–2004 (Protocol #98-12). Informed consent for the present study was not required as it comprised publicly available NHANES data. The reporting of this study conforms to STROBE guidelines. 17
Variables
In this study, CCR was investigated as the independent variable and total BMD as the dependent variable, using datasets from the NHANES database. Briefly, during data collection for NHANES, serum cystatin C concentrations were measured using an automated particle-enhanced nephelometric assay (Dade Behring N Latex Cystatin C assay), which was run on a Dade Behring turbidimeter II (BNII). Whole body scans, including arms and legs, the trunk, and the head, were conducted using a Hologic Discovery A densitometer (Hologic, Inc., Bedford, MA, USA), and the results of total BMD were obtained using Apex software, version 3.2 (Hologic). Data regarding several covariates were also extracted for the present study, including age, sex (male/female), race, smoking history (at least 100 cigarettes in life), income to poverty ratio, body mass index, high blood pressure, diabetes, high density lipoprotein (HDL)-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C. Further information on data measurement is available at http://www.cdc.gov/nchs/nhanes/.
Statistical analysis
The analysis was conducted following the guidelines provided by NCHS, using sample weights. Continuous variables are presented as mean ± SD and P values were calculated through a weighted linear regression model. Categorical variables are presented as n and percentages, and P values were calculated through a weighted χ2-test. To assess the independent correlation between CCR and total BMD, a weighted multiple regression analysis was performed. Three multiple linear regression models were created: model 1, with unadjusted covariates; model 2, adjusted for age, sex, and race; and model 3, adjusted for all covariates listed in Table 1. Interaction and stratified analyses were conducted according to age, sex and race. To address the nonlinearity between CCR and total BMD, weighted generalized additive models and smoothed curve fitting were utilized. All analyses were conducted using R software (http://www.R-project.org) and EmpowerStats software (http://www.empowerstats.com). A P value <0.05 was considered statistically significant.
Characteristics of 2992 participants aged ≥50 years.

Continuous data presented as mean ± SD; categorical data presented as n (%) prevalence.
BMD, bone mineral density; BUN, blood urea nitrogen; HDL, high density lipoprotein; Smoking history, smoked at least 100 cigarettes in life.
Statistically significant at P < 0.05 (weighted linear regression model for continuous data; weighted χ2-test for categorical data).
Results
A total of 4983 participants aged ≥50 years were initially enrolled into the study. After excluding participants with missing creatinine data (n = 852), missing cystatin C data (n = 1038), or missing total BMD data (n = 101), a total of 2992 participants (1394 [46.6%] males and 1598 [53.4%] females) were included in the final analysis. The largest proportion of participants were non-Hispanic White (2426 [81.1%]), followed by Mexican American, other Hispanic, non-Hispanic Black, and other race, at 90 (3.0%), 150 (5.0%), 236 (7.8%), and 90 (3.0%), respectively. Detailed information on the weighted sociodemographic and medical characteristics of the participants is provided in Table 1. All covariates were found to exhibit significant differences across the four quartiles (Q1–Q4) of CCR.
Multiple regression equations were utilized to examine the correlation between CCR and total BMD in the population, displayed in Table 2 as the correlation between CCR and total BMD as a continuous variable. CCR was found to have a significant positive correlation with total BMD in the multiple regression equations of Model 1 (β = 0.030, 95% confidence interval [CI] 0.029, 0.031), Model 2 (β = 0.009, 95% CI 0.008, 0.010), and Model 3 (β = 0.010, 95% CI 0.009, 0.013). The smoothed curves of CCR and total BMD are shown in Figure 1. After adjusting for all covariates, this trend remained significant in the CCR quartile group (P < 0.001).
The association between creatinine/cystatin C ratio and total bone mineral density (g/cm2).

Model 1, unadjusted data; Model 2, data adjusted for age, sex and race; Model 3, data adjusted for age, sex, race, vigorous recreational activities, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure, diabetes, HDL-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, and serum calcium. In subgroup analysis stratified by sex or race, the model was not adjusted for sex or race, respectively. CI, confidence interval.
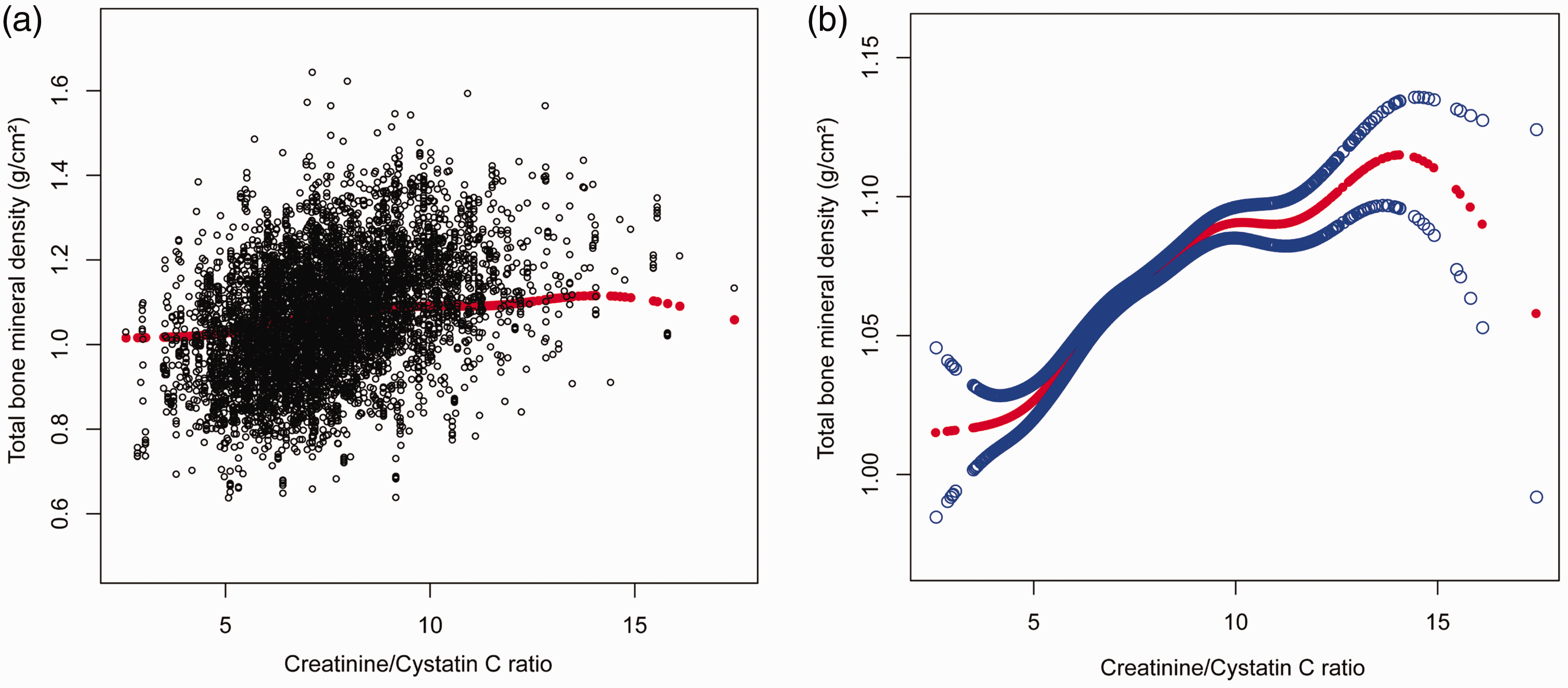
The association between creatinine to cystatin C ratio (CCR) and total bone mineral density (BMD) in 2992 participants aged ≥50 years: (a) scatter plot (each black dot represents a sample) of data adjusted for age, sex, race, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure blood, diabetes, high density lipoprotein (HDL)-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C. The relationship between total BMD and CCR is shown by the smooth curve (red dots) fitted to the scatter plot and (b) The solid arcs indicate the smoothed curve fit between the variables. The blue circles represent the fitted 95% confidence intervals, with data adjusted for age, sex, race, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure blood, diabetes, HDL-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C.
After adjusting for all covariates (Table 2), a positive correlation between CCR and total BMD was observed in both men (β = 0.011, 95% CI 0.008, 0.014) and women (β = 0.015, 95% CI 0.012, 0.018). When stratified by age, a more significant positive correlation was observed between CCR and total BMD in the older age groups. Notably, when data were stratified by race, the correlation between CCR and total BMD was most prominent in the ‘other Hispanic’ group (β = 0.034, 95% CI 0.026, 0.041), while no statistically significant correlation was observed in the ‘other race’ group (β = –0.016, 95% CI –0.0041, 0.008). To investigate the relationship, weighted generalized additive models and smoothed curve fitting was utilized to resolve the nonlinear relationship. Subgroup analysis was also conducted (Figures 2, 3, and 4). In the interaction results, the correlation between CCR and total BMD was observed to be influenced by age and race (P interaction <0.05), but was not influenced by sex (P interaction >0.05).
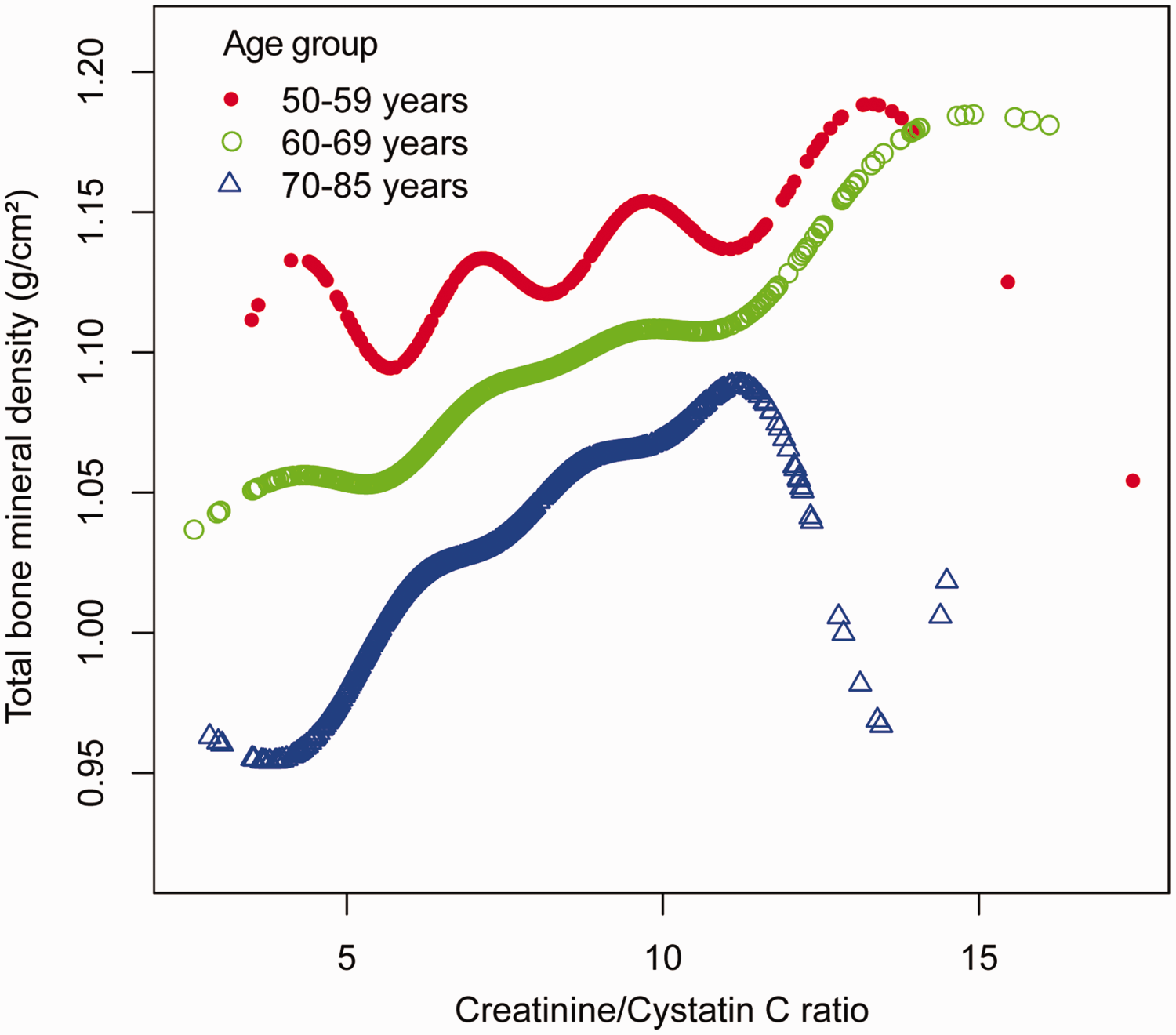
The association between creatinine to cystatin C ratio and total bone mineral density in participants aged ≥50 years stratified by age, with data adjusted for sex, race, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure blood, diabetes, high density lipoprotein-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C.
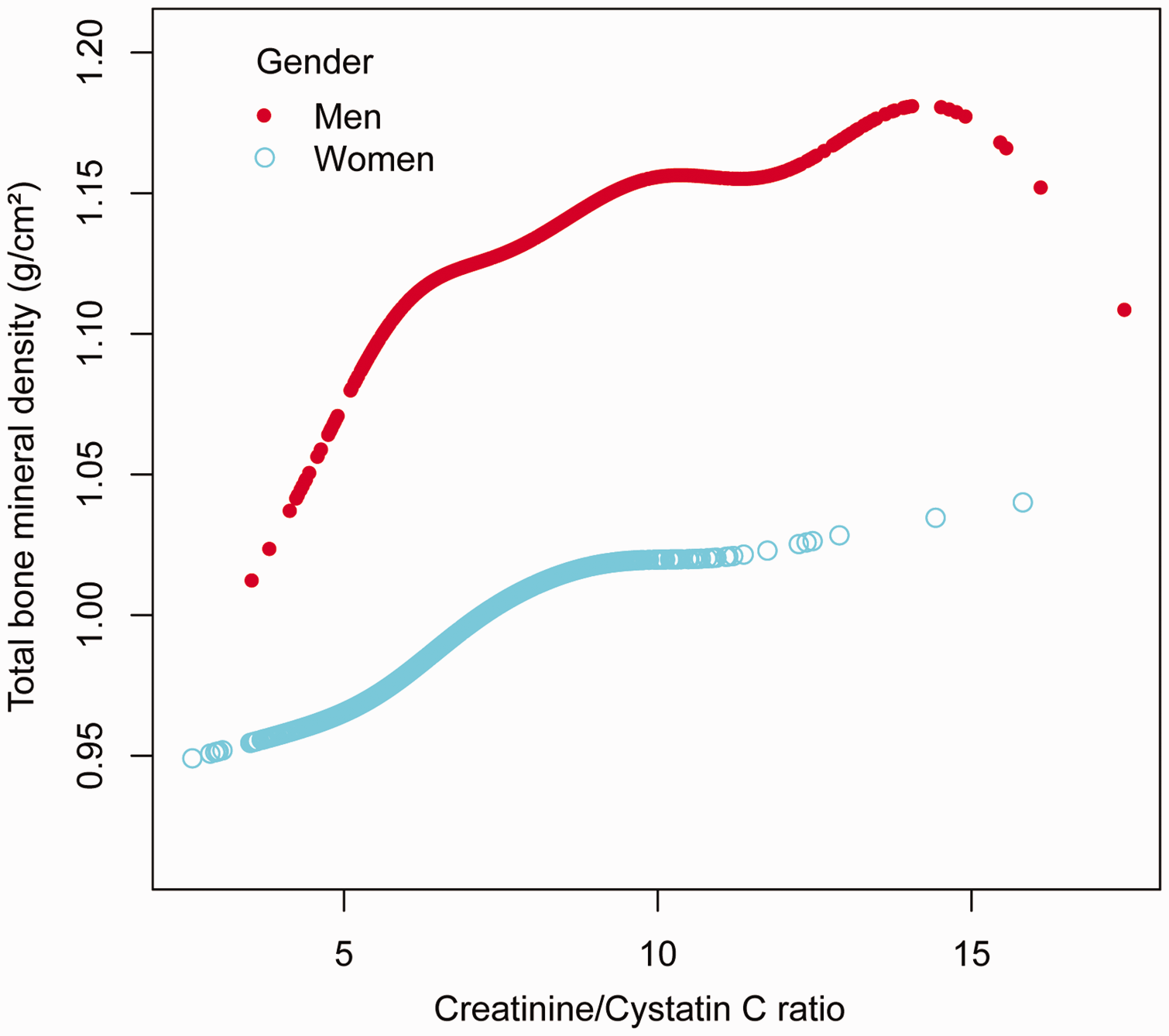
The association between creatinine to cystatin C ratio and total bone mineral density in participants aged ≥50 years stratified by sex, with data adjusted for age, race, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure blood, diabetes, high density lipoprotein-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C.

The association between creatinine to cystatin C ratio and total bone mineral density in participants aged ≥50 years stratified by race, with data adjusted for age, sex, smoked at least 100 cigarettes in life, income to poverty ratio, body mass index, high blood pressure blood, diabetes, high density lipoprotein-cholesterol, blood urea nitrogen, total protein, total cholesterol, serum phosphorus, serum calcium, creatinine, and cystatin C.
Discussion
The aim of this cross-sectional study was to determine how CCR and total BMD relate to each other in middle-aged and older adults. CCR was found to be positively correlated with total BMD, even when multiple confounders were taken into account. This correlation became more significant in older age groups. The correlation was found to be most pronounced in the other Hispanic population (non-Mexican American Hispanic), whereas no significant correlation was observed in the ‘other race’ group (those who were neither Hispanic nor non-Hispanic Black or non-Hispanic White). These findings provide new epidemiological evidence linking elevated CCR to relatively high BMD in middle-aged and older adults, which may contribute to a better understanding of the link between CCR and bone health.
Serum creatinine reflects the body's skeletal muscle mass, and creatinine levels may decrease in conditions such as muscle atrophy or muscle tissue destruction. 18 The relationship between muscle and bone is important in bone remodeling, 19 as muscles are attached to bones and secrete factors that can affect bone growth and development.20,21 When skeletal muscles are lost, skeletal health and function are affected, and a higher death risk is incurred. 22 A cross-sectional study found that adolescents with higher serum creatinine levels had higher BMD in the total and lumbar spines. Analyses stratified by race, age, and sex showed the same positive association. 23 Another study reported a positive correlation between subcutaneous adipose tissue cell telomere length and serum creatinine, suggesting that decreased serum creatinine may lead to decreased BMD through oxidative stress. 24 It is unclear how creatinine levels impact BMD, and other unknown factors may also have an impact.
As a cysteine protease inhibitor, cystatin C is crucial to the body's metabolism of homocysteine. When cystatin C levels increase, homocysteine catabolism is inhibited, resulting in increased levels of serum homocysteine. This, in turn, affects the bone transformation process by inducing the differentiation of mononuclear macrophages into osteoclasts, inhibiting apoptosis of osteoclasts, and promoting apoptosis of osteoblasts, ultimately affecting BMD.25,26 Cystatin C is significantly associated with renal function, and chronic kidney disease affects bone metabolism.27,28 Chronic kidney disease is associated with decreased BMD and increased fracture risk.29,30 A Mendelian randomization study of MR-Base and UK Biobank data showed significant correlations between serum cystatin C levels and osteoporosis. 5 According to a cross-sectional Korean study, serum cystatin C concentrations were inversely correlated with BMD among women, but not men. Women with a higher cystatin C level were more likely to have osteoporosis, whereas men did not show such a correlation. 31 These findings suggest that cystatin C might be a useful biomarker for assessing bone health, particularly among patients with chronic kidney disease.
Studies have shown that CCR is positively linked with muscle mass and strength.32–34 In 2013, CCR was first discovered to predict musculoskeletal disorders and muscle mass. 35 In addition, CCR has been demonstrated to predict fragility fractures in patients with type 2 diabetes. 36 Given the close relationship between muscle and bone health, CCR may be used as an independent predictor of total BMD. In the present study, CCR was found to be positively correlated with total BMD in Hispanic and non-Hispanic Black and White populations, but not in those of other race. This suggests that CCR may potentially serve as a cost-effective and simple predictor of osteoporosis in future clinical practice.
The present study has several strengths, including the large US-based sample that represents a broad range of ages and races, allowing for further subgroup analyses. However, the present results may be limited by several factors. First, the cross-sectional study design prevents the establishment of a causal relationship between CCR and bone density. Secondly, it should be noted that muscle mass and function were not assessed, which prevents any confirmation that the effect of CCR on bone density is mediated through muscle. Thirdly, other unmeasured confounding factors may have contributed to bias. Thus, further investigations of CCR and total BMD should be conducted longitudinally using larger sample sizes.
Conclusion
In conclusion, the present study demonstrates a positive correlation between CCR and total BMD in middle-aged and older adults aged 50–85 years. However, this correlation varies among different age groups and races. Specifically, a positive correlation was found to be most significant in the older ‘other Hispanic’ population (non-Mexican American Hispanic), while no significant correlation was observed in the ‘other race’ group (those who were neither Hispanic nor non-Hispanic Black or non-Hispanic White). These findings contribute to a better understanding of the association between CCR and bone health.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231206305 - Supplemental material for Association between the ratio of serum creatinine to cystatin C and bone mineral density in middle-aged and older adults: a cross-sectional study from NHANES database
Supplemental material, sj-pdf-1-imr-10.1177_03000605231206305 for Association between the ratio of serum creatinine to cystatin C and bone mineral density in middle-aged and older adults: a cross-sectional study from NHANES database by Zhenwei Wang, Weibin Du, Yuanbin Ou, Meichun Han, Jintao Hu and Renfu Quan in Journal of International Medical Research
Footnotes
Author contributions
Zhenwei Wang, Yuanbin Ou and Meichun Han collected data and wrote the manuscript. Zhenwei Wang and Weibin Du were major contributors to writing the manuscript. Jintao Hu and Renfu Quan contributed to study conception and design. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This work is supported by the Special Research Project of the Affiliated Hospital of Zhejiang Chinese Medical University (No. 2021FSYYZY43); Hangzhou Medical and Health Technology Planning Project (No. B20220021, B20200032, A20220507); Hangzhou Science and Technology Planning Project (No. 2020ZDSJ0042, 20220919Y084); Zhejiang Province Traditional Chinese Medicine Science and Technology Project (No. 2022ZB232, 2023ZR046); and Research Project of Zhejiang Chinese Medical University (No. 2021JKZKTS057B).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.