
Abstract
Objective:
To identify the factors that predict the remission and relapses in myasthenia gravis (MG) patients improved by prednisone and tacrolimus treatment.
Methods:
A retrospective, observational cohort analysis of MG patients who achieved remission after receiving prednisone and tacrolimus were performed at Tongji Hospital. The main outcome measures were the time to remission, prednisone discontinuation, tacrolimus reduction–associated relapse, and treatment outcome.
Results:
After adding tacrolimus, 256 patients were able to achieve remission with a mean time to remission of 2.1 ± 1.4 months. After a median follow-up of 2.9 years, 167 patients (65.2%) discontinued prednisone, and 20 patients (7.8%) achieved complete stable remission. Moreover, 53 of the 109 patients who were tapering tacrolimus experienced relapses. In multivariable analysis, female sex, low tacrolimus concentrations, and quantitative myasthenia gravis (QMG) scores have a positive correlation with the time to remission; concomitant additional autoimmune disease (AID) and high anti-acetylcholine receptor antibody (AChR-ab) levels were significantly associated with low probabilities of prednisone discontinuation [odds ratio (OR) = 0.312–0.912, respectively]; rapid tacrolimus decrement speed (⩾0.76 mg/year) was an independent predictor for the development of relapse during tapering tacrolimus (OR = 5.662).
Conclusion:
Sex, tacrolimus concentrations, and QMG scores can be used as potential predictors of the time to remission in MG patients treated with tacrolimus and prednisone. Prednisone should be tapered slowly, especially in patients with additional AID or high serum titers of AChR-ab. To avoid symptoms recurrence, the dose of tacrolimus should reduce slowly, not exceeding 0.76 mg/year.
Introduction
Myasthenia gravis (MG) is an immune-mediated neuromuscular disorder that leads to fluctuating and fatigable muscle weakness, caused by circulating antibodies, including anti-acetylcholine receptor (AChR), anti-muscle-specific kinase (MuSK) antibodies, and low-density lipoprotein receptor–related protein 4 (LRP4) antibodies. 1 The long-term treatment plan should include immunotherapy and glucocorticoids (steroids) are the main therapeutic options for controlling MG symptoms. 2 Although effective, prolonged use of steroids frequently results in considerable side effects, necessitating the administration of steroid-sparing agents.3,4 Tacrolimus, a calcineurin inhibitor, is widely used as a potent immunosuppressor to improve the symptoms of MG patients, especially in the Asian population.5–7 Several studies have demonstrated that tacrolimus significantly reduced prednisone dose and improved outcomes in various forms of MG, including thymomatous and seronegative MG.7–9 A few studies, however, have focused on the time required to achieve remission after adding tacrolimus, as well as the factors associated with the initial acting time of tacrolimus and possibility of discontinuing prednisone. Furthermore, once the MG symptoms had been effectively controlled, tacrolimus should be tapered to avoid unnecessary costs and adverse events.4,10 A rapid dose reduction of tacrolimus may lead to a recurrence of myasthenic weakness. As a result, it is critical to understand the frequency of and factors predicting initial exacerbations with tacrolimus dose reductions.
We present a retrospective cohort analysis of outcomes in MG patients from our clinic who were treated with prednisone and tacrolimus. Our goal is to determine the factors for predicting the time required in MG patients to achieve remission, the frequency of prednisone discontinuation, the tacrolimus reduction–associated relapses, and treatment outcome.
Materials and methods
Patient selection and study design
This retrospective cohort study was performed for patients with MG who were treated with prednisone and tacrolimus at Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology from January 2012 to May 2021. The diagnosis of MG was based on the clinical history of fluctuating and fatigable muscle weakness together with one or more of the positive results of the neostigmine, repetitive nerve stimulation (RNS), or AChR-ab test. 11 Specifically, a positive response to the neostigmine test was defined as a reduction of QMG score ⩾60% in any of the tested muscles with significant weakness after intramuscular injection of 1–1.5 mg neostigmine methylsulfate and 0.5 mg atropine, positive RNS was defined as a decrement of greater than 10% between first and fifth compound muscle action potential (CMAP) amplitude in any of tested nerves following 2–5 Hz stimulation, and anti-AChR antibody (AChR-ab) titers >0.50 nmol/l were defined as positive (RIA kit, RSR Limited, Cardiff, UK). All patients had achieved remission, which was defined as no symptoms of functional limitations of MG but some weakness of extraocular muscles on examination. 12 Patients were excluded if they had any of the following conditions: (a) thymectomy or other steroid-sparing agents were used within 3 months of receiving tacrolimus, (b) patients had an inadequate response to tacrolimus after at least 24-week treatment, (c) tacrolimus was withdrawn due to adverse events, (d) follow-up was less than 1 year, or (e) there was insufficient baseline data.
A subsequent follow-up was performed to identify those who had undergone a taper of tacrolimus. The patients with tacrolimus reduction were divided into two groups based on whether or not they experienced relapse: relapsed group and nonrelapsed group. The relapse of MG was defined as the reappearance or worsening of one or more MG symptoms or signs of muscle weakness with QMG scores ⩾3 points that lasted more than 24 h. Furthermore, the duration between the MG relapse and the last remission should be more than 3 months.6,13 Patients were excluded if their symptoms relapsed with other definite factors (such as infection, inappropriate drug, fatigue, or pregnancy) or if their follow-up was less than 6 months after tapering tacrolimus. The selection procedure is depicted in Figure 1.

Flowchart of participants’ recruitment.
Clinical parameters and therapy administration
The following patient characteristics were collected from medical records: onset age, sex, symptoms at onset, disease duration from onset to starting tacrolimus, concomitant autoimmune disease (AID), the serum levels of AChR-ab and anti- muscle-specific kinase antibody (MusK-ab) titers estimated by radioimmunoassay, initial tacrolimus trough concentration measured by liquid chromatography-mass spectrometry, thymus type, thymectomy, drug dose reduction and withdrawal, the Myasthenia Gravis Foundation of America (MGFA) clinical classification at maximum severity, 12 quantitative myasthenia gravis (QMG) scores evaluated at tacrolimus administration, 14 and MGFA postintervention status at the last visit. 12 Patients with negative AChR-ab (<0.5 nmol/l) were referred to as seronegative myasthenia gravis (SNMG). According to the MGFA postintervention status, complete stable remission (CSR) was defined as no symptoms or signs of MG for at least 1 year without the use of any pharmacologic medications. 12
All patients were treated with pyridostigmine bromide and prednisone at the same as or before tacrolimus. Tacrolimus (Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd., Hangzhou, China; H20094027) at a dose of 1–3 mg/day was prescribed to all patients, with a target trough concentration of 5–10 ng/ml. Once significant improvements in MG symptoms were observed, prednisone reduction was started at a rate no faster than 5 mg every 2 weeks for doses higher than 20 mg/day, 5 mg every month for lower doses, and finally adjusted as necessary to maintain remission. If patients continued to do well after at least 3 months of minimum dose or discontinuation of prednisone, a gradual reduction in tacrolimus dose would be initiated. The reduction speed is calculated as follows: the beginning dose diminished by the final dose divided by the duration of taper. Duration of taper was defined as the periods from the starting of tacrolimus use to relapse, stable tacrolimus dose, or tacrolimus withdrawal. If the clinical symptoms recurred, the dose of prednisone or tacrolimus was increased immediately until the symptoms improved and stabilized.
Statistical analysis
Numerical data are presented as mean value ± standard deviation (SD) or median [interquartile range (IQR)], and categorical data are presented as frequencies with absolute numbers and percentages. Correlations between clinical factors were evaluated using Spearman’s rank correlations. Kaplan–Meier curve was performed to visualize the rate of prednisone discontinuation during the tacrolimus treatment. Multiple linear regression was applied to measure the association between all clinical variables and the time to attain remission. Logistic regression was used to identify possible factors correlated with the prednisone discontinuation and tacrolimus reduction–associated relapse; univariate associations with a p value < 0.20 were used to build a multivariate model. The relapse risk was further evaluated with receiver-operating characteristic (ROC) curves, and the optimal cut-off values were defined as the point at which Youden’s index was maximal. Using parameters estimated from the sample, 15 a post hoc power calculation demonstrated that this study had 100% power to investigate predictors of the time required to achieve remission and prednisone discontinuation, and had 86% power to identify the predictors of the tacrolimus reduction–associated relapses. All data analyses were performed with IBM SPSS statistics version 22.0 (Armonk, NY, USA) and G* Power 3.1, and a two-tailed p < 0.05 was deemed to indicate statistical significance.
Results
Baseline characteristics of participants
Among 485 MG patients treated with prednisone and tacrolimus in our center, 83 patients were resistant to tacrolimus and 27 patients discontinued tacrolimus due to severe adverse events after a median of 3.0 months (range = 1.0–20.0 months) (Figure 1). These patients were excluded from the study, and a total of 256 patients [median (IQR) age at onset: 26.9 (5.9–46.6) years; 65.1% female] were enrolled in the study, with a follow-up for a median of 2.9 years (IQR = 2.2–4.1). According to the diagnostic tests of MG, there are 196 (76.6%) MG patients with positive AChR-ab, 8 (3.1%) SNMG patients with positive MuSK-ab, 19 (7.4%) SNMG patients with positive RNS, and 33 (12.9%) SNMG patients without any electrophysiological or serological evidence of MG (seen in Supplementary Table S1). At the initial stage, ocular MG was present in 162 patients, 72 of whom converted to generalized myasthenia gravis(GMG) after a median of 0.96 years (IQR = 0.17–6.69). Before tacrolimus treatment, the maximum disease severity was classified as ocular MG (MGFA class I) in 90 patients (35.2%), mild MG (MGFA class II) in 80 patients (31.2%), and moderate or severe MG (MGFA class III–V) in 86 patients (33.6%). The basic clinical data of the 256 study patients are summarized in Table 1.
Baseline characteristics of 256 patients with remission after adding tacrolimus.

AChR-ab, anti-acetylcholine receptor antibody; AID, autoimmune disease; CSR, complete stable remission; MG, myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America; MuSK-ab, anti-muscle-specific kinase antibody; Pre, prednisone; QMG, quantitative myasthenia gravis; RNS, repetitive nerve stimulation; Tac, tacrolimus.
Data are given as n (%), median (interquartile range), or mean value ± standard deviation.
Because only patients with ocular forms at onset can develop a generalized disease, the denominators are the number of patients with ocular forms at onset.
The AChR-ab titers >0.50 nmol/l and MuSK-ab titers >0.05 nmol/l were defined as positive (RIA kit, RSR Limited, Cardiff, UK).
Thymus status was evaluated by chest computed tomography (CT) scan in nonthymectomized patients and thymus histology in thymectomized patients.
Remission and prednisone discontinuation
The patients achieved remission after a mean time of 2.1 ± 1.4 months, with a mean reduction of 8.0 ± 4.3 in QMG scores. In multivariate linear regression analysis, female sex, QMG scores, and tacrolimus concentrations were found to be independent predictors of the time to remission (Table 2). Tacrolimus concentration was correlated with the reduction in QMG scores by Spearman’s test (p = 0.029, r = −0.137).
Multiple linear regression model for the influencing factors of the time to remission.

AChR-ab, anti-acetylcholine receptor antibody; AID, autoimmune disease; GMG, generalized myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America; Pre, prednisone; QMG, quantitative myasthenia gravis; Tac, tacrolimus.
There was a strong correlation between the duration of prednisone therapy before tacrolimus initiation and the QMG scores at tacrolimus administration (Spearman’s correlation coefficient = −0.366, p < 0.001).
p < 0.05.
Before tacrolimus administration, all patients had been on prednisone for a median (IQR) duration of 0.3 (0.0–2.7) years. The prednisone dose decreased significantly after the addition of tacrolimus, at a speed of 0.97 mg/month, from a mean of 22.87 ± 12.14 mg/day at baseline to 3.07 ± 5.08 mg/day at the final visit (p < 0.001). Prednisone was eventually withdrawn from 167 patients (65.2%) after a mean time of 1.24 ± 1.10 years (Figure 2). The 256 patients were further divided into two groups: prednisone discontinuation group (n = 167) and nondiscontinuation group (n = 88). The clinical data of the two groups were available in Supplementary Table S2. Age at onset, initial symptoms, concomitant AID, AChR-ab titers, MGFA classification, age at tacrolimus administration, and the periods of follow-up were found to be associated with the prednisone discontinuation using univariate logistic regression analysis. Finally, multivariate logistic regression analysis indicated that concomitant AID [odds ratio (OR) = 0.312, 95% confidence interval (CI) 0.163–0.599; p < 0.001] and AChR-ab levels (OR = 0.912, 95% CI = 0.864–0.962; p = 0.001) were independent predictors of prednisone discontinuation (Table 3).

The Kaplan–Meier curve for time to discontinue prednisone in MG patients. Regression line (solid) and 95% confidence limits (dotted) are shown.
Univariate and multivariate analyses for the influencing factors of prednisone discontinuation.
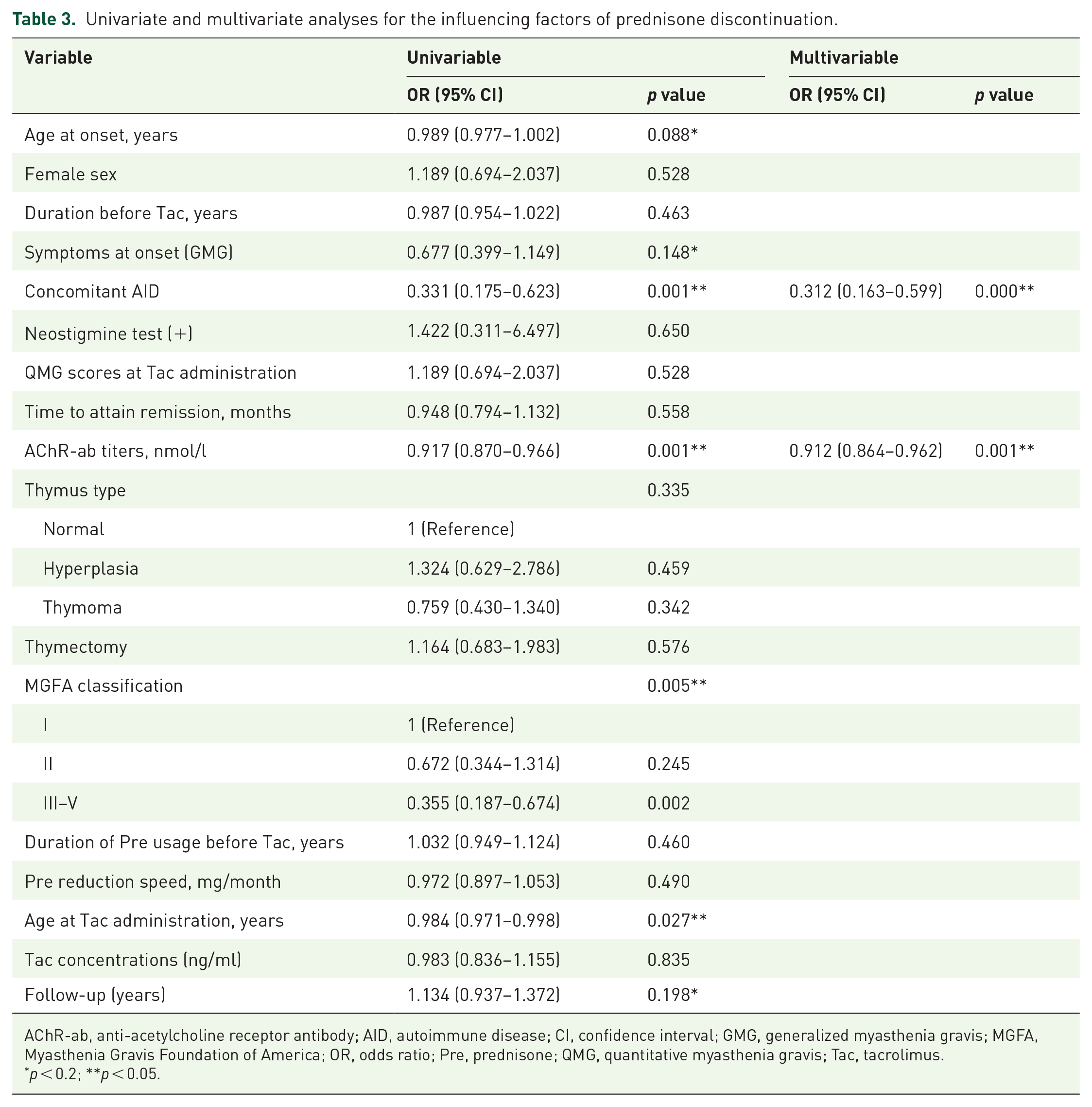
AChR-ab, anti-acetylcholine receptor antibody; AID, autoimmune disease; CI, confidence interval; GMG, generalized myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America; OR, odds ratio; Pre, prednisone; QMG, quantitative myasthenia gravis; Tac, tacrolimus.
p < 0.2; **p < 0.05.
Tacrolimus reduction–associated relapse
All 256 patients received a daily dose of 2–3 mg of tacrolimus with a mean trough concentration of 5.58 ± 1.59 ng/ml. One hundred nine of 256 (42.5%) patients who were well controlled with tacrolimus underwent a taper, with a follow-up for a median of 1.6 years (range = 0.5–6.7) (Table 4). These patients were divided into two groups: the relapsed MG group (n = 53) and the nonrelapsed MG group (n = 56), and the clinical data of the two groups were available in Supplementary Table S3. All patients had no symptoms or signs of MG before tacrolimus reduction. The QMG scores for 53 MG relapsed patients significantly increase at the time of relapse compared with that in baseline, with a mean QMG score of 9.6 ± 5.6 points (range = 3–24 points). The mean lag time from tacrolimus reduction to relapse in relapsed patients was 2.1 ± 1.6 months (range = 0.4–6.0 months). Univariate results showed that age at onset, sex, concomitant AID, AChR-ab titers, combination with prednisone, age at tacrolimus administration, and tacrolimus reduction speed were all associated with reduction-associated relapse. In the multivariate model, only tacrolimus reduction speed (OR = 5.662, 95% CI = 2.613–12.267; p < 0.001) remained significant (Table 5). The best cut-off value determined in an ROC curve analysis for the tacrolimus reduction speed was 0.76 mg/year (sensitivity = 90.6%; specificity = 76.8%) (shown in Figure 3).
Baseline characteristics of 109 patients with tacrolimus reduction.
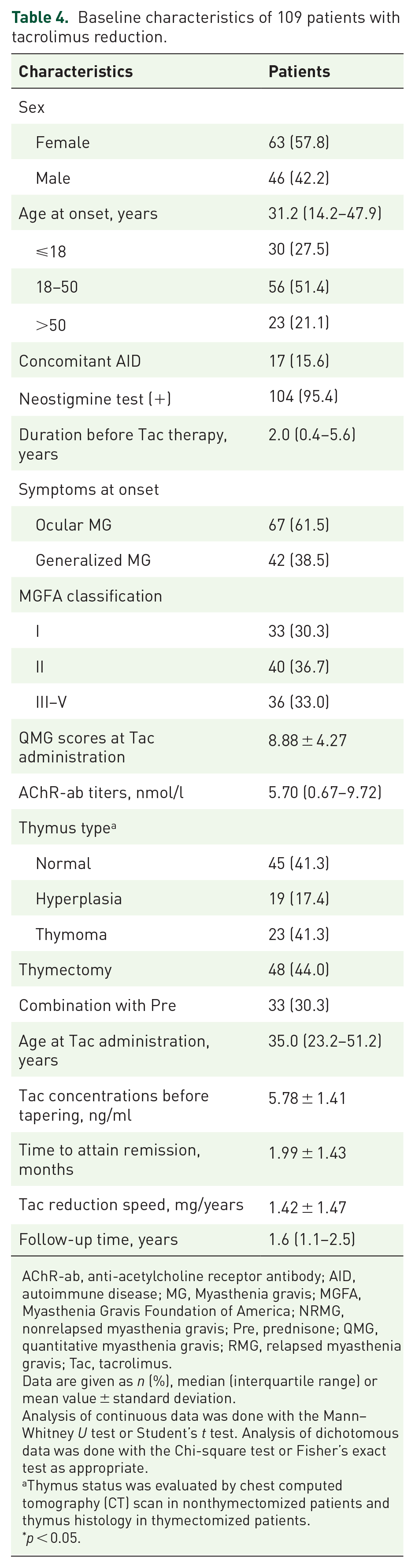
AChR-ab, anti-acetylcholine receptor antibody; AID, autoimmune disease; MG, Myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America; NRMG, nonrelapsed myasthenia gravis; Pre, prednisone; QMG, quantitative myasthenia gravis; RMG, relapsed myasthenia gravis; Tac, tacrolimus.
Data are given as n (%), median (interquartile range) or mean value ± standard deviation.
Analysis of continuous data was done with the Mann–Whitney U test or Student’s t test. Analysis of dichotomous data was done with the Chi-square test or Fisher’s exact test as appropriate.
Thymus status was evaluated by chest computed tomography (CT) scan in nonthymectomized patients and thymus histology in thymectomized patients.
p < 0.05.
Univariate and multivariate analyses for the influencing factors of MG relapse during tapering of tacrolimus dose.

AChR-ab, anti-acetylcholine receptor antibody; AID, autoimmune disease; CI, confidence interval; GMG, generalized myasthenia gravis; MGFA, Myasthenia Gravis Foundation of America; OR, odds ratio; Pre, prednisone; QMG, quantitative myasthenia gravis; Tac, tacrolimus.
p < 0.2; **p < 0.05.

Receiver operating characteristic curves analysis for MG relapse after tapering tacrolimus. With regard to the speed of tacrolimus reduction, the AUC is 0.875 and 95% CI is 0.806–0.943.
Treatment outcome and prognosis
For 53 patients with tacrolimus reduction–associated relapse, symptoms were reversed in 45 (84.9%) patients within 2 months of increasing the tacrolimus dose to the previous maintenance level. Six (11.3%) patients, however, required hospitalization for treatment with intravenous immunoglobulin (IVIG), and two patients developed acquired resistance to tacrolimus. Fortunately, no patients experienced a respiratory crisis. In terms of the treatment outcome of patients treated with prednisone and tacrolimus, only 20 out of 256 (7.8%) patients enter CSR after a variable period, ranging from 1.46 to 6.07 years. No factors, however, were found significantly associated with CSR by multivariate logistic regression.
Discussion
This was a retrospective study of the clinical outcomes in a large and heterogeneous group of MG patients who achieved remission after receiving prednisone and tacrolimus over a long-term follow-up. Unlike other traditional immunosuppressants, such as azathioprine, mycophenolate, and methotrexate, which had a delayed therapeutic response between 3 and 12 months,1,2,16,17 our findings demonstrated that the improvement began soon after starting tacrolimus and peaked after a mean of nearly 2 months. Ponseti et al. 18 reported that in addition to changes in muscle strength, the rapid immunomodulatory effect of tacrolimus on MG patients could also be reflected by a progressive reduction of serum AChR-ab levels. In addition, considering that tacrolimus has a biological role to increase glucocorticoid receptor transactivity from cytoplasm to nucleus,9,18 the favorable early results in this study may be partially attributable to the facilitatory effect of this drug on steroids pharmacology. Importantly, our results suggested that abruptly discontinuing tacrolimus may increase the risk of MG relapse, lending credence to the hypothesis that tacrolimus plays a role in the maintenance of MG remission.1,10
Sex, QMG scores, and tacrolimus concentrations were statistically identified as clinical predictors of the time to remission in this study. Our findings revealed that females took longer than men to achieve remission after taking tacrolimus. This sex bias could be explained by the fact that sex hormones like estrogens or progesterone can aggravate the MG disease by promoting the production of AChR-ab and expansion of AChR-specific Th1 cells. 19 Furthermore, the QMG scores were primarily used to assess the therapeutic efficacy of MG. 17 This study demonstrated a negative correlation between tacrolimus concentration and absolute value reduction of QMG scores, indicating that the tacrolimus efficacy has been considered to be concentration-dependent in MG treatment, with an adequate tacrolimus concentration being more effective than low tacrolimus concentration. 8
In the case of MG patients who responded well to combined immunotherapy, there is often a tendency to taper steroids dose first due to concerns about side effects associated with long-term use. 5 Our data showed that 65% of patients were able to discontinue prednisone after responding well to tacrolimus. This result may suggest that tacrolimus has stronger immunosuppressive and prednisone-sparing effects than azathioprine 16 and cyclosporine. 17 However, because there were insufficient data to make specific recommendations regarding the comparison of steroid-sparing effects between different immunosuppressants, it was concluded that a larger, prospective, randomized controlled trial would be required. 20 Moreover, we found that complete discontinuation of prednisone was more likely to fail in patients with other AID or high AChR-ab levels. This observation may indicate that MG patients with associated AID or high AChR-ab levels have a more generalized autoimmune disturbance that necessitates more effective combined immunotherapy.21–24
Similarly, in studies of azathioprine 25 or mycophenolate mofetil dose tapering, 26 fast tapering was associated with an increased risk of exacerbations in well-controlled MG patients. Our data showed that the speed of oral tacrolimus reduction was the most important factor possibly related to the relapse of MG symptoms in the late phase. To avoid disease rebound, the tacrolimus dose should be tapered down slowly, not exceeding 0.76 mg/year. In this study, relapses occurred in nearly half of the patients with well-controlled MG after tapering tacrolimus, which is considerably higher than the 4% relapses in the series of Nishida et al. 6 This could be because the latter limited definition of exacerbations to 3 months after tacrolimus reduction. In addition, relapses typically occurred within 6 months of dose reduction (mean 2.1 ± 1.6 months), indicating that the improvement induced by tacrolimus does not usually last after tapering off. Thus, physicians should be cautious when rapidly tapering immunotherapy and conduct regular follow-ups to monitor for signs of recurrence in MG patients.5,26,27
Consistent with previous studies that medications reduction–associated exacerbations were often mild and rarely required hospitalization,6,25,26 the majority of relapsed patients (84.9%) in our cohort achieved remission again within a few months after increasing tacrolimus dose. Notably, 2 of 53 relapsed patients developed resistance to tacrolimus and required more aggressive therapies, but the underlying mechanism for this observation remains unclear and needs to be further explored. 4 Furthermore, only 20 of 256 patients in this study achieved CSR at the last follow-up, which was similar to that of previous research works. 27 Mantegazza et al. 28 reported that factors influencing CSR included female sex, early onset age, and thymectomy therapy. No clinical factors, however, were found to be significantly associated with CSR in tacrolimus-treated MG patients.
Several limitations still exist in this study, for instance, (1) the treatment of tacrolimus among participants with intractable symptoms may contribute to selective bias; (2) despite the overall large size of our cohort, recruitment of subjects from a single center may not be highly representative; (3) the low AChR-ab titers in our cohort may be caused by population biases; (4) because of the lack of a control group in this study, the efficacy of tacrolimus in reducing QMG scores and prednisone dose needs to be further validated in long-term prospective randomized controlled trials.
Conclusion
In conclusion, our findings demonstrated that sex, tacrolimus concentrations, and QMG scores are clinically independent factors influencing time to remission in MG patients treated with tacrolimus. Although prednisone can be gradually tapered off in the majority of MG patients, it should be done with caution, particularly in patients with other AID or high serum titers of AChR-ab. Tacrolimus, as a maintenance drug to prevent disease relapses, should be tapered down slowly, not exceeding 0.76 mg/year.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221122538 – Supplemental material for Remission and relapses of myasthenia gravis on long-term tacrolimus: a retrospective cross-sectional study of a Chinese cohort
Supplemental material, sj-docx-1-taj-10.1177_20406223221122538 for Remission and relapses of myasthenia gravis on long-term tacrolimus: a retrospective cross-sectional study of a Chinese cohort by Zhuajin Bi, Yayun Cao, Chenchen Liu, Mengcui Gui, Jing Lin, Qing Zhang, Yue Li, Suqiong Ji and Bitao Bu in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.