
Abstract
Background:
Vagus nerve stimulation (VNS) is a therapeutic approach for patients with refractory postencephalitic epilepsy (PEE), which is characterized by drug resistance and disappointing surgical outcomes. However, the efficacy of VNS has not yet been studied in patients with refractory PEE. The present study aimed to demonstrate the efficacy of VNS and evaluate potential clinical predictors in patients with refractory PEE.
Methods:
We retrospectively collected the outcomes of VNS with at least a 1-year follow-up in all patients with refractory PEE. Subgroups were classified as responders and non-responders according to the efficacy of VNS (⩾50% or < 50% reduction in seizure frequency). Preoperative data were analyzed to screen for potential predictors of VNS responsiveness.
Results:
A total of 42 refractory PEE patients who underwent VNS therapy were enrolled, with an average age of 21.13 ± 9.70 years. Seizure frequency was reduced by more than 50% in 64.25% of patients, and 7.14% of patients achieved seizure-free events after VNS therapy. In addition, the response rates increased over time, with 40.5%, 50.0% and 57.1%, respectively at 6 months, 12 months, and 24 months after VNS therapy. Preoperative duration of epilepsy, monthly seizure frequency, and spatial distribution of interictal epileptic discharges (IEDs) were correlated with responders (p < 0.05) in the univariate analysis. Further multivariate regression analysis demonstrated that refractory PEE patients with high monthly seizure frequency or Focal IEDs (focal or multifocal epileptiform discharges) achieved better efficacy on VNS (p = 0.010, p = 0.003, respectively).
Conclusion:
VNS is an effective palliative therapy for patients with refractory PEE. Focal IEDs (focal or multifocal epileptiform discharges) and high seizure frequency were potential preoperative predictors of effectiveness after VNS therapy.
Keywords
Introduction
Encephalitis, including infectious and autoimmune encephalitis, is a neurological disorder with progressive encephalopathy and may lead to remote symptomatic epilepsy.1,2 The risk of unprovoked seizures in PEE patients is seven times higher than that in the general population. 2 Postencephalitic epilepsy (PEE) presents with at least one unprovoked seizure following the acute phase of encephalitis. 3 Appropriate antiepileptic drugs (AEDs) is effective for some patients with PEE; however, there are still 7%–15% intractable PEE patients without improvement. 4
In fact, the characteristics of refractory PPE are usually as follows: (a) PEE patients develop varied clinical seizure patterns and about 7%–15% of PEE patients show resistance to medical treatment;1,4–6 (b) there is a tendency for temporal focalization but precise seizure localization is difficult in PEE patients; 6 (c) even if clear mesial temporal sclerosis is demonstrated on brain magnetic resonance imaging (MRI), electroencephalogram (EEG) may detect multiple epileptogenic foci or diffuse brain dysfunction is revealed by neuropsychological testing, which is a negative prognostic factor for seizure remission; 7 and (d) approximately 59.1% of patients with refractory PEE tend to have unsatisfactory surgical outcomes, and these patients usually have bilateral or diffuse disease. 6 Therefore, refractory PEE has been regarded as a catastrophic postencephalitic epilepsy. For patients with refractory PEE, neuromodulations such as vagus nerve stimulation (VNS) may be a considerable therapeutic approach.
VNS is a minimally invasive and controllable treatment for patients with epilepsy, and there are approximately 45%–65% responders (⩾50% reduction in seizure frequency) after VNS therapy.8–12 In addition, indications,13–15 safety, and side effects16,17 of VNS therapy have been internationally validated and acknowledged. Some patient-related and epilepsy-related predictors with an impact on the prognosis of VNS therapy have been proposed.18–23 Significantly, VNS could also improve the cognition and quality of life in patients with epilepsy.19,24 Based on the advantages of VNS therapy, VNS may be an appropriate therapeutic choice for refractory PEE patients.25,26
Evidence suggests that precise seizure localization is difficult and the outcome of resection surgery is usually disappointing in refractory PEE patients,6,27 and the study which explores the efficacy and potential predictors of VNS has not yet been found in refractory PEE patients. The present study is the first to demonstrate the efficacy of VNS in 42 patients with refractory PEE and evaluated the potential predictors of responders.
Materials and methods
Definition of postencephalitic epilepsy, drug-resistant epilepsy
PEE was defined as at least one unprovoked seizure following acute encephalitis or meningitis according to the 2014 International League Against Epilepsy (ILAE). 3 However, it was difficult to determine the time criterion for the acute phase of encephalitis. Most studies applied the ongoing use AEDs as their time criteria, with variable time thresholds such as 6 months,25,28 12 months, 29 or 24 months. 5 According to the criterion of ILAE, the present study combined the history of encephalitis, EEG and auxiliary examinations to comprehensively diagnose PEE. 30 Minimum time threshold was set to 6 months in the present study, and all of the refractory PEE patients were required to continued AED use for ⩾ 6 months after acute encephalitis. Drug-resistant PEE was defined as ‘failure of adequate trials of two tolerated, appropriately chosen and used antiepileptic drug schedules (whether as monotherapies or in combination) to achieve sustained seizure freedom’ for PEE patients. 31
Patients
We retrospectively studied the effectiveness of VNS in patients with refractory PEE from Sanbo Brain Hospital, Capital Medical University between September 2008 and April 2020. All participants underwent examinations prior to VNS implantation, such as extraction of medical histories and clinical manifestations, long-term (interictal and ictal) scalp video-EEG, stereoelectroencephalography (SEEG), MRI, positron emission tomography (PET) and magnetoencephalography (MEG), and were determined as candidates for VNS therapy. VNS implantations were performed by two neurosurgeons according to standard procedures, 32 and the strategy for adjustment of stimulation parameters was based on available guidelines. 33 Patients were suggested for examination and adjustment of stimulation parameters within the first month after VNS therapy. They were then followed up every 3 months. All 42 patients received follow-up for at least 1 year after VNS therapy.
The present study was a retrospective study. The experimental group was the response group after VNS treatment, and the control group was the non-response group after VNS treatment. Whether the patients had focal IEDs before VNS operation was the main observation index. Based on previous literature, the proportion of patients with focal IEDs was estimated to be 72.4% in the response group and 24.1% in the non-response group. 34 Suppose α = 0.05, β = 0.10, N1/N2 = 2. According to PASS 15, the sample sizes of the response and non-response groups were calculated as N1 = 25 and N2 = 13, respectively. Finally, 27 patients were included in the response group and 15 patients in the non-response group.
The inclusion criteria for patients were as follows: (1) patients who had at least one unprovoked seizure following encephalitis and were diagnosed with PEE; (2) refractory PEE patients were identified as drug resistant, with no indications for resection surgery or disappointing surgical outcome (Engel class IV); (3) refractory PEE patients were candidates for VNS therapy and underwent VNS implantation; (4) normal neurodevelopment, no history of seizure and no family history of epilepsy prior to encephalitis were required for all participants; and (5) refractory PEE patients with VNS therapy were followed up for at least 1 year.
This study was compliant with the principles outlined in the Declaration of Helsinki and was approved by the ethics committee of the Sanbo Brain Hospital, Capital Medical University (SBNK-2017-15-01). All participants were informed of the purpose of the study, and written informed consent was obtained. For the children included, we obtained written informed consent from the next of kin, caretakers, or guardians on their behalf.
Clinical data collection
Medical histories of PEE patients were collected, including sex, etiology, age at encephalitis, latent period, age at VNS implantation, duration of epilepsy, seizure type and frequency, history of brain surgery, history of status epilepticus (SE) at encephalitis, duration of AED therapy, preoperative number of AEDs, spatial distribution of EEG and brain MRI. The etiology of refractory PEE was diagnosed based on clinical manifestations, cerebrospinal fluid examination and auxiliary examinations. We identified autoimmune encephalitis according to the 2016 diagnostic criteria of autoimmune encephalitis in the current study. 35 Latent period was defined as the duration from encephalitis to the first unprovoked seizure. The duration of epilepsy was defined as the period from the first unprovoked seizure to VNS implantation. The number of failed AEDs was categorized according to the preoperative AED regimen at the time of VNS implantation. Duration of AED therapy was defined as the period from initiation of AEDs following encephalitis to VNS implantation.
Seizure types were classified according to the 2017 ILAE Classification of the Epilepsies. 36 The outcomes of VNS therapy were determined using questionnaires when patients were readmitted for stimulation parameter adjustment, remote follow-up via telephone, WeChat, or other online approaches. The efficacy of VNS was evaluated according to the following equation: (baseline seizure frequency/month – seizure frequency/month with VNS) / (baseline seizure frequency/month) × 100%. In addition, the efficacy was classified by modified Engel and McHugh seizure outcome classification. 37 Responders were defined as 50% or greater reduction in seizure frequency after VNS therapy, compared to preoperative seizures under the predominant seizure type.38,39 After VNS therapy, outcomes of 6 months, 12 months, 24 months, and the last follow-up were collected. The last visit occurred before 24 months in a small number of patients. In addition, we analyzed the total efficacy and potential predictors of VNS based on the outcome at the last visit.
EEG and MRI acquisition
Patients were monitored using the standard 10–20 electrode placement system with 64 channels long-term video EEG in a quiet state. The major parameters of the Nicolet EEG system were set as follows: timebase, 30 mm/s; channels, 23; sensitivity, 150 μV/cm; high cut, 100 Hz; and low cut, 0.500 Hz. Spatial distributions of interictal epileptic discharges (IEDs) were classified as focal (including focal or multifocal epileptiform discharges only) and generalized. Several representative spatial distributions of IEDs were shown in Figure 1.

The representative EEG of refractory PEE patients. (a) Spike-and-wave discharges occurred simultaneously in the left central, parietal, and middle posterior temporal leads in focal IEDs, (b) medium to high amplitude spike-and-wave discharges in non-synchronous, paroxysmal, bilateral front head leads (FP1, F3, F7, M1, T3, FP2, F4, F8, M2, and T4) in multifocal IEDs, (c) irregular spike-and-wave and multi spikeand- wave discharges with medium to high amplitude were observed in the leads of both hemispheres synchronously and symmetrically in generalized IEDs.
Brain MRI with a 1.5 T magnet was performed in every refractory PEE patient before VNS implantation. The definite FLAIR/T2 abnormal signals suggested lesions. Based on the location of lesions and characteristic performances, the MRI results were classified as shown in Table 1. Additional methods included SEEG, PET, and MEG; however, the results of the measurements were not evaluated in the present study.
Factors associated with PEE patients: univariate analysis.

AEDs, antiepileptic drugs; EEG, electroencephalogram; Focal*, focal or multifocal; IEDs, Interictal epileptiform discharges; MRI, magnetic resonance images; SE, status epilepticus; VNS, vagus nerve stimulation.
P < 0.05.
Statistical analysis
Analyses were performed using SPSS (version 25.0) software. An independent t-test was used for continuous variables with normality, and the Mann–Whitney U-test was used for continuous variables without normality. Pearson χ2 and continuity correction tests were used to analyze categorical variables if appropriate. All statistical tests were two-tailed, and the significance was set at p < 0.05. Mean ± SD was shown for the continuous variable with normality, and median (interquartile range, IQR) for the continuous variable without normality. Categorical variables are represented as percentages. The relevance between VNS effectiveness and variables with significant differences in the univariate analysis was determined by multiple logistic regression.
Results
Demographic characteristics
The overall flow of patients is shown in Figure 2. All 77 refractory PEE patients with VNS implantation were collected, and 2 cases were excluded for stimulator removal (1 case with postoperative infection and 1 case with postoperative fat liquefaction). Thirty-three patients were excluded because their follow-up time was less than 1 year. The present study was based on the remaining 42 patients with refractory PEE (29 men and 13 women) managed during 2008–2020. No serious adverse effects were reported in the enrolled patients.
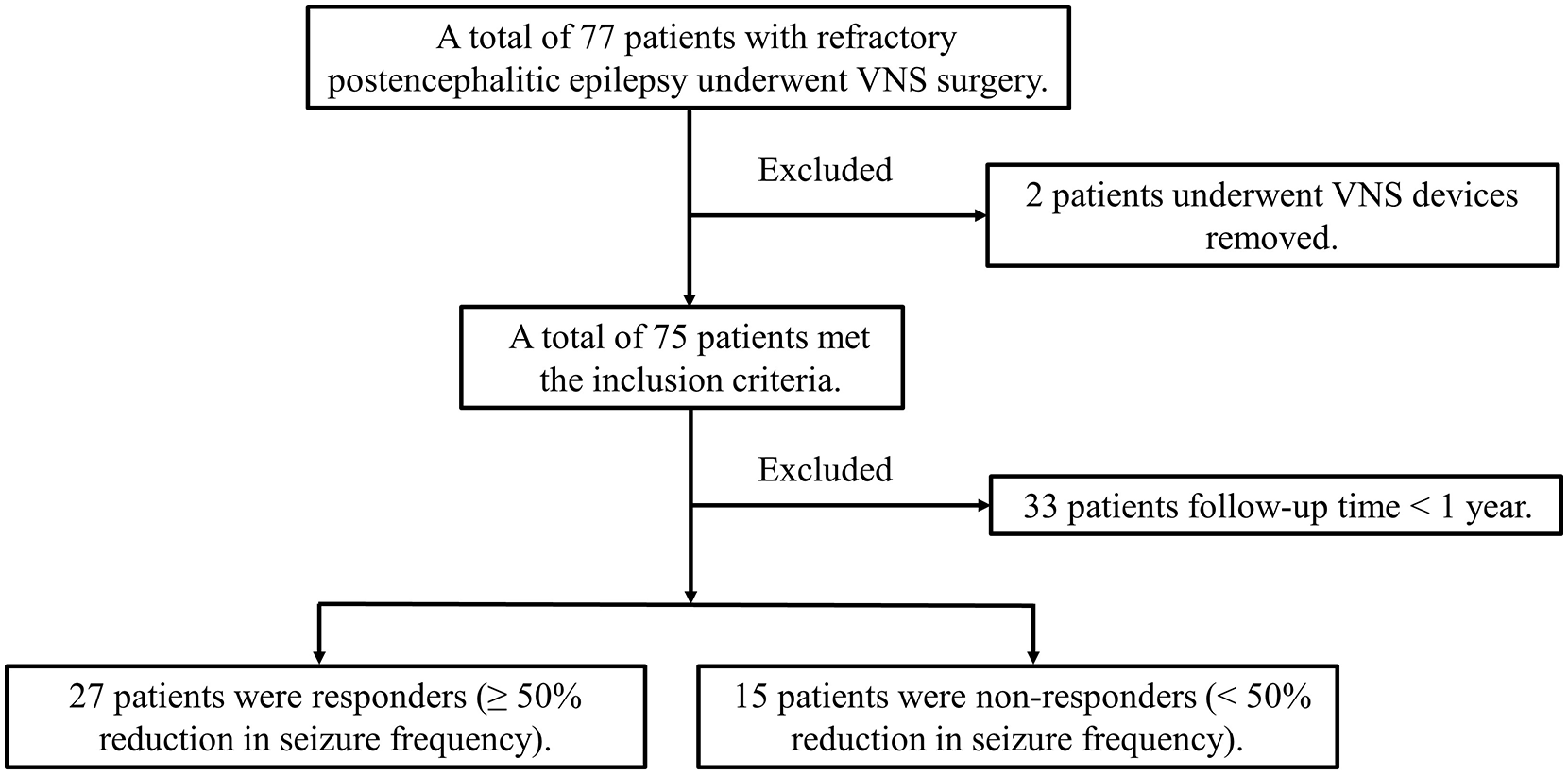
Flow chart. Flow chart for recruiting patients who satisfied the inclusion and exclusion criteria.
The mean age of the recruited refractory PEE patients was 18.05 ± 10.08 (range 2.2–43.2) years at the time of VNS implantation. Viral encephalitis was diagnosed in 90.48% (38 patients) of encephalitis patients; in addition, patients with bacterial and fungal encephalitis accounted for 7.14% (3 patients) and 2.38% (1 patient), respectively. None of the patients fulfilled the diagnostic criteria for autoimmune encephalitis. We found that the median age at encephalitis was 7.00 (IQR: 2.38–11.48) years, and only three patients had SE following encephalitis. In 23.81% (10 patients) of refractory PEE patients, they received brain surgery before VNS therapy. The median latent period, age at the first seizure after encephalitis, and duration of epilepsy was 0.05 (IQR: 0.00–1.25) months, 8.80 (IQR: 3.80–12.08) years and 3.50 (IQR: 1.00–8.25) years, respectively.
As shown in Table 1, the correlation between the variables mentioned above and VNS responders was analyzed by univariate analysis. The relevance between the duration of epilepsy and the responders was interesting. Univariate analysis revealed a significant difference (p = 0.028, Table 1); however, further multivariate logistic regression analysis showed no significant difference (p = 0.405, OR = 0.955, Table 2). Except for the duration of epilepsy, no evidence was found between the responders and other variables.
Predictors of efficacy for VNS in PEE patients on multivariate analysis.

CI, confidence interval; IEDs, interictal epileptiform discharges; OR, odds ratio; PEE, postencephalitic epilepsy; VNS, vagus nerve stimulation.
P < 0.05.
Outcomes of VNS
To evaluate the effectiveness of VNS, the clinical manifestations of all patients were followed and analyzed using the equation mentioned above. The median time of the last follow-up was 2.71 (IQR: 1.73–3.85) years for all participants, ranging from 1.00 to 11.83 years. The last follow-up outcomes of VNS therapy showed that seizures were reduced in 34 (80.95%) refractory PEE patients, ⩾ 50% reduction in seizure occurred in 27 patients (64.29%), and seizure-free events occurred in three patients (7.14%). Based on data from the last follow-up, McHugh and modified Engel seizure outcome classifications were used to specifically demonstrate the effectiveness of VNS therapy (Table 3). The McHugh scale showed that 45.24% of patients with refractory PEE were class I, 19.05% were class II, 14.28% were class III, and 21.43% were class IV–V. The modified Engel scale found that 7.14% of patients with refractory PEE were class I, 16.67% were class II, 40.48% were class III, and 35.71% were class IV.
Seizure control outcomes by modified Engel and McHugh seizure outcome classifications.
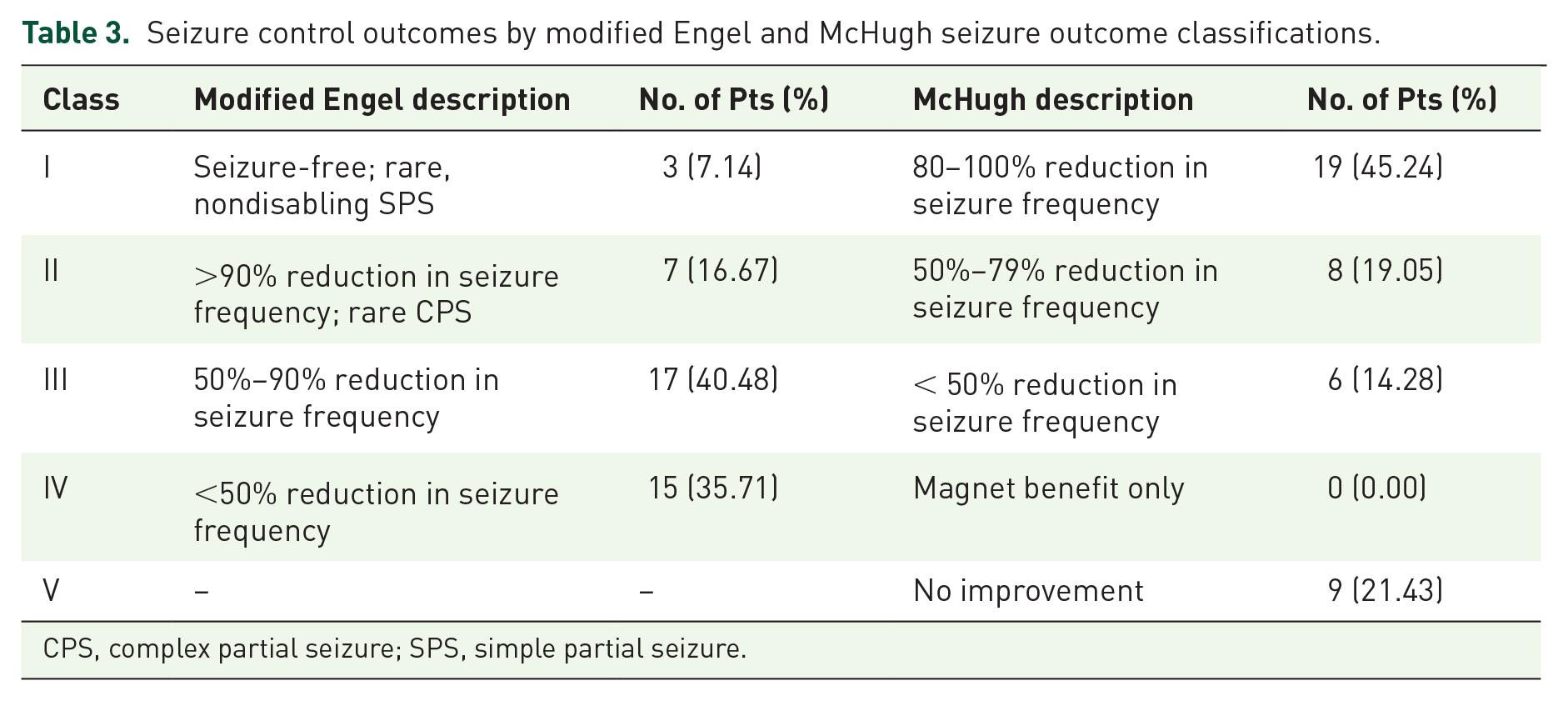
CPS, complex partial seizure; SPS, simple partial seizure.
After VNS therapy, the outcomes of 42 recruited patients were shown at 6- and 12-month follow-ups, and only 28 patients were shown at 24-month follow-ups (Figure 3). Six months after VNS therapy, 17 of 42 (40.5%) patients experienced ⩾ 50% seizure reduction. After 1 year, the number increased to 21 of 42 (50.0%) and at 2 years it was 16 of 28 (57.1%). Out of the 25 non-responders after 6 months, 7 patients (28.0%) had a ⩾ 50% reduction in seizure frequency at one year. Of the 21 non-responders after 1 year, 4 patients (9.5%) had a ⩾ 50% seizure frequency reduction at 2 years. Moreover, the outcomes at one year showed that out of 14 patients without improvement after six months, three patients (21.4%) had a ⩾ 50% seizure frequency reduction, and two patients (14.3%) had a reduction of < 50%. The outcomes at two years showed that out of 12 patients without improvement after one year, two patients (16.7%) had a ⩾ 50% seizure frequency reduction, and two patients (16.7%) had a reduction of < 50%. Three out of 17 patients (17.6%) who reported a ⩾ 50% seizure reduction after six months returned as non-responders after 1 year, and 6 out of 21 patients (28.6%) who reported a ⩾ 50% seizure reduction after one year returned as non-responders after two years. Only three patients became seizure-free throughout the study period.
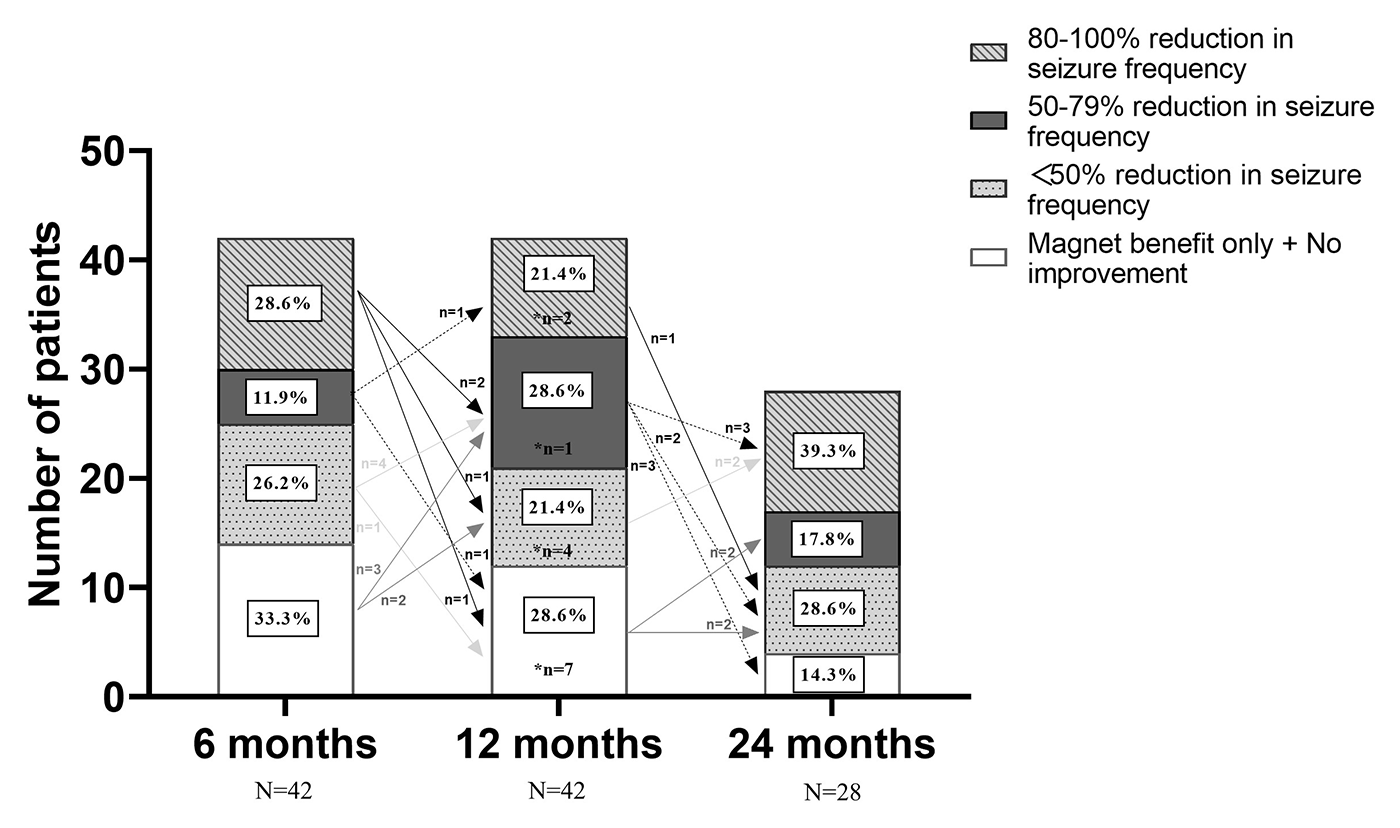
McHugh outcome classification. Seizure outcomes at 6-, 12-, and 24-month follow-up after VNS therapy with McHugh outcome classification. Arrows indicate changes in VNS effectiveness between follow-ups. *Patients lost to follow-up.
Correlation of outcomes with clinical characteristics
With regard to monthly seizure frequency, we divided the monthly frequency into the low frequency group (⩽ 24 times per month), low to medium frequency group (> 24 times and ⩽ 45 times per month), medium to high frequency group (> 45 times and ⩽ 80 times per month), and high frequency group (> 80 times per month). Pearson χ2 and continuity correction chi-square tests were used to determine the significant difference in monthly seizure frequency. Further multivariate analysis found that high monthly seizure frequency was strongly associated with responders (p = 0.01, OR = 24.807, Table 2). Our findings demonstrated that a high monthly seizure frequency was an independent predictor of responder. However, there was no difference between responders and non-responders after VNS therapy with regard to seizure types and preoperative number of AEDs.
Correlation of outcomes with EEG and MRI
All results from preoperative EEG (interictal and ictal) and MRI were classified and analyzed. As shown in Table 1, 20 (47.62%) patients presented with Focal IEDs (focal or multifocal epileptiform discharges), with 17 responders and three non-responders; 22 (52.38%) patients presented with generalized IEDs, with 10 responders and 12 non-responders. A positive correlation (p = 0.008, Table 1) was observed between responders and the spatial distribution of IEDs after univariate Pearson χ2 analysis. Further analysis revealed, remarkably, that there was a significant correlation between responders and focal or multifocal epileptiform discharges (p = 0.003, OR = 14.961, Table 2). Our results suggests that refractory PEE patients with preoperative Focal IEDs (focal or multifocal epileptiform discharges) may be candidates for better outcomes of VNS therapy. Ictal onset rhythms of EEG and different MRI manifestations all explored the differences between responders and non-responders (Table 1). However, none of these differences was statistically significant.
Discussion
VNS therapy has been used in patients with catastrophic PEE who are drug resistant and cannot be relieved by surgery. We analyzed data from refractory PEE patients who received VNS therapy and found that VNS was an effective approach to improve seizures in patients. Further analysis determined two independent preoperative predictors of VNS effectiveness, including high monthly seizure frequency and Focal IEDs (focal or multifocal epileptiform discharges).
One of the major findings in this study was that VNS relieved seizures in 80.96% of refractory PEE patients, with 64.29% responders and 7.14% seizure-free patients. The detailed effectiveness classifications are shown in Table 3 according to McHugh and Engel. A study reviewed 30 years of reported studies on VNS and showed that the response rates (the percentage of responders) reached 45%–65% (ranging from 22.0% to 74.3%) in most published studies. 11 Consistent with previous studies, the response rate in the current study reached 64.29%, indicating that VNS was an effective palliative therapy for refractory PEE patients.
Conversely, the response rates (including seizure-free patients) at 6, 12, and 24 months were reviewed and presented with 40.5%, 50.0%, and 57.1%, respectively. Our findings showed that the response rate increased at 12 and 24 months after VNS therapy. The efficacy of VNS increases over time. The increasing trend in VNS efficacy over time has also been elucidated in other studies.4,40,41 A study on VNS therapy with 20 PEE patients showed that the effective rate at 3, 6, and 12 months respectively reached 30%, 45%, and 70% and found that the grand total EEG score children with PEE could be improved after a 1-year VNS therapy. 4 This trend was studied on a prospective study of 362 drug resistant patients with epilepsy, and the result demonstrated that the response rates of VNS therapy at 3, 6, 12, 24 and 36 months were respectively 38.9%, 46.8%, 55.8%, 57.7%, and 58.8%. 40 Another study of 30 children with drug resistant epilepsy proposed that the response rates at 6, 12, and 24 months were respectively 38%, 43%, and 42%. 41 In addition, based on the time points chosen for the present study, we observed that more than 50% of refractory PEE patients with VNS therapy achieved more than 50% seizure remission at 12 months, which was the same as in studies of 20 patients with PEE and 362 patients with drug resistant epilepsy.4,40 Comparison of our findings with other studies above confirmed that the curative effect of VNS improves over time. In fact, an additional uncontrolled factor was that 11 non-responders patients lacked data on outcomes at 24 months, but only three responder patients did not. Additional studies with longer follow-up periods and larger samples may be needed to minimize these factors.
In fact, the effectiveness of VNS therapy was explored in some specific indications, such as genetic generalized epilepsy (GGE), 13 Lennox–Gastaut syndrome (LGS),42–44 and Dravet syndrome (DS).15,45 After VNS therapy, 64.7% (n = 11) responders of patients with GGE and 41.4% (n = 12) responders of patients with LGS were found. 13 Another study on LGS showed that the efficacy of VNS therapy was considerable, in which 113 patients with LGS were reviewed and yielded a 55% responder rate. 44 Response rates of patients with LGS who underwent VNS implantation respectively reached 55%, 67.7%, and 65% at 6, 12 and 24 months. 43 For VNS therapy on DS, a meta-analysis reviewed 13 studies and found that 52.9% of patients experienced a ⩾ 50% reduction of seizures. 15 A retrospective study enrolled 20 children with DS demonstrated that VNS therapy could control seizures in a time-dependent manner, with response rates of 36.4%, 54.5%, and 63.2% at 12, 24, and 36, respectively. 45 The result of the current study was different compared with other studies on specific indications. We supposed that the observed difference may be due to the small cohort of participants.
The clinically relevant finding was that preoperative high seizure frequency (> 80 times per month), as an independent predictor, was strongly associated with responders of refractory PEE patients (p = 0.01, OR = 24.807). A retrospective study collected epileptic characteristics from 80 children with drug-resistant epilepsy and demonstrated that high seizure frequency (> 80 times per month) was determined as the predictor of VNS effectiveness compared to other groups with lower seizure frequency after classification and regression tree analysis. 46 Another study indicated that patients with initial higher seizure burdens at baseline responded more consistently to VNS by multiple regression analysis. 47 Based on the studies above, we divided patients into four groups and obtained consistent conclusions. A similar result was also shown in a previous study of medication-resistant generalized epilepsy, multiple regression analysis found that patients with higher baseline seizure rates had better responses to VNS. 48 However, another study 49 proposed that a higher baseline seizure rate was not a positive predictor of VNS responsiveness, which was different from our finding. Given that the specific mechanism of VNS therapy is not clear, different results should be interpreted comprehensively, such as the influence of differences in follow-up time and variable patient settings. Further studies on seizure frequency that take these variables into account may need to be undertaken.
To determine the optimal VNS therapy for patients with epilepsy, many studies have explored and indicated the relevance between responsiveness to VNS and electrical seizure patterns (interictal and ictal). 50 Another notable aspect of our study similarly focused on the issue, and found that focal or multifocal epileptiform discharges showed significant correlation with VNS responders of refractory PEE patients (p = 0.003, OR = 14.961). Prior studies have noted the importance of IEDs, for example, a study included 144 patients with medically intractable epilepsy, and concluded that unilateral IEDs significantly associated with seizure free events after VNS therapy. 51 Another study also indicated that the absence of only bilateral IEDs was correlated with seizure-free events, and explained that bilateral synchronous IEDs arising from the interaction of multiple foci presented with a higher degree of epileptogenicity. 52 Likewise, compared to generalized IEDs in patients with drug resistance, the patients with focal or only multifocal IEDs could achieve better benefit from VNS therapy.22,34 These results were in agreement with those obtained in this study, and our results suggested that refractory PEE patients with focal or multifocal epileptiform discharges presenting with lower epileptogenicity could be better candidates for responders after VNS therapy.
Surprisingly, the duration of epilepsy was not identified as an independent predictor of responders in refractory PEE patients through multivariate analysis, even if significant relevance was found in the univariate analysis. This discrepancy could be attributed to the confounding effect of other variables, such as history of brain surgery, duration and types of AED therapy. In fact, some studies have proposed some positive predictors of better VNS efficacy, such as duration of epilepsy, 53 age at VNS implantation, 54 seizure type, 21 and the presence of lesions on MRI, 50 and genetic variations of adenosine kinase. 55 Contrary to predictors mentioned by other studies, our findings showed no significant difference. Therefore, future studies on these different conclusions are required.
The current study had some limitations. First, the inherent biases of the retrospective design cannot be ruled out in this single-center study. Second, a relatively small cohort of participants was included in the present study, and larger samples in the future could be improved to draw more definite conclusions. Third, this study did not obtain evaluation of cognition and quality of life that is important for VNS therapy of refractory PEE patients. Finally, the influence of clinical variables could not be completely controlled in the present study. Although these limitations were recognized, this study strengthens the idea that VNS could be considered as an effective therapy for refractory PEE patients, and that high preoperative seizure frequency and Focal IEDs (focal or multifocal epileptiform discharges) may be two independent predictors of better outcomes.
Conclusion
The present study demonstrated that 64.29% of patients with refractory PEE had a reduction in seizure frequency of more than 50% after VNS therapy, and the efficacy increased over time. Notably, our findings suggest that refractory PEE patients with preoperative high seizure frequency or Focal IEDs (focal or multifocal epileptiform discharges) were strongly correlated with better outcomes of VNS therapy.
Footnotes
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Natural Science Foundation of China (Grant No. 81571275 and No.11932003).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.