
Abstract
Pulmonary arterial hypertension (PAH) is a rare but fatal cardiovascular disorder with high morbidity and mortality. Diagnosis and treatment of this disease at an early stage would greatly improve outcomes. The molecular indicators of PAH are mostly nonspecific, and diagnostic and prognostic biomarkers are urgently needed. A more comprehensive understanding of the molecular mechanisms underlying this complex disease is crucial for the development of new and more effective therapeutics to improve patient outcomes. In this article, we review published literature on proteomic biomarkers and underlying molecular mechanisms in PAH and their value for disease management, aiming to deepen our understanding of the disease and, ultimately, pave the way for clinical application.
Introduction
Pulmonary arterial hypertension (PAH) is a rare but fatal cardiovascular disorder with high mortality despite therapeutic advances. PAH is characterized by a sustained increase in mean pulmonary arterial pressure (mPAP > 20 mmHg), normal pulmonary capillary wedge pressure (PCWP ≤ 15 mmHg) and increased pulmonary vascular resistance (PVR > 3 Wood units). 1 In PAH, the pulmonary vasculature is dynamically obstructed by vasoconstriction, structurally obstructed by adverse vascular remodeling, and pathologically noncompliant as a result of vascular fibrosis and stiffening. 2 According to the new classification, PAH is classified as follows: idiopathic (IPAH); heritable (HPAH); drug- and toxin-induced; associated with related factors, including connective tissue disease, HIV infection, portal hypertension, congenital heart disease (CHD) and schistosomiasis; PAH in long-term responders to calcium channel blockers; PAH with overt features of venous/capillary (PVOD/PCH) involvement; and persistent pulmonary hypertension ( PH of the newborn syndrome. 1 The incidence of PAH ranges from 2.0 to 7.6 cases per million adults per year, and its prevalence varies from 11 to 26 cases per million adults. 3 Early clinical symptoms of PAH are nonspecific and overlap with those of other cardiorespiratory diseases, leading to misdiagnosis or delayed diagnosis. The current treatment strategies for PAH are insufficient, and the prognosis is poor. There is undoubtedly an unmet need for the detection of dependable biomarkers and the development of novel therapeutic strategies.
Multiple advances have been made in the molecular analysis of the mechanisms underlying PAH. In particular, several genetic alterations have been identified, such as heterozygous germline mutations of bone morphogenetic protein receptor type-2 (BMPR2), a member of the transforming growth factor beta (TGF-β) family. 4 Mutations in this gene account for 70%–80% of HPAH cases, as well as for 15%–25% of IPAH cases; 2 multiple other genes are also related to this disease. 5 However, complex processes occur during gene expression, such as transcriptional regulation, alternative splicing and RNA editing, and proteins execute such functions. Thus, the measurement of protein levels is better for examining the clinical phenotype than raw transcriptome data. 6 Indeed, with the development of high-throughput mass spectrometry (MS) and analysis software, proteomics has become a vital complement to genomics approaches, providing valuable information about unresolved aspects of PAH.
Protein microarrays designed based on known proteins or peptides first enabled an increase in the throughput capacity to discover protein biomarkers. Then, gel-based and MS-based techniques, including two-dimensional gel electrophoresis (2-DE) and two-dimensional difference gel electrophoresis (2D-DIGE), were implemented as high-throughput technologies for proteomics. 7 However, the main problems with these methods are their poor reproducibility, small protein load capacity, and inability to detect proteins with low abundance and strong hydrophobicity. 8 The most commonly utilized method for analyzing proteins by MS is a bottom-up approach to identify and quantify enzymatically digested peptides. The two traditional methods for protein identification by MS are matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) and liquid chromatography (LC) with electrospray ionization (ESI). Nano ESI coupled with nano high-performance LC (nHPLC) has become the standard LC-MS approach in the majority of proteomics labs. 9 In addition, surface-enhanced laser desorption/ionization (SELDI), another strategy for the MS analysis of macromolecules, has been introduced, simplifying sample extraction and facilitating effective on-probe investigations of biopolymers when compared to conventional MALDI approaches. 10 Quantitative proteomics can be separated into shotgun proteomics and targeted proteomics approaches. The former can be performed based on mass tags, including isobaric tags for relative and absolute quantification labels (iTRAQ), tandem mass tag (TMT), and stable isotope labeling using amino acids in cell culture (SILAC) or by calculating the spectral count, which is a label-free quantitative approach. 11 Labeling combined with tandem mass spectrometry (MS/MS) strategies allow the quantification and identification of many different pooled samples in one experiment, with high sensitivity and reproducibility. 9 Moreover, label-free quantification overcomes the limitation of sampling conditions in label-based methods and has the capacity to evaluate large samples, although demands for data and information analysis are high. The methods mentioned above are frequently used, and new proteomic technologies are still evolving.
A wide variety of clinical specimens, including blood (plasma/serum), heart/lung tissues (fresh frozen and formalin-fixed paraffin-embedded tissue blocks) and different cell types from patients or murine models, such as monocrotaline (MCT)- and pulmonary artery binding (PAB)-induced PAH rats, are commonly used in PAH proteomic studies. Conversely, other body fluids, such as urine and bronchoalveolar lavage fluid, have not been used in PAH studies to date. The classical workflow for PAH proteomics studies using various biospecimens is shown in Figure 1. In this review, we summarize the current proteomic studies and outline those that are proposed to be valuable in the field of PAH. The main findings were summarized in Figure 2.
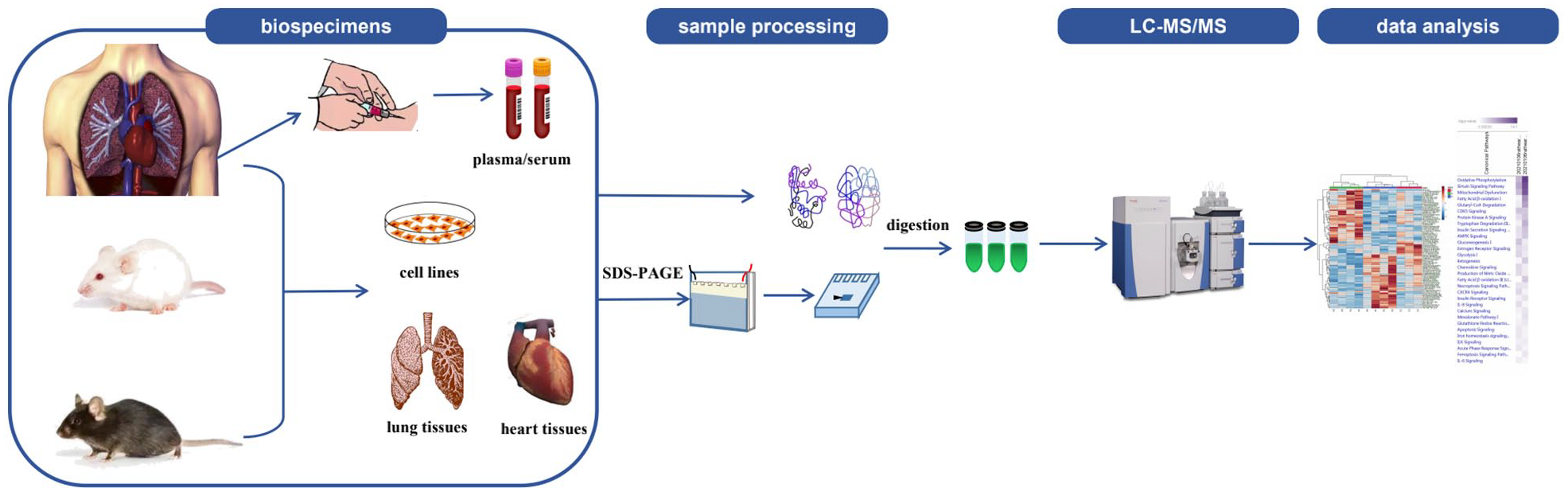
An overview of proteomics workflow and commonly used biospecimens for studying PAH. Commonly used biospecimens in proteomic studies of PAH include blood (plasma/serum), heart/lung tissues and different cell types from patients and murine models. Samples are extracted via gel-based or gel-free approaches and then digested enzymatically. Peptides are then fractionated using liquid chromatography (LC) and then subjected to mass spectrometry (MS). Proteins are identified in databases, and functional analyses are performed using bioinformatic methods.

The main findings from proteomic analysis of PAH.
Proteomic studies to identify PAH biomarkers for potential clinical use
Although the list of biomarkers is constantly growing,12–14 and includes TNF-like weak inducer of apoptosis (TWEAK), pro-atrial natriuretic peptide (proANP), growth differentiation factor-15 (GDF-15), soluble fms-like tyrosine kinase 1, placental growth factor, and galectin-3, guidelines recommend only a small number of them, such as brain natriuretic peptide (BNP), N-terminal proBNP (NT-proBNP), and cardiac troponin (cTn). Two major biomarkers of PAH were recently proposed in the 2019 European Respiratory Society (ERS) International Congress. 15 One study reported that the levels of endostatin (ES), a potent angiostatic factor, are elevated in PAH patients and distinguishes them from healthy controls (HCs) at a serum threshold of 66 ng/ml, with an area under the receiver operator characteristic (ROC) curve (AUC) of 0.879. 16 The ES level in PAH patients was found to correlate positively with the mPAP, right atrial pressure (RAP), 6-min walking distance (6MWD), and cardiac output (CO).16,17 ES could also identify nonsurvivors, with an AUC of 0.675 (p = 0.02), and higher expression was related to a significantly increased risk of death (unadjusted hazard ratio = 4.2, 95% CI = 1.3–14.6), with a median follow-up of 3.4 years. 16 All of the above findings indicate that ES can serve as a diagnostic and predictive biomarker of disease severity and poor survival in PAH. Another promising biomarker is asymmetric dimethylarginine (ADMA), the major endogenous nitric oxide synthase (NOS) inhibitor, which has been shown to be relevant to follow-up BNP and risk assessment scores in PAH patients who improved after targeted therapy. 15 A comprehensive list of proteomic studies focusing on blood biomarkers and the key findings are presented in Table 1.
A comprehensive list of proteomic studies focusing on blood biomarkers of PAH.

ADIPO, adiponectin; ADMA, asymmetric dimethylarginin; ANPEP, alanyl membrane aminopeptidase; ApoE, apolipoproteins E; AUC, area under the ROC curve; DBH, dopamine β-hydroxylase; 2-DE, two-dimensional gel electrophoresis; Epo, erythropoietin; ELISA, enzyme-linked immunosorbent assay; FSTL3, Follistatin-like 3; GNAS, guanine nucleotide-binding protein Gs; GP1BA, glycoprotein Ib platelet-subunit; HC, healthy control; HPAH, heritable pulmonary arterial hypertension; IGFBP1, insulin-like growth factor binding protein-1; IL-1R1, interleukin-1 receptor-like 1; IPAH, idiopathic pulmonary arterial hypertension; iTRAQ, isobaric tags for relative and absolute quantification labels; LC-MS, liquid chromatography-mass spectrometry; LRG, leucine-rich a-2-glycoprotein; MALDI-TOF, matrix-assisted laser desorption/ionization-time of flight; MDK, Midkine; MS, mass spectrometry; 6MWD, 6-minute walking distance; NYHA, New York Heart Association; SSc, systemic sclerosis; TIMP, tissue inhibitors of metalloproteinases; TRF1, transferrin receptor 1; UHPLC, ultra-high-performance liquid chromatography; VSD, ventricular septal defect; PAH, Pulmonary arterial hypertension; WHO, World Health Organization.
Diagnostic biomarkers for PAH
Currently, the diagnosis of PAH is mainly based on symptoms, physical examination and several procedures, including right heart catheterization (RHC). 26 Several molecular biomarkers, such as pentraxin 3 (PTX3), caveolin-1 (Cav1), selenoprotein P and interleukin (IL)-32, have potential diagnostic value, but large-scale verification is lacking.27–30 Proteomic research can identify whole protein profiles and constitutes a potent method for novel biomarker discovery. Abdul-Salam et al. 18 first screened the differentially expressed proteins (DEPs) in the plasma of 27 IPAH patients using SELDI-TOF MS and identified complement 4a (C4a) des Arg as a potential diagnostic biomarker. The ability of this marker to identify 92% of IPAH patients and 80% of HCs was validated, with a cutoff value of 0.6 µg/ml. Using gel-based proteomic analysis, Yu et al. 19 reported protein changes in the serum of 20 IPAH patients. Thirteen proteins were altered compared with those in HCs, of which two candidates, that is, alpha-1-antitrypsin and vitronectin, were significantly downregulated and may serve as valuable biomarkers that are worthy of further exploration. In addition, Rice et al. 20 used SOMAscan to identify 82 proteins as being differentially regulated in the serum of 13 treatment-naive systemic sclerosis-associated PAH (SSc-PAH) patients compared to SSc-non-PAH patients. The levels of growth factor-midkine (MDK) and TGF-β-regulated protein-follistatin-like 3 (FSTL3) were elevated, and their discrimination capacity for SSc-PAH was evaluated in three independent cohorts. The combination of MDK and FSTL3 had AUCs of 0.94, 0.85, and 0.92, indicating the potential as a diagnostic biomarker of PAH in SSc patients.
Prognostic/predictive biomarkers for PAH
Several recent registries have identified some effective predictors of survival outcomes, such as age, sex and factors reflective of right heart function. 31 Most prognostic markers recommended by the European Society of Cardiology (ESC) and ERS guidelines are related to right ventricular function and CO, including various indices of exercise tolerance, mean RAP, and cardiac index (CI). 26 At present, the most popular tools for PAH risk stratification and prognostication are the risk scores published by the US Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL), the 2015 ESC/ERS PH guidelines risk table and a multiparametric risk stratification approach raised in the sixth World Symposium on Pulmonary Hypertension (WSPH), in which BNP or NT-proBNP is the only laboratory biomarker, which is absolutely not specific in PAH.32–34 More recently, investigators have derived additional risk assessment strategies, but molecular biomarkers are still lacking.32,35–37
Using LC-MS/MS, Sandqvist et al. 21 identified significant upregulation of ADMA and symmetric dimethylarginine (SDMA) levels in the plasma of 21 PAH patients compared to 14 patients with left ventricular systolic dysfunction (LVSD) patients and 27 HCs. According to the results, L-arginine levels and the L-arginine/ADMA ratio were significantly lower in PAH patients than in HCs and were correlated with 6MWD (r = 0.58, p = 0.006) and the World Health Organization (WHO) functional class (r = −0.46, p = 0.043), respectively, in PAH patients. Zhang et al. 22 revealed higher levels of leucine-rich a-2-glycoprotein (LRG) in the serum of IPAH patients compared with HCs through 2-DE and MALDI-TOF MS analysis, and the results were validated by ELISA. Furthermore, the serum concentration of LRG, which modulates the activity of TGF-β, was correlated positively with the New York Heart Association (NYHA) functional class (r = 0.71, p < 0.01) but inversely correlated with the right-sided CO (r = −0.65, p < 0.01), indicating that it may be a specific prognostic biomarker of IPAH.
There is a growing consensus that the sensitivity and specificity of biomarker panels, multiple markers used in combination, are increased compared to those of proteins utilized individually. 9 Yuan et al. 23 found that increased plasma protein levels of dopamine β-hydroxylase (DBH), adiponectin (ADIPO), and alanyl membrane aminopeptidase (ANPEP) were independently associated with the occurrence of PAH in 120 patients with ventricular septal defect (VSD) patients. A new total risk score was developed based on these three proteins as a predictor of the development of PAH in VSD patients, with a large AUC of 0.87 (95% CI = 0.78–0.96, p < 0.0001). A multicenter observational cohort study used aptamer-based technology to probe the plasma proteome of HPAH and IPAH patients and identified a panel of nine proteins, IL-1 receptor-like 1 (IL1R1/ST2), tissue inhibitors of metalloproteinases (TIMP-1 and TIMP-2), plasminogen, apolipoproteins E (ApoE), erythropoietin (EPO), complement factor H and factor D, and insulin-like growth factor binding protein-1 (IGFBP-1), that acted as prognostic factors independent of the plasma NT-proBNP concentration and were confirmed by targeted assays. A cutoff-based score using this panel predicted the prognosis of all-cause mortality independent of the REVEAL equation, raising the C statistic AUC from 0.83 to 0.91 (p < 0.0001). 24
In addition, complex changes in cytokines, cellular immunity and autoantibodies suggest that PAH is, in part, an autoimmune, inflammatory disease. 2 A multiplex immunoassay performed by Sweatt et al. 25 measured a circulating proteomic panel of 48 cytokines and chemokines in the plasma of PAH patients, classifying them into four proteomic immune clusters independent of clinical features. These immune clusters had different central cytokine signatures, clinical risk profiles and long-term outcomes. For instance, cluster 1 (TNF-related apoptosis inducing ligand (TRAIL), CCL5, CCL7, CCL4, macrophage migration inhibitory factor (MIF), and TNF-β) comprised the highest risk group with more functional class IV symptoms, higher NT-proBNP concentrations, and higher REVEAL scores and more impaired echocardiographic right ventricular function. Correspondingly, the event rate was highest (50.0%, n = 29/58, 7 transplantations and 22 deaths) and the 5-year transplant-free survival rate was lowest (47.6%, across cluster p < 0.001) in cluster 1 patients, suggesting that blood cytokine profiles distinguishing PAH immune phenotypes are potential prognostic features of PAH.
Nevertheless, blood samples do have some limitations. The presence of a few highly abundant proteins, such as albumin and immunoglobulin, can mask proteins of lower abundance that may be biologically important; ready-made albumin and IgG removal kits are available. Another limitation of serum samples is that a small series of protein changes might occur after plasma is allowed to clot, which may prevent the detection of some disease-related proteins. 19 However, the establishment of blood biomarkers that can be noninvasive is still an ideal choice for PAH patients. In addition, serum/plasma can be a true indicator of disease progression and can help in longitudinal studies monitoring minute changes in the proteome. 38
Proteomics studies to uncover the mechanisms underlying PAH
Progress has been made in understanding the pathophysiological mechanisms of PAH and approving drug therapies. For example, a cancer-like increase in cell proliferation and resistance to apoptosis reflects acquired abnormalities of mitochondrial metabolism and dynamics. Epigenetic dysregulation of DNA methylation, histone acetylation, and microRNAs also contributes to disease pathogenesis. 2 In addition to identifying protein biomarkers, proteomics has been useful for uncovering the mechanism of PAH, especially with the development of bioinformatic technology and analysis software. Comprehensive lists of proteomic studies focusing on PAH occurrence and progression and on PAH-related gene mutations as well as their main findings are presented in Tables 2 and 3, respectively.
A comprehensive list of proteomic studies focusing on PAH occurrence and progression.

ATP5F1A, ATP synthase subunit alpha; C3, complement 3; CFHR2, complement factor H-related protein 2; CHCHD3, MICOS complex subunit; CHD, congenital heart disease; CLIC4, chloride intracellular channel 4; CPS1, carbamoyl-phosphate synthetase I; 2D-DIGE, two-dimensional fluorescence difference gel electrophoresis; 2-DE, two-dimensional gel electrophoresis; DEPs, differentially expressed proteins; EIF5B, eukaryotic translation initiation factor 5B; FABP4, fatty acid binding protein-4; HADHA, trifunctional enzyme subunit alpha; HADHB, trifunctional enzyme subunit beta; HC, healthy control; HPLC-ESI, high-performance liquid chromatography-electrospray ionization; HSP-27, heat shock protein-27; IMMT, MICOS complex subunit MIC60; IPAH, idiopathic pulmonary arterial hypertension; iTRAQ, isobaric tags for relative and absolute quantification labels; LC-MS, liquid chromatography-mass spectrometry; MALDI-TOF, matrix-assisted laser desorption/ionization-time of flight; MCT, monocrotaline; MRPL34, mitochondrial ribosomal protein L34; MS, mass spectrometry; NDUFS1, NADH-ubiquinone oxidoreductase 75 kDa subunit; PAB, pulmonary arterial banding; PABPN1, polyadenylate-binding nuclear protein 1; PAEC, pulmonary artery endothelial cell; PAH, pulmonary arterial hypertension; PDE5A, phosphodiesterase type 5 A; PH, pulmonary hypertension; PKA, protein kinase; RV, right ventricle; SLC25A3, phosphate carrier protein; SUCLG2, succinate-CoA ligase subunit beta; SuHx, Sugen5416 with hypoxia; TGOLN2, trans-Golgi network integral membrane protein 2; TMT, tandem mass tag; UQCRC2, Cytochrome b-c1 complex subunit 2; ZC3 H4, zinc finger CCCH domain-containing protein 4.
A comprehensive list of proteomic studies focusing on PAH-related gene mutations.
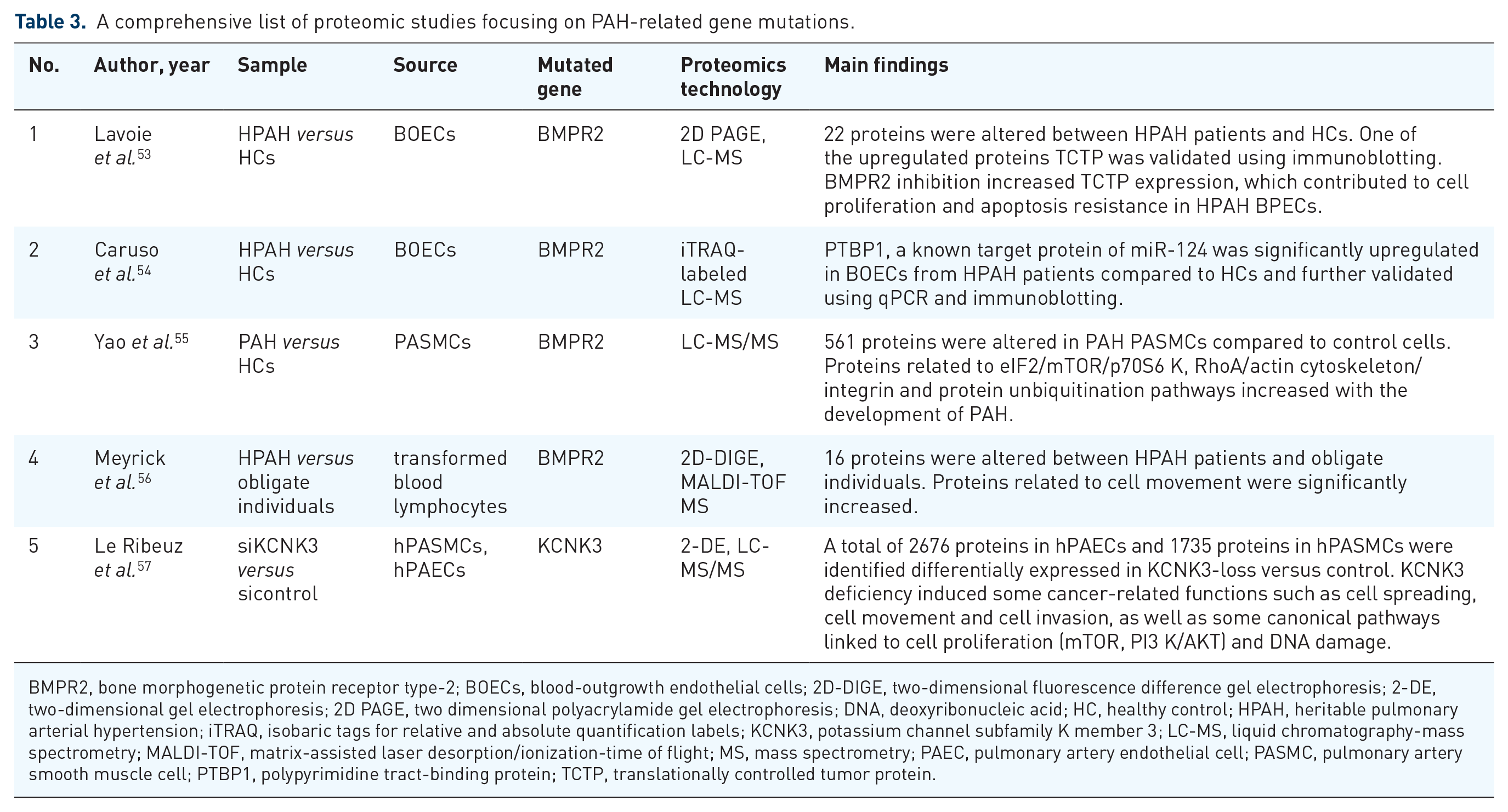
BMPR2, bone morphogenetic protein receptor type-2; BOECs, blood-outgrowth endothelial cells; 2D-DIGE, two-dimensional fluorescence difference gel electrophoresis; 2-DE, two-dimensional gel electrophoresis; 2D PAGE, two dimensional polyacrylamide gel electrophoresis; DNA, deoxyribonucleic acid; HC, healthy control; HPAH, heritable pulmonary arterial hypertension; iTRAQ, isobaric tags for relative and absolute quantification labels; KCNK3, potassium channel subfamily K member 3; LC-MS, liquid chromatography-mass spectrometry; MALDI-TOF, matrix-assisted laser desorption/ionization-time of flight; MS, mass spectrometry; PAEC, pulmonary artery endothelial cell; PASMC, pulmonary artery smooth muscle cell; PTBP1, polypyrimidine tract-binding protein; TCTP, translationally controlled tumor protein.
Disease occurrence and progression
Using a gel-based approach, Régent et al. 39 identified 336 DEPs between normal human vascular smooth muscle cells (VSMCs) from the pulmonary artery and VSMCs from PAH patients (PAH-SMCs). The PAH-SMCs displayed a more synthetic phenotype, as the expression of smooth muscle myosin heavy chain was decreased and the proliferation rate increased. Xu et al. 40 found four proteins to be differentially expressed at both the protein and phosphopeptide levels in pulmonary artery endothelial cells (PAECs) in the lungs of PAH patients compared to HCs: eukaryotic translation initiation factor 5B (EIF5B), trans-Golgi network integral membrane protein 2 (TGOLN2), polyadenylate-binding nuclear protein 1 (PABPN1), and zinc finger CCCH domain-containing protein 4 (ZC3 H4). Further integrative network analysis of multiomics data in PAECs and plasma uncovered dysregulated pathways that are primarily related to mitochondria. Faber et al. 41 employed the MALDI-TOF MS approach and found that the majority of cytoplasmic protein changes in a PAB-induced PAH rat model were related to metabolism, indicating a shift toward the glycolytic pathway at the expense of β-oxidation in the compensated right ventricle (RV). James et al. 42 reported that antimycin A (AA)-induced inhibition of mitochondrial complex III also lead to sustained pulmonary vasoconstriction and a glycolytic shift. These authors further investigated quantitative mitochondrial proteomics in the lungs of AA-induced PH rats, detecting significant changes in 28 proteins with severe impairment in fatty acid pathways, the TCA cycle, the electron transport chain and amino acid metabolism. Using TMT-labeled quantitative proteomics analysis of MCT-induced rat models, Prisco et al. 43 demonstrated that increased glucose flux through the hexosamine biosynthetic pathway (HBP) adversely affected the RV by promoting excess O-GlcNAcylation of mitochondrial proteins. Using an iTRAQ-based LC-MS approach, Hołda et al. 44 investigated the RV myocardial proteomic profile of rats with MCT-induced PAH at different stages. Proteins associated with the fatty acid β-oxidation pathway and myosin-7 were upregulated during early PAH; during end-stage PAH, proteins related to myocardial structural components, intensified fibrosis and glycolytic processes were increased, and those related to the cardiomyocyte Ca2+ current were decreased. Changes in RV proteins associated with apoptosis inhibition were observed in both stages. Shields and colleagues used heart adipose samples from Sprague-Dawley (SD) rats with significant PAH to perform adipose proteomics analysis with 2-D DIGE in combination with MALDI-TOF MS. They selected 21 significantly different protein spots and identified 2 interesting proteins suggested to be involved in the innate immune system (complement C3) and adipose dysfunction (fatty acid binding protein-4, FABP4), which implicated small visceral adipose dysfunction related to inflammation in the pathophysiology of this experimental animal model of PAH. 45 Impaired mitochondrial and metabolic functions found in the lungs and RV are also present in the skeletal muscles of PAH patients. 46 Considering the possible involvement of peripheral oxidative metabolism dysfunction, Malenfant et al. 46 documented 9 downregulated proteins in the skeletal muscle and 10 upregulated proteins in 8 IPAH patients compared to the HCs. The IPAH patients exhibited decreased expression levels of oxidative enzymes and more glycolytic metabolism in skeletal muscles, with abnormal mitochondrial morphology and function.
By examining surgically acquired lung samples from IPAH/HPAH patients undergoing lung transplantation (n = 8) and control subjects using label-free LC-MS/MS, Abdul-Salam and colleagues observed increased expression of chloride intracellular channel 4 (CLIC4), which was found to be essential for the inordinate angiogenesis of plexiform lesions and was confirmed by western blotting and immunohistochemistry. 47 Further proteomic analysis of CLIC4-interacting proteins in human PAECs identified ADP ribosylation factor 6 (Arf6) as an apparent mediator of CLIC4 in the downstream nuclear factor-kappa B (NF-ĸB), hypoxia-inducible factor (HIF) and angiogenic response signaling pathways in PAH. 48 Hemnes et al. 49 performed an aptamer-based proteomic assay and detected 11 plasma DEPs in PAH patients compared with HCs that were involved in insulin signaling, lipid signaling and transport. Using iTRAQ-labeled quantitative LC-MS/MS analysis, Zhang et al. 50 revealed significant alterations in 10 plasma proteins when comparing 266 CHD patients with or without PAH. Among them, carbamoyl-phosphate synthetase I (CPS1), which is related to endogenous NO production, and complement factor H-related protein 2 (CFHR2), which is related to the complement system and coagulant mechanism, were found to play important roles and were further validated by ELISA.
In addition to the commonly used samples, samples such as platelets and exosomes have received recent attention in the proteomic field. As platelets from IPAH patients exhibited typical metabolic shifts and activation defects, Aulak et al. 51 performed proteomics analyses of platelets from IPAH patients and HCs, showing dysregulated vasoactive signals. Further mechanistic examinations revealed that decreased expression of the G protein αs and increased expression of cAMP-dependent protein kinase type II isoforms led to inactivation of the prostacyclin pathway; reduced soluble guanylate cyclase (sGC) subunits and incremental phosphodiesterase type 5 A impacted NO responsiveness. 51 Exosomes have been found to modulate PAH based on miRNAs and may be a novel therapy. 58 Hogan et al. 52 performed proteomic analysis of mesenchymal stromal cell-derived exosomes using LC-MS/MS, indicating that exosomes were enriched for several metabolic proteins involved in glycolysis, the TCA cycle and the electron transport chain. This finding provides clues for further research on abnormal mitochondrial metabolism in PAH and the therapeutic effect of exosomes.
Pathogenic alterations underlying PAH-related gene mutations
BMPR2 was the first mutated gene to be associated with PAH, although the mechanism by which it acts was not entirely clear. One of the notably upregulated proteins in the blood-outgrowth endothelial cells (BOECs) of HPAH patients with BMPR2 mutations was identified by proteomic analysis as translationally controlled tumor protein (TCTP), a protein promoting tumor cell growth and survival; TCTP was further validated in the Sugen5416 injection combined with hypoxia (SU5416) rat model of severe PAH. This result indicated that increased TCTP expression was associated with intimal lesions and proliferating ECs and may be an important mediator of vessel remodeling. 53 Using an iTRAQ-labeled proteomic approach, Caruso et al. 54 identified polypyrimidine tract-binding protein (PTBP1) as one of the most upregulated proteins in BOECs from HPAH caused by BMPR2 mutation compared with control cells. Combined with metabolic profiles and unbiased genome-wide screening, they discovered an altered miR-124/PTBP1 axis and increased expression of pyruvate kinase muscle isoforms 2 (PKM2) in PAH BOECs, leading to a hyperproliferative and hyperglycolytic phenotype of PAH. In addition, Yao et al. 55 performed a comparative analysis of protein expression in response to endothelin-1 in pulmonary artery smooth muscle cells (PASMCs) from PAH subjects with BMPR2 mutations and HCs using label-free MS quantitation. The results identified eukaryotic initiation factor 2/mammalian target of rapamycin/p70 ribosomal protein 6 kinase (eIF2/mTOR/p70S6 K), RhoA/actin cytoskeleton/integrin and protein ubiquitination as the canonical pathways involved in the development of PAH, and these pathways are intimately related to the PAH-related physiology of smooth muscle proliferation, apoptosis, contraction and cellular stress. Although BMPR2 mutation is autosomal dominant, only an estimated 20% of carriers develop clinical PAH. 59 Using MALDI-TOF MS, 16 proteins associated with cell movement, binding, signal transduction, and catabolism showed altered expression in transformed blood lymphocytes from HPAH patients compared with obligate individuals from one family with a known BMPR2 mutation. Among them, the levels of growth factor receptor-bound protein 2 (Grb2) protein, an adapter protein linked to binding, signal transduction and activation of several growth factor receptors, were reduced. In contrast, the level of PSD-95/disks large/ZO-1 (PDZ) and LIM domain protein 1 (PDLIM1), which is associated with the actin cytoskeleton, was increased, and that of β-actin and lymphocyte-specific protein 1, an intracellular F-actin binding protein, was decreased. These differences highlight the potential role of actin dynamics in the progression of BMPR2-mutated PAH. 56
Using an LC-MS/MS-based proteomics approach, Le Ribeuz et al. 57 identified 326 and 222 DEPs in hPAECs and hPASMCs with loss of potassium channel subfamily K member 3 (KCNK3) expression, which is a commonly recognized genetic cause of PAH. Among the altered proteins with the highest fold changes, increased heme oxygenase 1 (HMOX1) expression and decreased interferon-induced proteins with tetratricopeptide repeats 3 (IFIT3) expression were highlighted and validated by western blotting. Further functional analysis suggested that KCNK3 deficiency induces some cancer-related functions, such as cell spreading, movement, and invasion, as well as some canonical pathways linked to cell proliferation, such as mTOR, phosphatidylinositol 3 kinase/protein kinase B (PI3 K/AKT), and DNA damage.
Response to treatment
PAH is characterized by elevated PAP and is managed by vasodilator therapies. Despite great advances in the treatment of PAH, it is still a devastating disease with high mortality. Novel targets and identification of suitable candidates for PAH therapy are urgently needed. Nogueira-Ferreira et al. 60 discovered that MCT-injected rats treated with terameprocol (TMP), a cellular proliferation inhibitor and apoptosis promoter, showed reduced pulmonary and cardiac remodeling and improved cardiac function. Then, using an iTRAQ-based proteomic approach, they found decreased levels of the transcription factor high mobility group protein B1 (HMGB1) in PASMCs from the MCT rats, as well as DNA transcription- and TGF-β-related pathways, which partly explained the potential therapeutic role of TMP in PAH. Using gel-based MS analysis, Yeager et al. 61 sought to uncover the molecular differences between IPAH patients with good and poor responses to long-term vasodilator therapy. The results showed that children with a good response had less serum amyloid A4 (SAA-4) in their plasma than those with a poor response and lower serum amyloid P (SAP) levels prior to therapy. As SAP and SAA-4 regulate circulating mononuclear phagocytes, they may be conducive to the differential response with regard to inflammation in IPAH. Omics studies to characterize the likelihood of a patient responding to a given drug were mainly about gene variants and expression patterns; proteomic studies for precision medicine are still scarce and need further exploration.62–64
Huang et al. 65 used iTRAQ-labeled MS to identify DEPs in tissues from the lung biopsies of CHD patients with reversible and irreversible PAH evaluated by RHC after repair surgery. Most of these DEPs are cytoskeletal and collagen proteins that are mainly associated with cell adhesion, cytoskeleton organization and the extracellular matrix. Upregulation of Cav1, filamin A, and cathepsin D combined with increased macrophagocytes and downregulation of glutathione S-transferase mu 1 (GSTM1) are potential biomarkers for evaluating the operability of CHD-PAH. In another article published by the same team, transgelin was reported to be significantly upregulated in the lung tissues of patients with irreversible CHD-PAH, contributing to PSMC proliferation, migration and apoptosis resistance. 66 Proteomics represent a valid approach to improve our comprehension of molecular mechanisms leading to PAH, which could facilitate the distinction of treatment responders versus nonresponders in the future.
Different alterations between RV and LV
In most cases, the study of PAH is limited to the right heart and pulmonary circulation system. Studies focused on different alterations between the left ventricle (LV) and RV have also been conducted. It is well established that MCT has toxic effects, which can be directly observed in the myocardium; thus, proteomic analysis might be biased by this fact. In the MCT model, both ventricles are affected by enhanced neuroendocrine stimulation, but only the RV exhibits excessive pressure load. 67 Schott et al. 67 analyzed RV and LV proteomes in this model by gel-based MALDI-TOF MS. Proteomic changes, including those of myofilament regulatory proteins, energy metabolism-related proteins, and cell cycle regulating proteins, which were restricted to the RV, may simply be caused by pressure overload. Alteration of BRCA1-associated protein 2 (BRAP2) inhibited the translocation of breast cancer susceptibility gene-1 (BRCA1), a tumor suppressor gene, and repressed its antiproliferative role in PAH, which allowed specific focus to be applied to the molecular mechanisms of RV over the course of PAH. Using iTRAQ-labeled MALDI-TOF/TOF, Friehs et al. 68 compared the proteomic profiles of pressure-overloaded LVs and RVs of newborn New Zealand white rabbits by aortic banding (AOB) and PAB, respectively. The expression levels of proteins involved in cellular macromolecular complex assembly and protein kinase-A signaling in LV-AOB were increased, while those associated with the structural constituents of muscle and calcium handling in RV-PAB were increased. These different alterations provide new insight into the divergent physiological response to pressure overload and into the biological basis of ventricular-specific treatment.
Proteomic studies to characterize deep phenotypes of PAH
Except for HPAH, PAH subtypes are mainly classified by clinical features, which are not relevant to molecular biology pathogenesis. Although they all belong to PAH based on the WSPH classification, different subtypes of PAH have both common and specific mechanisms. According to the abovementioned proteomic studies, we summarized the differences and similarities of the altered proteins and pathways among IPAH, HPAH, CHD-PAH, and SSc-PAH (Supplementary Table 1). Funded by the National Heart, Lung, and Blood Institute (NHLBI), the pulmonary vascular disease phenomics program (PVDOMICS, NCT02980887) aims to perform reclassification and deep phenotyping of PH based on molecular and cellular information using multiomics approaches (genomics, transcriptomics, proteomics, metabolomics, coagulomics, cell biomics), which could assist with personalized diagnoses, prevention and treatment in the long term. In the future, we expect more innovative findings from currently undergoing programs in this area will be published in article form.
Conclusion
To conclude, several studies have examined the proteome of PAH and successfully discovered potential biomarkers for disease occurrence, diagnosis, prognosis and response to treatment. Most of these biomarkers are related to previously accepted mechanisms but provide details about more concrete molecular changes, such as energy metabolism, endothelial function, regulation of cell growth, inflammation and the immune system. Moreover, some newly proposed biomarkers provide further insight into the disease. Although many candidate protein markers and latent mechanisms have been reported, few have been deeply investigated and implemented in the clinic. Whether the proteins and mechanistic pathways acquired from proteomic studies aid clinical decisions needs more validation in prospective clinical cohorts and deeper mechanistic mining grounded in basic research. Integration of multiomics approaches is imperative for the elucidation of molecular alteration at multiple levels and for providing more targeted directions for further in-depth research. We should pay continuous attention to the innovative outcomes from the large-scale project, such as the PVDOMICS, the U.K. PAH Cohort Study Consortium, and the U.S. PAH Biobank Consortium. While progress has been made regarding elucidation of the underlying mechanisms and approval of drug therapies, proteomics, and posttranslational modifications (PTMs) will continue to broaden our understanding of PAH pathogenesis and promote the development of proteomics-driven precision medicine (PDPM) for PAH. Ultimately, integrating the data from all platforms will deepen our understanding of the disease and pave the way for better outcomes for patients with PAH.
Supplemental Material
sj-docx-1-taj-10.1177_20406223211047304 – Supplemental material for Proteomic analysis of pulmonary arterial hypertension
Supplemental material, sj-docx-1-taj-10.1177_20406223211047304 for Proteomic analysis of pulmonary arterial hypertension by Xiaohan Qin, Tianhao Li, Wei Sun, Xiaoxiao Guo and Quan Fang in Therapeutic Advances in Chronic Disease
Footnotes
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (grant number 2018-I2M-1-001), the National Natural Science Foundation of China (grant number 81500306), and Xinxin-Merck Cardiovascular Research Fund (grant number 2017-CCA-xinxin merck fund-005).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.