
Abstract
Objectives
To identify the effects of two years’ oral bisphosphonate (alendronate) treatment in patients who underwent total knee arthroplasty (TKA); to determine whether significant responses seen after the first year of treatment changed during the second year. Additionally, the study tried to identify factors relating to bone mineral density (BMD) changes.
Methods
This was a prospective 2-year follow-up study of a previous 1-year report of postmenopausal women with knee osteoarthritis who underwent primary unilateral or staged bilateral TKA, after which they received 70 mg alendronate orally once-weekly. BMD was measured using quantitative computed tomography (QCT) on lumbar vertebrae at baseline (pre-TKA) and at 12 and 24 months. Factors associated with BMD changes were determined by regression analysis.
Results
Sixty-one patients entered the second year and continued treatment for ≥24 months. Mean vertebral QCT BMDs at baseline and after 12 and 24 months’ alendronate treatment were 71.8 mg/ml (41.9–97.5 mg/ml), 69.3 mg/ml (31.4–103.9 mg/ml), and 72.7 mg/ml (33.1–136.1 mg/ml), respectively. Patients undergoing bilateral TKA and who had more severe OA at baseline (bilateral severe [grade 4] OA) had a lower BMD response after 2 years’ bisphosphonate treatment, compared with patients with less severe unilateral knee OA who underwent unilateral TKA. Improvements were, however, seen compared with year 1 levels. Low BMI was associated with BMD nonresponse.
Conclusions
Patients with bilateral severe OA (grade 4) requiring bilateral knee replacement are at greater risk of nonresponse after 2 years’ oral alendronate treatment. A longer duration of treatment may be necessary in these patients.
Keywords
Introduction
Osteoarthritis (OA) and osteoporosis (OP) are both common in the elderly and the two conditions may be associated, as shown in several studies that have demonstrated an increased bone mass in OA patients – even at sites distant to OA-affected joints – but similar or higher risks of fragility fracture.1–3 Furthermore, prospective cohort studies have suggested an increased risk of fragility fractures in OA.4–6 Patients with a clinical diagnosis of knee OA have double the risk of a fragility hip fracture, suggesting poor bone quality in patients with severe knee OA. 4
Globally, OA is the most prevalent form of arthritis and the prevalence of clinically diagnosed knee OA is increasing.7,8 In advanced OA, when other treatment modalities are of no benefit, total knee arthroplasty (TKA) has proven to be the most successful intervention to reduce knee pain and improve physical function.9,10 TKA is one of the most commonly performed orthopaedic surgical procedures in older women who are also likely to require OP management; this patient subgroup is of particular interest because of the high risk of bone fractures.
The effect of 12 months’ oral bisphosphonate (as alendronate) in postmenopausal patients with knee OA, who subsequently went on to receive TKA, has been studied previously by our group. 11 Our research showed that lumbar spine quantitative computed tomography (QCT) bone mineral density (BMD) declined in over half (53.7%) of these patients after alendronate treatment, and that this decline was significant in patients who underwent bilateral versus unilateral TKA.
The present prospective cohort study represents a follow-up of the previous 1-year report. 11 The objectives were to identify the effects of 2 years’ oral alendronate treatment, and to determine whether significant responses (decline of BMD in bilateral TKA patients) seen after the first year of treatment normalized during the second year: a phenomenon described previously with long-term bisphosphonate treatment (described as ‘regression to mean’). 12 The present study also determined whether the severity of knee OA affected response to bisphosphonate therapy, as this was not determined in the previous study.
Patients and methods
Study population
This was a prospective 2-year follow-up study of a previous 1-year study that enrolled consecutive postmenopausal women who underwent primary, elective TKA for knee OA, between March 2007 and October 2009, at Hanyang University Hospital, Seoul, Republic of Korea. Eligible patients had to be >12 months postmenopausal and with a lumbar spine QCT BMD of <120 mg/ml. Patients were excluded if they had a rheumatic disease or a disease capable of affecting the skeleton, were taking medication capable of affecting the skeleton, or had a medication possession ratio (MPR; a measure of compliance with the medicine) <80%.
The study protocol was approved by the Institutional Review Board on human subject research and by the Ethics Committee of the Hanyang University Hospital, Seoul, Republic of Korea. All patients provided written informed consent.
Study procedures
All patients underwent either unilateral or staged (with a 2-week interval) bilateral knee TKA. All TKAs were performed using cemented, posterior-stabilized prostheses. After surgery, patients performed active and passive knee range-of-motion exercises. Patients began walking with walking aids when active knee flexion was >90° and quadriceps strength was considered sufficient.
After surgery, all patients received 70 mg alendronate plus 5600 IU vitamin D3 tablets (Fosamax-plus®, Merck Sharp & Dohme, NJ, USA) orally, once-weekly. Patients were educated on how to take the medications correctly (e.g. with 6–8 oz of plain water ≥30 min before first breakfast, and not to lie down for ≥30 min after taking medication) and were checked routinely on an outpatient basis to confirm they were taking their medication correctly. MPRs were calculated for all patients, and were used as an indicator of the level of compliance. 13 MPR was defined as the number of days alendronate was taken during the study period divided by 365 (for 1-year analysis). A weekly dose was viewed as administration for 7 days and prescription of alendronate at 70 mg/week was viewed as administration for 28 days (prescribed on a monthly basis; four tablets).
Study assessments
Patient characteristics were obtained retrospectively by reviewing medical histories and operation records. Associated comorbidities were obtained by history taking and by preoperative examinations, and included hypertension, diabetes, cardiovascular disease, respiratory diseases and cerebral vascular diseases. To identify factors associated with BMD changes, age, body mass index (BMI; kg/m2), radiographic knee OA grade (assessed using the Kellgren–Lawrence classification system 14 ), surgical procedure (unilateral versus bilateral TKA) and the number of associated comorbidities were reviewed. Knee Society knee and function scores were recorded for each patient at baseline and annually thereafter, using distinct 100-point scales, with higher score indicating better knee status. 15 Standard anteroposterior, posteroanterior, lateral, and merchant radiographs of both knees were routinely obtained preoperatively and evaluated for severity of OA using the Kellgren–Lawrence classification system. 14 Knees, including nonoperated knees, were classified as either bilateral severe OA if both knees were of Kellgren–Lawrence grade 4 (large osteophytes, marked joint space narrowing, severe sclerosis and a definite deformity of bone contour) or unilateral severe OA, if the contralateral knee was of grade 0 to grade 3. 14
Quantitative computed tomography was performed on lumbar vertebrae (L2–4) at baseline and at 12 and 24 months after surgery (80 Kv; 10-mm slice thickness). Traditional single-slice-based volumes of interest (VOIs) in trabecular osteo VOIs were measured at vertebral body midsections and trabecular BMDs (mg/ml) were used to calculate mean BMD. A decline or gain in BMD was defined as a change greater than least significant change (LSC) in lumbar spine BMD, as described previously.16–19 To calculate LSC at the lumbar spine (L2–L4) with a 95% level of confidence (confidence interval, CI), the precision error obtained from the medical centre was multiplied by 2.77, which yielded an LSC of 2.77%.
Patients who experienced a decline in BMD exceeding LSC were defined as nonresponders and patients who experienced an increase in BMD exceeding LSC were defined as responders.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical software program, version 10 (SPSS Inc., Chicago, Il, USA) for Windows®. Demographic and clinical variables were compared using the independent-sample t-test, Fisher’s exact test or χ2-test as appropriate. In addition, univariate and multivariate logistic and linear regression analysis were used to identify factors relating to BMD response. All results were presented as mean values with 95% CI. Pearson’s correlation coeffcient was calculated to identify the relationship between bilateral TKA and bilateral severe OA patients. P-values < 0.05 were considered statistically significant.
Results
Eighty-two patients were enrolled for the first 12 months, as described in the 1-year study;
11
61 patients were enrolled into the 2-year follow-up study and 21 patients were excluded from entering the second year because of poor compliance (MPR < 80%) (Figure 1). Mean patient age was 69.8 years (55–83 years) at the time of operation. Of the 61 patients followed for 2 years, 10 experienced a decline or gain in BMD not greater than the LSC at 2 years: these patients were not included in the logistic regression analyses.
Flow of patients in a 2-year study evaluating the effect on bone mineral density of oral alendronate treatment after total knee arthroplasty.
According to the Kellgren–Lawrence classification of preoperative knee radiographs, 14 46 patients showed severe bilateral OA (grade 4 for both knees), and 15 showed severe unilateral OA (grade 4 for affected knees; grade 2 [four patients] or grade 3 [11 patients] for contralateral knees). Of the 46 patients with severe bilateral OA, 39 (84.8%) underwent bilateral TKA for debilitating pain in both knees; the remaining seven patients underwent unilateral TKA.
Clinical characteristics at baseline and at 2 years’ follow-up in postmenopausal women who underwent primary, elective total knee arthroplasty (TKA) for knee osteoarthritis (OA) in a 2-year study to evaluate the effect of oral alendronate treatment on bone mineral density after TKA.

Data presented as mean ± SD.
Patients experiencing a decline in BMD exceeding LSC.
Patients experiencing an increase in BMD exceeding LSC.
Knee and function scores determined by the Knee Society Knee Score (range 0–100). 15
BMD, bone mineral density; BMI, body mass index; LSC, least significant change.
No statistically significant between-group differences (P ≥ 0.05); Fisher’s exact test/χ2-test as applicable.
Figure 2 shows QCT BMD changes over 2 years according to surgical procedure. The decline in BMD during the first year of treatment in patients who underwent bilateral TKA began to increase from 1-year onwards, almost reaching pretreatment levels after 2 years’ treatment. Patients who underwent unilateral TKA achieved a steady increase in QCT BMD throughout the 2-year treatment period. Similar results were seen when patients were stratified by knee OA severity (Figure 3).
Changes in bone mineral density (BMD) over 2 years of oral alendronate treatment, stratified according to surgical procedure (unilateral total knee arthroplasty [TKA] or bilateral TKA), in postmenopausal women who underwent primary elective TKA for knee osteoarthritis and were followed-up for ≥24 months. Changes in bone mineral density (BMD) over 2 years’ oral alendronate treatment, stratified according to severity of knee osteoarthritis (OA) (grade 4 bilateral OA versus unilateral OA),
14
in postmenopausal women who underwent primary elective total knee arthroplasty (TKA) for knee osteoarthritis and were followed-up for ≥24 months.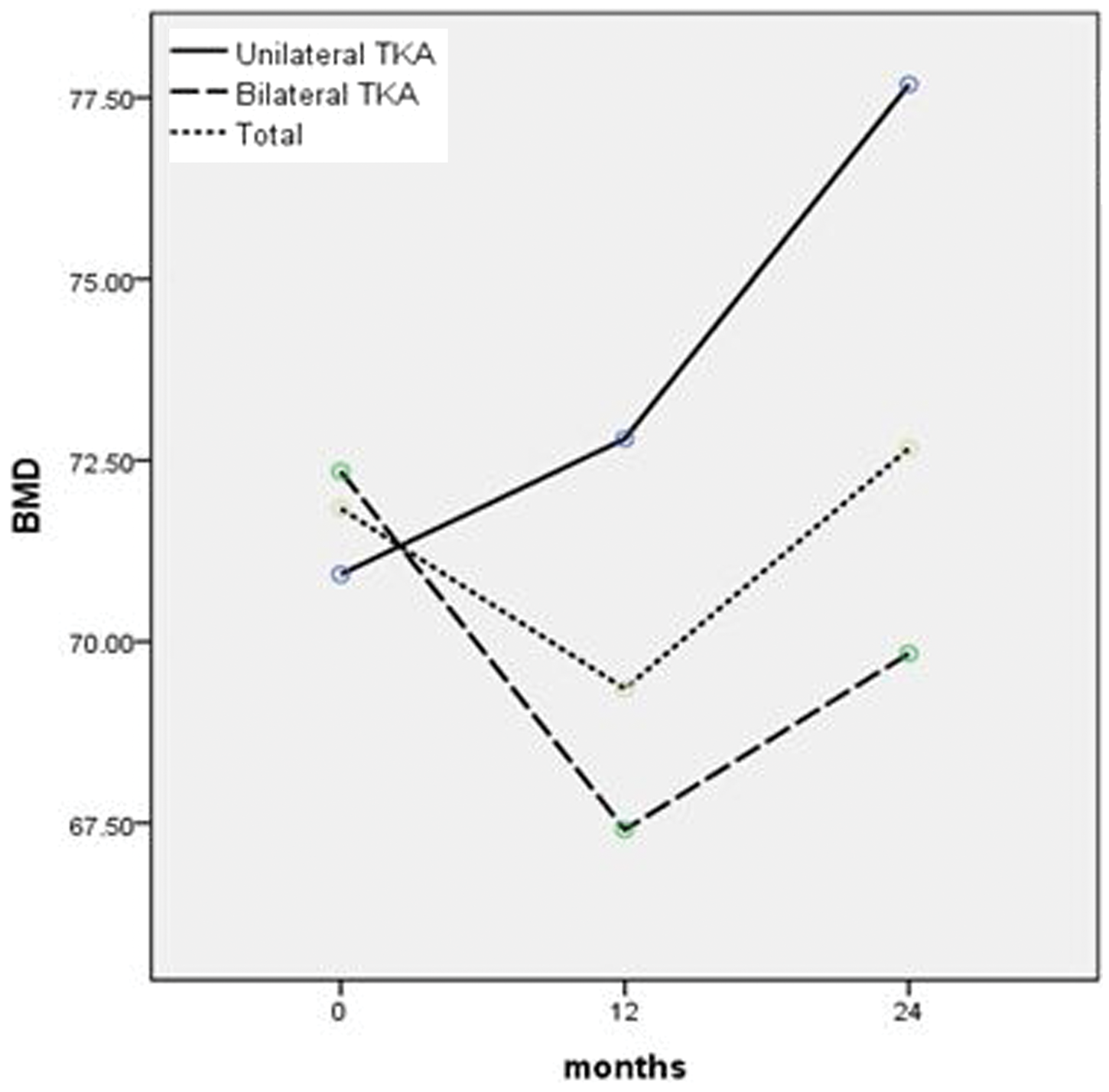

Univariate logisitc analysis of factors relating to a decline in bone mineral density (BMD), in postmenopausal women who underwent primary elective total knee arthroplasty (TKA) for knee osteoarthritis (OA) in a 2-year study, which evaluated the effect of oral alendronate treatment on BMD after TKA.

Data presented as odds ratios (95% confidence intervals).
Calculated using univariate logistic regression analysis.
Defined as 2nd-year knee score minus baseline knee score.
Defined as 2nd-year function score minus baseline function score.
TKA, total knee arthroplasty; BMI, body mass index; OA, osteoarthritis.
Multivariate analysis of factors related to a bone mineral density (BMD) decline in postmenopausal women, who underwent primary elective total knee arthroplasty (TKA) for knee osteoarthritis (OA) in a 2-year study, which evaluated the effect of oral alendronate treatment on BMD after TKA.

Data presented as odds ratios (95% confidence intervals).
Calculated using multivariate logistic regression analysis.
Defined as 2nd-year knee score minus baseline knee score.
Defined as 2nd-year function score minus baseline function score.
TKA, total knee arthroplasty; BMI, body mass index; OA, osteoarthritis; NA, not applicable.
Univariate and multivariate linear regression analysis was also performed on all 61 patients included in the 2-year analysis. A significant relationship between BMD nonresponse and bilateral TKA (versus unilateral TKA) and bilateral severe OA (versus unilateral severe OA) was found (data not shown).
Discussion
The present study reported, for the first time, the effect of 2 years’ oral bisphosphonate (as alendronate) after TKA on lumbar spine BMD in postmenopausal women. In patients undergoing bilateral TKA, BMD declined during the first year of treatment but increased almost back to pretreatment levels during the second year. Logistic and linear regression analysis showed that surgical procedure (bilateral TKA versus unilateral TKA), and more severe OA (bilateral severe [grade 4 14 ] OA), were significantly associated with BMD nonresponse during 2 years of treatment.
In the previous 1-year study, 53.7% (44/82) patients experienced a mean lumbar spine QCT BMD decline of 6 mg/ml after 1 year of oral bisphosphonate treatment, whereas the remaining 38 (46.3%) patients experienced a mean increase of 6.8 mg/ml. 11 Logistic and linear regression analyses showed that bilateral TKA was significantly associated with a decline in BMD. The present follow-up study determined the effect of 2 years’ oral bisphosphonate administration and examined whether the significant decline of BMD observed in the bilateral TKA group after the first year of treatment normalized during the second. The results showed that 2 years of bisphosphonate treatment may not be enough to achieve full recovery in BMD in bilateral severe OA patients undergoing bilateral TKA. Patients with less-severe unilateral OA, undergoing unilateral TKA, showed a steady increase in BMD throughout the 2-year treatment period. In bilateral TKA patients, BMD had almost reached pretreatment levels after 2 years’ bisphosphonate treatment, suggesting that continued bisphosphonate treatment of ≥2 years may be required to achieve a significant BMD increase. Additionally, seven patients with bilateral severe (grade 4 14 ) OA underwent unilateral TKA, suggesting that not all patients with radiographically severe bilateral OA will require bilateral TKA. A significant decline in BMD was significantly greater only in bilateral severe OA patients undergoing bilateral TKA. Thus, bilateral severe OA, rather than bilateral TKA, might have had more impact on BMD decrease during the 2-year treatment period.
Several studies have reported a possible association between OA and OP.1–4,20–22 A prospective cohort study demonstrated an increased risk of fragility fractures in patients with OA. 5 Additionally, a higher fragility hip-fracture rate in patients with knee OA who subsequently went on to receive TKA has been reported; 6 in this study, the fracture rate started to increase the year before (and peaked at 18 months after) TKA, only returning to normal after 3 years. 6 The present ongoing study could provide an answer to the normal return of fracture risk after 3 years, as it is expected that an improvement in lumbar spine QCT BMD over 2–3 years’ bisphosphonate treatment might be demonstrated in patients with severe OA undergoing bilateral TKA.
There were several limitations to the present study. First, there was no control group, and it was not possible to compare results with patients who underwent TKA but did not receive bisphosphonate treatment. Secondly, the sample size was small and 21 patients were excluded during the second year of follow-up due to noncompliance. Thirdly, based on previous database study reports in this population, 6 the follow-up period may have been too short to show a full recovery in BMD with bisphosphonate treatment post-bilateral TKA. It could be speculated that a third year of bisphosphonate treatment would show significant gains in BMD in patients with more severe knee OA undergoing bilateral TKA. Fourthly, bone marker levels were not monitored (e.g. N-telopeptide of collagen type I, carboxyl-termial cross-linking region of collagen type I); these biochemical markers of bone turnover are known to reflect the activity of osteoclasts and osteoblasts, 23 and should be included in future studies. Finally, OA severity should have been more specifically evaluated: it was only classified as either bilateral severe OA if both knees were of Kellgren–Lawrence 14 grade 4, or unilateral severe OA if the contralateral knee was of grade 0 to grade 3. 14
In summary, the present study describes the effect of 2 years’ oral alendronate treatment after TKA on lumbar spine BMD, as determined by QCT. In particular, patients with bilateral OA (grade 4 14 ) undergoing bilateral TKA were found to have lower BMD response after 2 years of bisphosphonate treatment than patients with less severe unilateral knee OA who underwent unilateral TKA. Improvements were, however, seen from year 1 onwards. Furthermore, low BMI was associated with BMD nonresponse. Further longer-term studies are required to show whether continued treatment with bisphosphonates would produce further improvements in BMD levels, in patients undergoing TKA.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.