
Abstract
Background:
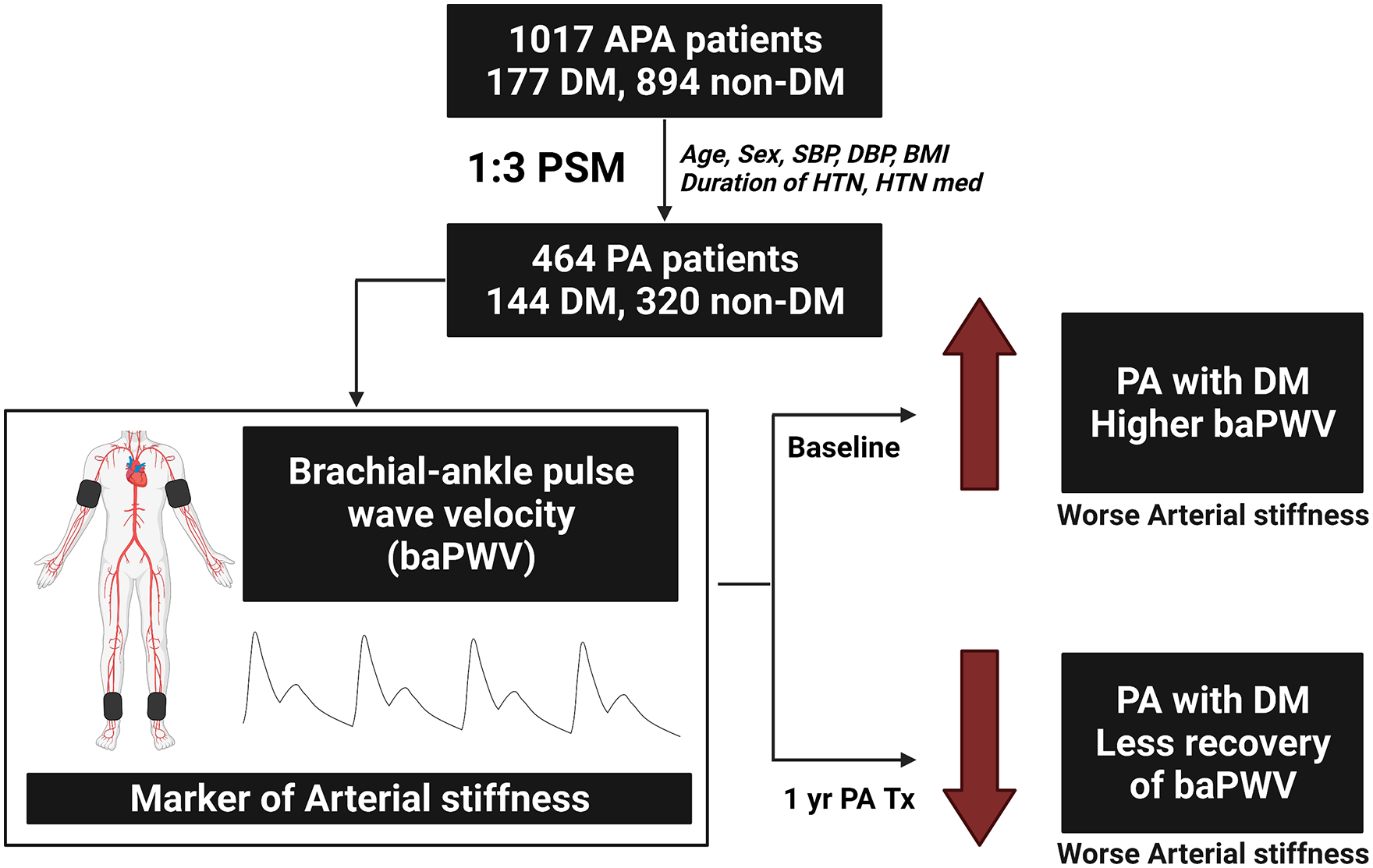
Aldosterone excess in primary aldosteronism (PA) has been linked to insulin resistance, and diabetes mellitus has been associated with increased arterial stiffness and worse cardiovascular outcomes. However, the impact of diabetes on baseline and post-treatment arterial stiffness in patients with PA is unknown.
Methods:
This study prospectively enrolled 1071 PA patients, of whom 177 had diabetes and 894 did not. Clinical, biochemical, and brachial-ankle pulse wave velocity (baPWV) data were analyzed at baseline and 1 year after PA-specific treatment. After propensity score matching of age, sex, body mass index, systolic and diastolic blood pressure, hypertension duration, and number of antihypertensive medications, 144 patients with diabetes and 320 without diabetes were included for further analysis.
Results:
After propensity score matching, the baseline characteristics were balanced between the diabetes and nondiabetes groups except for fasting glucose, HbA1c, and lipid profiles. The patients with diabetes had significantly worse baseline baPWV compared with those without diabetes. After multivariable linear regression, the presence of diabetes mellitus remained a significant predictor of worse baseline mean baPWV (β: 46.3, 95% confidence interval: 2.9–89.7, p = 0.037). After 1 year of PA-specific treatment, only the nondiabetes group had significant recovery of mean baPWV (1661.8 ± 332.3 to 1565.0 ± 329.2 cm/s, p < 0.001; Δ = −96.8 ± 254.6 cm/s). In contrast, the diabetes group had less improvement (1771.2 ± 353.8 cm/s to 1742.0 ± 377.2 cm/s, p = 0.259; Δ = −29.2 ± 263.2 cm/s) even though the systolic and diastolic blood pressure significantly improved in both groups.
Conclusion:
The presence of diabetes mellitus in PA patients was associated with worse baseline and less post-treatment recovery of arterial stiffness.
Keywords
Central illustration
Introduction
Primary aldosteronism (PA) is an important cause of hypertension and accounts for at least 4% of patients with newly diagnosed hypertension, and up to 23% of PA patients have resistant hypertension.1–3 PA patients have excessive autonomous aldosterone production which is unresponsive to renin regulation, and aldosterone overproduction is associated with diabetes mellitus (DM) and metabolic syndrome.4,5 Several studies have reported higher prevalence of insulin resistance and DM in patients with PA compared with those with essential hypertension.5,6 Since DM and PA are both independent predictors of worse cardiovascular outcomes, the presence of DM in PA would be expected to have additional detrimental effects on the cardiovascular system.
Arterial stiffness is a good marker to detect subclinical cardiovascular disease, and it has been reported to be an independent predictor of long-term cardiovascular events.7,8 Increased arterial stiffness results in widening of the arterial pulse pressure, altering vessel flow dynamics, increasing shear force and subsequently endothelial dysfunction and vascular disease.9,10 Arterial stiffness can be assessed noninvasively by measuring brachial-ankle pulse wave velocity (baPWV), which is a simple and reproducible method. 11 In the Framingham Heart Study, higher arterial stiffness assessed by pulse wave velocity (PWV) was associated with an increased risk of cardiovascular events. 12 The arteries of diabetic patients appear to age at an accelerated rate and these patients have worse PWV. 13 Furthermore, increased PWV is strongly associated with mortality in DM patients. 14 In addition, aldosterone excess in PA has been shown to contribute to increased vascular fibrosis and cellular hypertrophy, which also results in arterial stiffness.15–18 However, the interplay of PA and concurrent DM on arterial stiffness and its effects on treatment outcomes remain unknown. Therefore, the aim of this study was to investigate the effects of DM on baseline and post-treatment baPWV in PA patients.
Materials and methods
The authors declare that all supporting data are available within the article.
Patients
We prospectively enrolled patients with PA from June 2006 to April 2020 at National Taiwan University Hospital. The PA patients were all registered in the Taiwan Primary Aldosteronism Investigation (TAIPAI) database. The inclusion criteria were: (1) patients with confirmed diagnosis of PA; 19 (2) patients had baseline baPWV analysis at enrollment; (3) patients had screening of DM at enrollement. 20 The exclusion criteria were: (1) patients age <18 years old; (2) patients unwilling to participate in the study. The patients’ medical information, including demographics, biochemistry and medications were recorded at enrollment and at scheduled follow-up periods. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were obtained using a sphygmomanometer according to clinical guidelines. Comprehensive evaluations including blood pressure, laboratory studies, and baPWV were performed at enrollment. Patients who received follow-up baPWV analysis 12 months after PA-specific treatment including mineralocorticoid receptor antagonists and adrenalectomy were selected to evaluate the treatment effects on arterial stiffness. The diagnoses of PA and DM were made according to the guidelines.19,20 This study was approved by the Institutional Review Board of National Taiwan University Hospital and was performed in accordance with relevant guidelines and regulations. Informed consent was obtained from all patients before enrollment.
Laboratory measurements of aldosterone and cortisol
Plasma aldosterone concentration (PAC) was measured using a radioimmunoassay with a commercial kit (Aldosterone Maia Kit; Adaltis Italia S.P.A., Bologna, Italy), and plasma renin activity (PRA) was measured as the generation of angiotensin-I in vitro using a commercially available radioimmunoassay kit (Cisbio, Bedford, Massachusetts, USA). Aldosterone-to-renin ratio (ARR) was calculated as the PAC divided by the PRA. All antihypertensive medications were discontinued for at least 21 days before measuring plasma PRA and PAC as suggested in clinical guidelines. 19
Diagnostic criteria for primary aldosteronism and subtype identification
The confirmation and diagnosis of PA and further identification of aldosterone-producing adenoma (APA) were made according to previously published protocols and algorithms. 19 Patients who met the following three criteria were defined as having PA: (1) autonomous excess aldosterone production with an ARR > 35; (2) a TAIPAI score > 60%; and (3) post-saline loading PAC > 10 ng/dl, or PAC/PRA > 35 (ng/dl)/(ng/ml per h) in a post-captopril test, or PAC > 6 ng/dl in a fludrocortisone suppression test. 19 APA was diagnosed in patients with PA and at least one of the following three conditions: (1) adenoma on a computed tomography scan for preoperative evaluation; (2) lateralization of aldosterone secretion evidenced by adrenal vein sampling or dexamethasone suppression NP-59 single photon emission computed tomography/ computed tomography; and (3) pathologically proven adenoma after surgery if the patients received an operation. 19 The choice of unilateral adrenalectomy or medical treatment with mineralocorticoid receptor antagonists was discussed with the APA patients, along with a pre-operational assessment. The PA patients were enrolled after consenting to the surgery and if they were physically suitable for adrenalectomy.
Predictors of interest
The predictors of interest were baseline and post-1-year PA-specific treatment baPWV. The baPWV was measured using an automatic waveform analyzer (Colin VP-2000, Omeron Inc., Japan) after the patients had been allowed to rest for 15 min in a supine position. 21 The waveforms of bilateral brachial arteries, phonocardiograms, and electrocardiograms were simultaneously recorded. Occlusive cuffs connected to oscillatory and plethysmographic sensors were wrapped around the upper arms and ankles to measure and analyze blood pressure and pulse waveforms. Differences in conduction times were estimated according to wave front theory. Right side, left side, and mean baPWV were measured as the distances between the brachial and ankle sites divided by the differences in conduction time.
Covariates
The explanatory variable of primary interest in this study was the presence or absence of DM. The covariates were sex, age, duration of hypertension, antihypertensive agents, number of antihypertensive medications, body mass index, SBP, DBP, aldosterone-producing adrenal adenoma or not, laboratory data, log PAC, log PRA, and log ARR.
Statistical analysis
There were no previous studies investigating the difference of baPWV in PA patients with or without diabetes. The difference of baPWV in patients with or without diabetes was used for sample size calculatio. 22
A minimum of 93 diabetic patients and 185 nondiabetic participants in the propensity score matched cohort were required to achieve a type I error of 1% and a power of 99%.
Because there were substantial differences in the clinical characteristics between the DM and non-DM groups, we conducted propensity score matching to balance the distribution of these clinical characteristics between the two groups. The propensity score was estimated using a multiple logistic regression model including the following possible confounding variables in the patients with and without DM: age, sex, body mass index, SBP, DBP, duration of hypertension, and number of antihypertensive medications. Each diabetic patient was matched to a maximum of three nondiabetic patients. The balance of covariates between the matched groups was subsequently examined. All continuous variables were presented as mean ± standard deviation. Nonnormally distributed variables (i.e. PAC, PRA and ARR) were presented as median and interquartile range. Differences between proportions were assessed using the chi-square test. Comparisons of continuous data between the two groups were conducted using the independent t test (for normally distributed variables) or the Mann–Whitney U test (for nonnormally distributed variables). Univariable linear regression analysis was performed to test the relationships between baPWV and clinical parameters. Significant determinants in the univariable linear regression analysis (p < 0.05) were analyzed using multivariable linear regression analysis to identify the significant factors associated with baPWV. The changes in clinical characteristics and PWV analysis before and after PA-specific treatment were assessed using the paired sample t test or Wilcoxon signed-rank test. These changes were compared between the DM and non-DM groups using the independent sample t test (for normally distributed variables) or Mann–Whitney U test (for nonnormally distributed variables).
We also examined potential linear and nonlinear relationships between baseline fasting glucose level and mean baPWV value (baseline value and the change before and after treatment). The baseline fasting glucose level was treated as a flexible variable using a restricted cubic spline (RCS) with three knots which were located in the 10th, 50th and 90th percentiles. A two-sided p value < 0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS for Windows, version 25.0 (SPSS, Inc., Chicago, IL), with the R-3.3 plugin extension for the propensity score analysis (the ‘Matchit’ package). The RCS analysis was carried out using R version 4.0.2 (R Development Core Team) with the ‘rms’ package (Version 6.2-0, updated on March 18, 2021).
Results
Patient characteristics and demographics
A total of 1071 PA patients were enrolled in this study, including 681 (63.6%) with aldosterone-producing adrenal adenoma and 390 (36.4%) with idiopathic bilateral adrenal hyperplasia. Of the 1071 enrolled PA patients, 177 (16.5%) had DM and 894 (83.5%) did not. The DM patients were significantly older, took more antihypertensive medications, and had significantly higher body mass index and SBP. The biochemistry data showed that the DM patients had significantly higher fasting blood glucose, HbA1c, triglyceride, and low-density lipoprotein levels, and significantly lower high-density lipoprotein level. The usage rates of angiotensin converting enzyme inhibitor, angiotensin receptor blocker, beta blocker, alpha blocker, calcium channel blocker, diuretic and mineralocorticoid receptor antagonist antihypertensive medications were all significantly higher in the DM patients, except for vasodilators. The baseline characteristics are shown in Table 1.
Baseline characteristics.

AC, glucose, fasting blood glucose; ACEI, angiotensin converting enzyme inhibitors; APA, aldosterone-producing adenoma; ARB, angiotensin receptor blockers; ARR, aldosterone-renin ratio; BMI, body mass index; CCB, calcium channel blocker; DBP, diastolic blood pressure; DM, diabetes mellitus; DPP-4, dipeptidyl peptidase 4; HDL, high-density lipoprotein; HTN, hypertension; LDL, low-density lipoprotein; MRA, mineralocorticoid receptor antagonist; PAC, plasma aldosterone concentration; PRA, plasma renin activity; PSM, propensity score matching; SBP, systolic blood pressure; SGLT-2, sodium-glucose cotransporter 2.
Values are expressed as mean ± SD, median (interquartile range), or number (percentage).
1:3 PSM with age, sex, BMI, SBP, DBP, Years of HTN, No. of HTN medication.
After propensity score matching, there were 76 DM patients matched to 228 non-DM patients, 24 DM patients matched to 48 non-DM patients, and 44 DM patients matched to 44 non-DM patients. All of the baseline characteristics and kinds of antihypertensive medications were well balanced except for the biochemistry profile after matching, and fasting blood glucose, HbA1c, triglyceride, and low-density lipoprotein were still significantly higher in the DM patients. The baseline characteristics after propensity score matching are shown in Table 1.
Baseline PWV analysis between the DM and non-DM patients
The DM patients had worse baseline right, left and mean PWV values: right baPWV [DM group: 1840.0 ± 401.6 cm/s versus non-DM group: 1670.1 ± 340.1, β: 169.9, 95% confidence interval (CI): 113.3–226.6, p < 0.001], left baPWV (DM group: 1835.3 ± 433.7 cm/s versus non-DM group: 1657.0 ± 413.2 cm/s, β: 178.3, 95% CI: 120.8–235.9, p < 0.001), and mean baPWV (DM group: 1837.4 ± 413.2 cm/s versus non-DM group: 1663.6 ± 335.2 cm/s, β: 173.8, 95% CI: 117.3–230.3, p < 0.001). The baseline baPWV data are shown in Table 2.
PWV analysis.

baPWV, brachial-ankle pulse wave velocity; CI, confidence interval; DM, diabetes mellitus; PSM, propensity score matching.
Values are expressed as mean ± SD.
1:3 PSM with age, sex, BMI, SBP, DBP, Years of HTN, No. of HTN medication.
After propensity score matching, the baseline right, left, and mean baPWV values remained significantly higher in the DM patients: right baPWV (DM group: 1790.5 ± 342.9 cm/s versus non-DM group: 1706.3 ± 348.1 cm/s, β: 84.2, 95% CI: 15.8–152.5, p = 0.016), left baPWV (DM group: 1785.2 ± 372.5 cm/s and non-DM group: 1693.9 ± 337.9 cm/s, β: 91.3, 95% CI: 22.3–160.3, p = 0.010), and mean baPWV (DM group: 1787.3 ± 354.4 cm/s versus and non-DM group: 1700.3 ± 339.2 cm/s, β: 86.9, 95% CI: 18.9–154.9, p = 0.012). The baseline baPWV data after propensity score matching are shown in Table 2 and Figure 1(a).
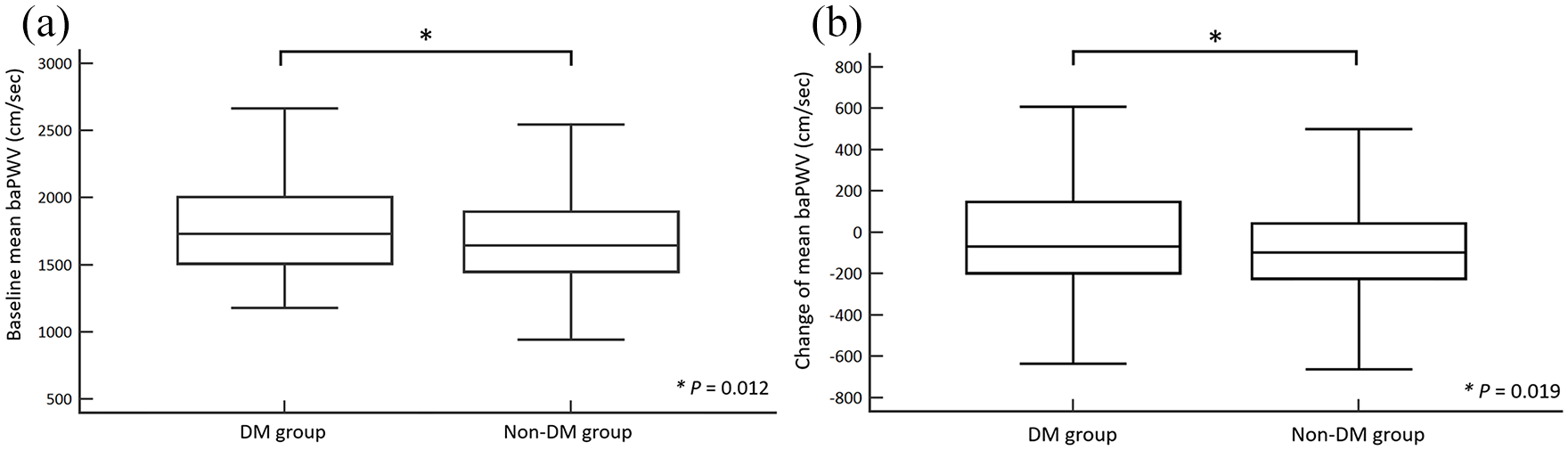
(a) Baseline mean baPWV in the DM and non-DM PA patients after propensity score matching. (b) The changes in mean baPWV in the DM and non-DM PA patients after 1 year of treatment.
Factors associated with baseline PWV
In univariable linear regression analysis, age, duration of hypertension, number of antihypertensive medications, SBP, DBP, and DM were significantly associated with higher baseline mean baPWV. In multivariable linear regression analysis, only age (β: 15.2, 95% CI: 13.7–16.4, p < 0.001), duration of hypertension (β: 2.6, 95% CI: 0.3–16.6, p = 0.027), SBP (β: 5.9, 95% CI: 5.1–6.6, p < 0.001), and DM (β: 46.3, 95% CI: 2.9–89.7, p = 0.037) remained in the model (Table 3). Of note, DBP was not included in the multivariable model due to its high collinearity with SBP.
Univariable and multivariable linear regression of predictors of worse mean baPWV.

APA, aldosterone-producing adenoma; ARR, aldosterone-renin ratio; BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; HTN, hypertension; PAC, plasma aldosterone concentration; PRA, plasma renin activity; SBP, systolic blood pressure.
DBP was not included in the multivariable model due to its high collinearity with SBP.
Clinical and PWV improvements after PA-specific treatment
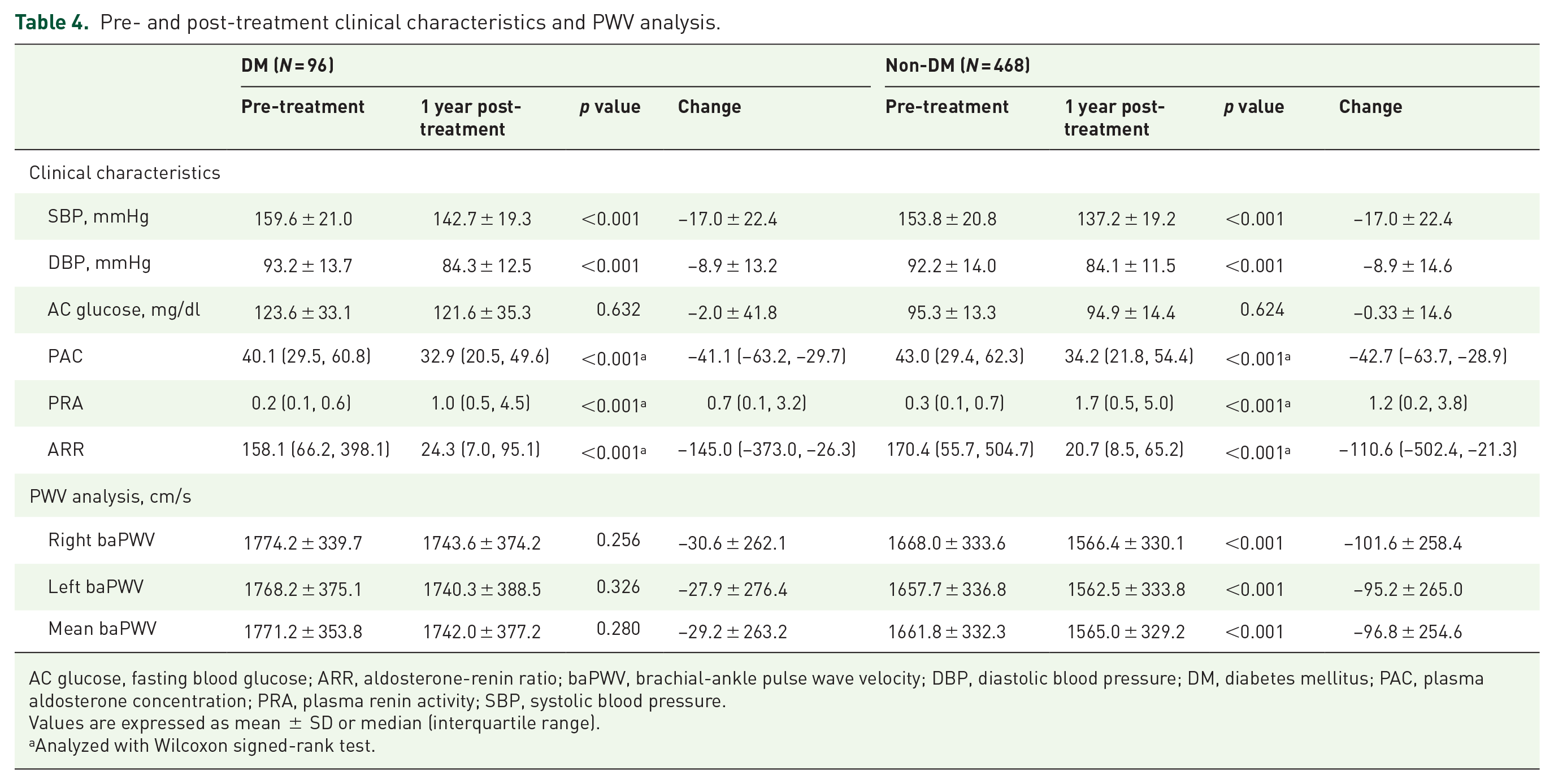
Ninety-six patients with DM and 468 patients without DM completed 1 year of PA-specific treatment. Sixty-two patients (64.6%) in the DM group and 319 (68.2%) in the non-DM group had aldosterone-producing adrenal adenoma (p = 0.495), and 81 patients (84.4%) in the DM group and 409 (87.7%) in the non-DM group received adrenalectomy (p = 0.425). SBP, DBP, PAC, PRA, and ARR significantly improved after PA-specific treatment in both the DM and non-DM groups. However, significant improvements in right, left, and mean baPWV were only noted in the non-DM group, and the improvements were not significant in the DM group.
After 1 year of treatment, the right baPWV decreased from 1774.2 ± 339.7 cm/s to 1743.6 ± 374.2 cm/s in the DM group (p = 0.256) and 1668.0 ± 333.6 cm/s to 1566.4 ± 330.1 cm/s in the non-DM group (p < 0.001); the left baPWV decreased from 1768.2 ± 375.1 cm/s to 1740.3 ± 388.5 cm/s in the DM group (p = 0.326) and 1657.7 ± 336.8 cm/s to 1562.5 ± 333.8 cm/s in the non-DM group (p < 0.001); the mean baPWV decreased from 1771.2 ± 353.8 cm/s to 1742.0 ± 377.2 cm/s in the DM group (p = 0.280) and 1661.8 ± 332.3 cm/s to 1565.0 ± 329.2 cm/s in the non-DM group (p < 0.001).
In addition, the changes in right, left, and mean baPWV were significantly higher in the non-DM group. The change in right baPWV was −30.6 ± 262.1 cm/s in the DM group and −101.6 ± 258.4 cm/s in the non-DM group (p = 0.014). The change in left baPWV was −27.9 ± 276.4 cm/s in the DM group and −95.2 ± 265.0 cm/s in the non-DM group (p = 0.025). The change in mean baPWV was −29.2 ± 263.2 cm/s in the DM group and −96.8 ± 254.6 cm/s in the non-DM group (p = 0.019). These results are shown in Table 4 and Figure 1(b).
Pre- and post-treatment clinical characteristics and PWV analysis.
AC glucose, fasting blood glucose; ARR, aldosterone-renin ratio; baPWV, brachial-ankle pulse wave velocity; DBP, diastolic blood pressure; DM, diabetes mellitus; PAC, plasma aldosterone concentration; PRA, plasma renin activity; SBP, systolic blood pressure.
Values are expressed as mean ± SD or median (interquartile range).
Analyzed with Wilcoxon signed-rank test.
Linear and nonlinear relationships between glucose levels and baPWV values
As illustrated in Figure 2(a), the relationship between baseline fasting glucose level and baseline mean baPWV value was slightly nonlinear (p for nonlinearity = 0.031). In general, baseline fasting glucose was positively correlated with baseline mean baPWV, whereas the slope was slightly steeper at a baseline fasting glucose level of approximately less than 100 mg/dl. In contrast, baseline fasting glucose was not correlated with the change in mean baPWV in either the linear or nonlinear pattern ( Figure 2(b)).

(a) Restricted cubic spline plot of the association between baseline fasting blood glucose and baseline mean baPWV. (b) Restricted cubic spline regression plot of the association between baseline fasting blood glucose and change in mean baPWV.
Discussion
There were three major findings in this study. First, the PA patients with DM were older and had higher baseline blood pressure and worse metabolic profile. Second, the PA patients with DM had worse baseline arterial stiffness compared with the non-DM PA patients. Third, the PA patients with DM had less recovery of arterial stiffness after 12 months of PA-specific treatment compared with the non-DM PA patients.
Excess aldosterone in patients with PA has been shown to have detrimental effects on many different organ systems through mineralocorticoid receptors.18,23,24 Unregulated aldosterone in PA also increases the risk of cardiovascular, renal, and cerebrovascular diseases, and several studies have also demonstrated impaired glucose metabolism.6,25–27 The prevalence of DM in patients with PA has been reported to be as high as 23%,5,25,28 which is much higher compared with the general population. 29 In the present study, the prevalence of DM was 16.5%. In addition, the body mass index and lipid profile were significantly higher in the DM patients than in those without DM. The metabolic syndrome has also been associated with cardiovascular events. 30 As DM is a major contributor to cardiovascular comorbidity, an increasing number of studies have investigated the effect of DM in patients with PA in recent years.
DM is an important global health issue and it is a major risk factor for cardiovascular disease. 31 It causes microvascular complications such as nephropathy, retinopathy and neuropathy, and also macrovascular complications such as coronary artery disease and peripheral arterial disease with an increasing duration of DM. 32 Arterial stiffness is a useful marker to detect subclinical cardiovascular disease, and it can also be used to predict clinical outcomes. 33 PWV is currently the gold standard for noninvasive measurements of arterial stiffness, and it has been linked to cardiovascular outcomes. Many methods can be used to conduct PWV analysis, including heart carotid (hc) PWV, heart femoral (hf) PWV, carotid-femoral (cf) PWV, and baPWV. While PWV can be measured in any artery or between arterial sites, carotid-femoral pulse wave velocity (cfPWV) remains the gold standard for measuring arterial stiffness. However, the use of cfPWV in clinical practice is limited by the need to expose the groin and other technical issues. 34 Consequently, baPWV is often used in Asian countries as it avoids the need to expose the groin. baPWV is associated with cardiovascular outcomes. A previous meta-analysis showed that an increase in baPWV of 100 cm/s was associated with 12%, 13%, and 6% increased risks of total cardiovascular events, cardiovascular mortality, and all-cause mortality, respectively. 35
In the current study, we found that baseline baPWV was significantly higher in the DM patients, and the results were consistent even after propensity score matching. This emphasizes that arterial stiffness was worse in the patients with PA and concurrent DM. Furthermore, previous studies have reported that age, baseline SBP, and the duration of hypertension were strongly associated with baseline PWV.21,36 In this study, the presence of DM was also an independent predictor of worse baseline PWV after multivariable linear regression analysis. Interestingly, although previous studies have demonstrated that arterial stiffness would recover after PA-specific treatment, 37 we found significantly less recovery of arterial stiffness in the DM patients after treatment. Furthermore, the glucose control in majority of DM patients in this cohort reached the target of guideline recommendations, the mean HbA1c was 6.9% and the mean fasting blood glucose was 128.3 mg/dl. 20 In addition, there was no significant change in fasting blood glucose in either the DM or non-DM group after treatment. This suggests the long-term detrimental effects of DM with aldosterone excess on arterial stiffness even after adequate blood glucose control.
In the vasculature, insulin signaling plays a crucial role in normal vascular function. The insulin signaling regulates the endothelial cell nitric oxide production and modulation of intracellular calcium homeostasis. 38 Aldosterone and mineralocorticoid receptor activation have been shown to decrease insulin receptor substrate-1 expression via reactive oxygen species and attenuate glucose uptake in vascular smooth muscle cell.38,39 The insulin resistance and hyperglycemia are possible reasons for the worse arterial stiffness and poor response to the PA-specific treatment in the DM patients. 40 Hyperglycemia can induce endothelial dysfunction, vascular smooth muscle cell proliferation, and activate fibrosis cascades.41–43 Insulin resistance can enhance collagen synthesis and induce tissue inflammation. 44 In addition, excess aldosterone also participates in arterial wall remodeling through vascular smooth muscle cell proliferation, tissue inflammation, and dysregulation of collagen metabolism. 45 These detrimental effects of aldosterone, hyperglycemia, and insulin resistance can stiffen the arterial wall and decrease vascular wall compliance. Arterial stiffness can be observed in the early stages of diabetes, and the stiffness increases if micro- and macrovascular complications are present. 46 In the current study, the RCS regression plot analysis showed that the baseline fasting blood glucose level was associated with baPWV but not the improvement in PWV after treatment which suggested the long-term effects of DM and PA on vascular remolding and arterial stiffness. The duration of DM may be a more important predictor of the improvement in arterial stiffness than DM control status. 47 Unfortunately, the duration of DM was not available in this cohort. Further studies are needed to clarify the underlying pathogenesis and mechanism of arterial stiffness induced by DM and aldosterone. This will help to identify high-risk patients and provide timely management.
Limitations
There were several limitations to this study. First, the duration of DM, which may have been a covariate of arterial stiffness, was not available in our cohort. Second, the baseline triglyceride, low-density lipoprotein, and DM medication uses were unbalanced between two groups even after propensity score matching which may be the confounders of this study. Third, the duration of hypertension may be uncertain due to recall bias. Fourth, the follow-up period was only 1 year and not all patients had the follow-up PWV analysis. Future studies with more patients having a longer follow-up period are warranted to examine the long-term effects of concurrent DM in PA on arterial stiffness. Fifth, this study did not examine the effects between surgery and mineralocorticoid receptor antagonists including spironolactone and eplerenone. Sixth, this study only investigated the effects of concurrent DM in PA on arterial stiffness. Further studies are needed to examine the long-term cardiovascular outcomes in patients with PA and concurrent DM.
Conclusion
In conclusion, the PA patients with concurrent DM in this study were associated with worse baseline and less recovery of baPWV after 1 year of PA treatment compared with those without DM. These findings indicate that the presence of DM was associated with worse arterial stiffness in patients with PA.
Footnotes
Appendix
Membership of the TAIPAI (Taiwan Primary Aldosteronism Investigation) Study Group: Che-Hsiung Wu, MD (Chi-Taz Hospital, PI of Committee); Vin-Cent Wu, MD (NTUH, PI of Committee); Yen-Hung Lin, MD (NTUH, PI of Committee); Hung-Wei Chang, MD, PhD (Far Eastern Clinics, PI of Committee); Lian-Yu Lin, MD, PhD (NTUH, PI of Committee); Fu-Chang Hu, MS, ScD (Harvard Statistics, Site Investigator); Kao-Lang Liu, MD (NTUH, PI of Committee); Shuo-Meng Wang, MD (NTUH, PI of Committee); Kuo-How Huang, MD (NTUH, PI of Committee); Yung-Ming Chen, MD (NTUH, PI of Committee); Chin-Chen Chang, MD (NTUH, PI of Committee); Shih-Cheng Liao, MD (NTUH, PI of Committee); Ruoh-Fang Yen, MD, PhD (NTUH, PI of Committee); and Kwan-Dun Wu, MD, PhD (NTUH, Director of Coordinating Center).
Acknowledgements
We thank Hsing-Fen Lin for his assistance with the statistical analysis during the completion of the manuscript and the staff of the Second Core Lab in the Department of Medical Research in National Taiwan University Hospital for technical assistance. We also thank members of the TAIPAI study group to help us completed the study (Appendix).
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Ministry of Science and Technology (MOST 107-2314-B-002-264-MY3), National Taiwan University Hospital (NTUH 107-A141, 108-A141, 109-A141, 108-N01, 108-S4382, UN108-37), and the Excellent Translational Medicine Research Projects of National Taiwan University College of Medicine, and National Taiwan University Hospital (109 C 101-43).
Conflict of interest statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
This study was approved by the Institutional Review Board of the National Taiwan University Hospital, Taiwan (NTUH REC No. 200611031R).
Informed consent
All the participants provided written informed consent prior to participation.