
Abstract
Aims:
This study aimed to explore the effects of vertebral rotation on the position of the aorta relative to the thracolumbar and lumbar spine, and to identify risk factors for vertebral rotation in patients with adult degenerative scoliosis (ADS).
Methods:
A total of 71 patients with ADS were divided into left scoliosis (LS) group (n = 40 cases) and right scoliosis (RS) group (n = 31cases) with well-matched demographics. Apical vertebrae, Cobb angle (°), coronal horizontal movement, thoracolumbar kyphosis (TLK) and Nash–Moe rotation classification were measured on X-ray. The Cartesian coordinate system was established on T2-MRI for each level of intervertebral disc on thracolumbar and lumbar spine, where aorta–vertebrae angle (α), aorta–vertebrae distance (d), and vertebral rotation angle (γ) for each level of T12-L1 to L3-L4 on MRI were defined within the Cartesian coordinate system.
Results:
There was no statistical difference in the distribution of apical vertebrae between LS and RS groups. Nash–Moe classification was of no significance between the two groups. When there was a larger Cobb angle and coronal horizontal movement, a greater γ in LS group and a lower γ in RS group were noted (both p < 0.001). There was no correlation among γ, α, and d in LS group (p = 0.908 and 0.661, respectively) nor in RS group (p = 0.738 and 0.289, respectively). In LS group, Nash–Moe classification correlated to Cobb angle, coronal movement and TLK. In RS group, it correlated to Cobb angle and coronal movement. Cobb angle was the risk factor for Nash–Moe classification in RS group while no factors were identified in LS group. Coronal movement was independent risk factor for γ (p = 0.003) in LS group. Moreover, γ was affected by Cobb angle (p = 0.001) and coronal horizontal movement (p = 0.006) in RS group.
Conclusion:
Vertebral rotation could be predicted by Cobb angle or coronal horizontal movement measured on X-ray in ADS patients and aorta maintained in a relatively normal position in patients with ADS.
Keywords
Introduction
Adult degenerative scoliosis (ADS), in high prevalence, is a potentially debilitating spine condition caused by progressive degenerative changes with multiaxial rotational deformity. It can result in severe pain and functional impairment, and often warrants surgical intervention since conservative measures have not be proven effective in the majority of ADS cases.1,2 It frequently develops in a skeletal mature spine deriving from the degenerative change on facets or disc without preexisting spinal deformity. 3 The progressive degeneration mainly occurs in the distal levels of the spine, resulting in load-sharing changes involving the entire spine, and ensuing loss of lumbar lordosis and sagittal plane deformity. The pathological findings include disc collapse, facet hypertrophy, capsule degeneration, and ligamentous hypertrophy, which influence the load distribution of both the anterior and the posterior columns, ultimately leading to degenerative scoliosis. There have been two factors reported in association with the severity of the ADS: magnitude of the curvature and vertebral rotation.4–6
The vertebral rotation plays a pivotal role in the development of ADS with typical characteristic. Hong et al. 2 carried out a prospective cross-sectional study on 1347 adult volunteers, and found an identified relationship between ADS and lateral olisthisis, vertebral rotation, lumbar hypolordosis, sagittal imbalance, and a high level of the L4-5 disc. Trammell et al. 6 identified the presence of rotatory olisthisis and its association with a number of parameters, such as age, gender, type of curve, magnitude of curvature, level of occurrence, and severity of slip and pain. Rotatory olisthisis was noted statistically irrelevant to the occurrence of back pain associated with adolescent idiopathic scoliosis (AIS) and more likely to be associated with radicular pain in lumbar degenerative curves. For ADS patients, pedicle screw fixation is challenging in thoracic spine since inadvertently misplaced screws may initiate a high risk of complications. Also, patients are typically of advanced age and with atherosclerosis with reduced vascular elasticity. However, to date, studies have seldom assessed the relationship between vertebral rotation and the abdominal aorta. Hence, it is of great significance to address the effects of vertebral rotation in the position of the aorta relative to the spine in patients with ADS.
Previous studies have described the influence of vertebral rotation on the pedicle screw placement, and concentrated on patients with AIS and other spinal deformities,7,8 but not on ADS. Therefore, the present study was conducted to achieve the following objectives: (1) to assess features of vertebral rotation in left curve of scoliosis (LS) and right curve of scoliosis (RS) in ADS patients, (2) to explore the effects of the vertebral rotation on the position of the aorta relative to thoracolumbar or lumbar spine, and (3) to identify factors influencing vertebral rotation for this population.
Methods
Participants
The inclusion criteria were as follows: (i) patients who were diagnosed as ADS by clinical symptoms and radiological data; (ii) apical vertebrae were located within the thoracolumbar spine or lumbar spine (T12-L4); (iii) the existence of magnetic resonance imaging (MRI) findings of the thoracolumbar spine and lumbosacral spine, and (iv) the existence of posteroanterior and lateral radiographs containing lumbar spine and the whole spine. The exclusion criteria were as follows: (i) congenital vascular malformation; (ii) history of spinal fusion; or (iii) history of cardiovascular surgery.
All ADS patients were treated by the same senior surgeon during general anesthesia. The patient was in the prone position and a posterior two-portal approach was used; also, posterior exposure of the spinous process and laminae was performed. Asymmetrical pedicle subtraction osteotomy was performed and a convex-sided posterolateral wedge osteotomy was applied to correct scoliosis and restore sagittal balance. Patients underwent posterior spinal fusion using the PEEK Rod System or pedicle-screw-based constructs.
This retrospective single-center study was approved by the Ethics Committee of Peking University People’s Hospital (Beijing, China) (No. 2018PHC076) and all participants signed informed consent. According to studies on similar studies,3,4,9 the effect size |ρ| of all parameters ranged from 0.35 to 0.60 among patients with ADS. We defined the α error possibility as 0.05 and the power (1 – β error possibility) was 0.90, so the minimal sample was 65 in the protocol. Thus, a total of 71 patients with ADS were recruited from January 2014 to June 2018. There were 40 cases with LS (LS group) and 31 cases with RS (RS group). All subjects provided written informed consent prior to commencing the study.
Measurements
X-ray radiography
The standard chest examination was carried out, consisting of posterior–anterior and lateral X-ray films of the lumbar and whole spine to identify (1) LS and RS, (2) Cobb angle [degrees (°)], (3) apical vertebrae distribution, (4) coronal horizontal movement (millimeters) (the vertical distance from curvature apex to the sacral vertical line), and (5) the angle of thoracolumbar kyphosis (TLK) (the sagittal angle between the superior endplate of T10 and the inferior endplate of L2, of which the kyphosis was a positive value in kyphosis patients).
In addition, Nash–Moe classification (0–IV Grade; a higher grade meant a more severe vertebral rotation degree) was also measured, which reflected the vertebral rotation degree and was only acquired on apical vertebrae region. 9 Two investigators calculated the above-mentioned parameters independently.
MRI
All subjects were asked to lie in a neutral supine position. MRI was conducted using a 1.5-T scanner (Gyroscan Intera; Philips Medical Systems, Amsterdam, Netherlands). Axial 4-mm slices with 1-mm overlap were acquired using a three-dimensional thick T2-weighted spin-echo axial scan through the vertebral bodies (repetition time: 5000 ms; echo time: 120 ms; field of view: 250 mm; matrix size: 250 × 360). The same MRI and image acquisition protocol was applied for patients lying in the supine position and images were analyzed using PACS software (Easy Vision IDS5, version 11.4; Philips, Hamburg, Germany). To clarify the relative positions of the abdominal aorta and the vertebrae, the following parameters were measured from the magnetic resonance images from the T12 vertebrae to the L5 vertebrae with a Cartesian coordinate system.
Cartesian coordinate system: a line connecting both medial edges of the superior facets was defined as the X-axis. The Y-axis was drawn perpendicular to the X-axis starting from the dorsal edge of the right superior facet and the two lines intersect at the origin “O”.
Left pedicle-aorta angle (α): the angle formed by the Y-axis and a line connecting the origin and the center of the aorta was defined as the left pedicle–aorta angle (α). The angle was defined as 90° when the aorta was located directly to the left, and −90° when it was located directly to the right of the original point.
Left pedicle–aorta distance (d): this distance was defined as a line connecting the origin O and the nearest edge of the aorta.
Vertebral rotation angle (γ): it was defined as the angle subtended by a straight line through the posterior central aspect of the vertebral foramen and the middle of the vertebral body and the sagittal plane (Figure 1).

The position of the Cartesian coordinate system and instructions for α, γ, and d.
Statistical analysis
The value of each parameter at each vertebral level was presented as mean ± standard deviation (SD). Independent-samples t-test was performed on respective comparisons of gender, age, body mass index (BMI), Cobb angle, coronal horizontal movement between LS and RS groups. Mann–Whitney U-test was used to compare the distribution of apical vertebrae and Nash–Moe rotation classification between the two groups. One-way analysis of variance and the Kruskal–Wallis test were used to compare variables on different levels of apical vertebrae in the same group. Pearson correlation and Spearman correlation analysis were respectively utilized to assess the correlation of the rotation angle and Nash–Moe classification to Cobb angle, the coronal horizontal movement, α, and d between the two groups. Ordinal logistic regression was used for determining the risk factors of Nash–Moe classification in the two groups. Multiple linear regression analysis was utilized to identify risk factors for γ. The data were statistically analyzed using SPSS 22.0 software (IBM, Armonk, NY, USA) and p < 0.05 was considered statistically significant.
Results
There was no significant gender-based difference between LS and RS groups (p = 0.413). The age was well-matched in LS and RS groups (p = 0.126), as well as BMI (p = 0.232) (Table 1).
Demographic characteristics of deformity and control participants.
BMI, body mass index; LS, left scoliosis; RS, right scoliosis.
X-ray radiography
In the two groups, L1 to L4 were distributed as apical vertebrae, in which L3 was the most frequent in LS group, while L2 was the most frequent in RS group. There was no significant difference in distribution of apical vertebrae between LS and RS groups. The average Cobb angle and coronal horizontal movement were not significantly different between the two groups (p = 0.311 and 0.394, respectively). In apical vertebral region, Nash–Moe rotation classification was mainly in Grade I and II in both groups, and there was no significance in distribution between the two groups (Table 2).
Cobb angle, Nash–Moe classification in Ap-V, Ap-V distribution, and coronal horizontal displacement distance in two malformed groups.

Ap-V, apical vertebrae distribution; LS, left scoliosis; RS, right scoliosis; TLK, thoracolumbar kyphosis.
MRI findings and the results of correlation analysis
There was no significant difference in γ among different levels in LS group (F = 1.165, p = 0.337), and among different levels in RS group (F = 1.427, p = 0.253) (Table 2).
The results of Pearson’s correlation analysis demonstrated a significant correlation among the γ, Cobb angle, and coronal horizontal movement in the LS group (p < 0.001). Also, there was a significant correlation among the γ, Cobb angle, and coronal horizontal movement in the RS group (p < 0.001). However, no significant correlation was noted among the γ, α, and d in the LS group (p = 0.908 and 0.661, respectively), and there was no significant correlation among the γ, α, and d in the RS group (p = 0.738 and 0.289, respectively). In LS group, Nash–Moe classification correlated to Cobb angle, coronal horizontal movement, and TLK. In RS group, it correlated to Cobb angle and coronal movement. (Table 3). Figures 2 and 3 show that when there was a greater Cobb angle and coronal horizontal movement, there was a larger γ in LS group and a lower γ in RS group (Figures 2 and 3).
Pearson correlation analysis between Cobb angle, the horizontal displacement, TLK, α, d, and the vertebral rotation degree.

The Nash–Moe classification was measured in only the apical vertebral region, so in this column, α and d were also obtained in only the apical vertebral region.
LS, left scoliosis; r, correlation coefficient; RS, right scoliosis; TLK, thoracolumbar kyphosis.

Scatter diagram between mean γ and Cobb angle or coronal movement. (a) Correlation between mean γ and Cobb angle in LS group, R2 = 0.324; (b) correlation between mean γ and coronal movement in LS group, R2 = 0.454; (c) correlation between mean γ and Cobb angle in RS group, R2 = 0.588; (d) correlation between mean γ and coronal movement in RS group, R2 = 0.529.

The standard standing whole spine X-ray and lumbar spine MRI T2-weighted axis-image of LS and RS groups. (a and b) The whole spine X-ray and L3 level MRI of a 61 year-old woman in LS group. The γ is 6.3°; the apical vertebrae is L3, Cobb angle is 16.7°, and coronal movement is 32.4 mm; α is −4.8° and d is 5.22 cm. (c and d) The whole spine X-ray and L3 level MRI of a 67 year-old woman in LS group. The γ is 13.6°; the apical vertebrae is L3, Cobb angle is 22.3°, and coronal movement is 43.6 mm; α is −4.8° and d of 5.33 cm. (e and f) The whole spine X-ray and L3 level MRI of a 63 year-old woman in RS group. The γ is −10.8°; the apical vertebrae is L3, Cobb angle is 19.2°, and coronal movement is 36.4 mm; α is 5.9° and d of 5.73 cm. (g and h) The whole spine X-ray and L3 level MRI of a 68 year-old woman in RS group. The γ is −16°; the apical vertebrae is L3, Cobb angle is 25.2°, and coronal movement is 45.7 mm; α is 6.6° and d of 5.75 cm.
Regression analysis of vertebral rotation degree
Ordinal logistic regression analysis of Nash–Moe rotation classification was also performed based on correlation analysis. In LS group, there was no identified risk factor for Nash–Moe classification in the apical vertebral region. In RS group, the Cobb angle was the independent risk factor for Nash–Moe classification, where Nash–Moe classification = 0.03 × Cobb angle (°) +0.92 (Nash–Moe classification is integer). More specifically, when Cobb angle < 36°, Nash–Moe classification belonged to Grade 0 to II, and Grade III corresponds to the Cobb angle of 36–70°, generally.
Multiple linear regression analysis of γ was also performed based on correlation analysis. In LS group, coronal horizontal movement was a risk factor for γ (p = 0.003), and the regression equation was γ (°) = −4.502 + 0.542 × coronal horizontal movement (mm). In RS group, γ was affected by Cobb angle (p = 0.001) and coronal horizontal movement (p = 0.006), and the regression equation was γ (°) = 2.953–0.512 × Cobb angle (°)–0.406 × coronal horizontal movement (mm) (Table 4).
Multiple linear regression analysis of γ in LS and RS groups.
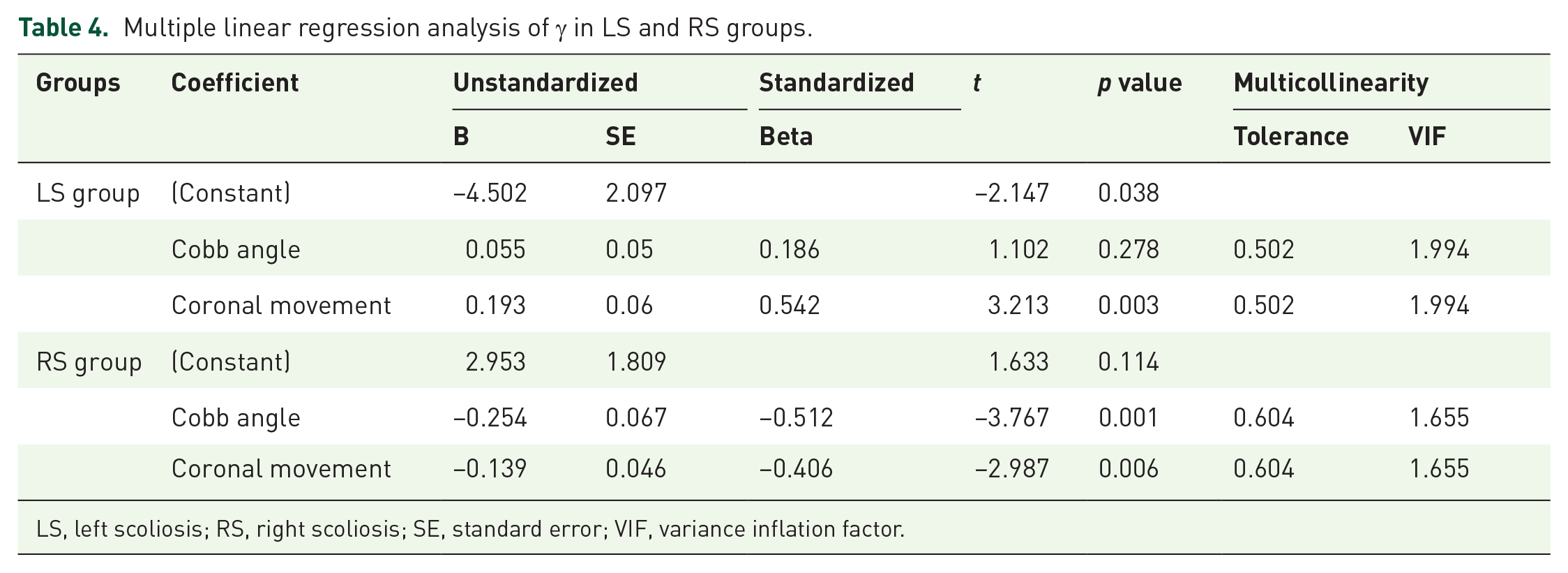
LS, left scoliosis; RS, right scoliosis; SE, standard error; VIF, variance inflation factor.
Discussion
A previous study indicated a significant correlation between the vertebral rotation and the clinical symptoms irrespective of the degree of scoliosis. 10 Although the exact mechanism of the vertebral rotation in ADS has been defined, it was assumed that asymmetrical degeneration of facet joint is worthy of consideration.11–13 Due to the asymmetry in the orientation of facet joint, the facet position was abnormal and the distribution of mechanical loads and stress in the spine changed, which may be a potential cause of spinal degeneration14–16 and instability.17–21 Faraj et al. 22 evaluated the relationship between apical vertebral axial rotation and pretreatment patient-reported health-related quality of life, disability, and pain in patients with ADS using a novel radiographic software tool. They found that increased apical vertebral axial rotation was associated with suboptimal pretreatment health status scores. Furthermore, a number of researchers demonstrated that the vertebral rotation can lead to the pain that is caused by the degeneration of the facet joints or the decreased foraminal width.13,23 Therefore, the vertebral rotation is an important index for indicating the severity of the ADS. In the present study, a positive correlation was noted among the vertebral rotation, Cobb angle, and coronal horizontal movement, consistent with findings of previous studies. Thus, we can use γ to evaluate the severity of ADS in clinical practice.
To our knowledge, the vertebral rotation in patients with AIS significantly affects the position of the aorta. Milbrandt and Sucato 24 determined the position of the aorta in patients with LS and compared these findings with those observed in normal patients. Their results revealed that in LS, the aorta is positioned more anteriorly and to the right (toward the concavity) compared with patients with a straight spine. This position may allow full access to the convexity of the left curve to perform an anterior fusion/release as well as instrumentation. Liljenqvist et al. 25 concluded that idiopathic scoliosis is associated with distinctive intravertebral deformity, with smaller pedicles on the concave side and a shift of the dural sac toward the concavity. Sevastik et al. 26 pointed out that rotation and the anterior displacement of the vertebral body in scoliosis result in a deviation of the aorta along the left (concave) side of the vertebral body to a more posterior position relative to the vertebral body with a possible increased length of the intercostal artery on the right (convex) side. Studies that concentrated on the position of the aorta in patients with AIS showed that it changed at different vertebral rotations.24,27,28 However, the effects of vertebral rotation on the position of the aorta in patients with ADS remain elusive.
In the current research, a quantitative relationship between vertebral rotation and radiological parameters depending on X-ray was first established. Then, the regression equation indicated that vertebral rotation in segments with scoliosis could be influenced by Cobb angle and coronal horizontal movement, which was of great significance for correlating parameters depending on X-ray and MRI findings. Next, when there was a lack of MRI due to different constraints, vertebral rotation could still be predicted by X-ray, and thus, the direction of implantation of pedicle screws could be identified. In addition, Nash–Moe rotation classification is a world-wide known index for the grade of vertebrae rotation and it can be measured on X-ray, which was full of significance for lower cost without MRI and for rapid clinical strategy. 9 To an extent, it was more suitable than γ since the latter parameters could be acquired only on MRI. However, there were some differences in risk factors for the rotation degree between LS and RS groups, which may be related to small sample size of the current study. Then, Nash–Moe rotation classification is ranked data but not a continuous valuable such as γ angle, and the Nash–Moe rotation classification in degenerative scoliosis, unlike idiopathic scoliosis, was mainly in lower grade, so it could be a reporting bias in revealing the relationship between Cobb angle and the rotation classification.9,29
Due to the vertebral rotation, the structure of the vertebrae is complex and unclear, therefore, the insertion of pedicle screws is associated with difficulty and may cause aortic injury. Although ADS typically becomes more complicated in elderly patients, the arterial elasticity is reduced and is commonly accompanied by atherosclerosis. 30 Therefore, it is highly essential to indicate the effects of vertebral rotation on the position of the aorta in patients with ADS to guide spine surgeons and to reduce the risk of vascular complications. In the present research, the effects of vertebral rotation on the position of aorta in patients with ADS were found to be different from those in patients with AIS, which can be justified in the following. AIS is frequently manifested as a regular and smooth curve with a larger Cobb angle. However, ADS is mainly caused by the degeneration of intervertebral discs, facets, and paravertebral muscles, in which the curve is irregular and the Cobb angle is typically <40°.31,32 Also, ADS patients are mainly of advanced age and with atherosclerosis; thus, the vascular elasticity can be reduced, and the tethering ability of connective tissues can be alleviated, which can lessen the effects of the vertebral rotation. Hence, the vertebral rotation has no significant influence on the position of the aorta in patients with ADS.
In spine surgeries, vascular injury is rare but a catastrophe, manifested as acute bleeding, pseudoaneurysm, or arteriovenous fistula.33,34 Liu et al. 35 indicated that the risk of aortic injury caused by the misplacement of screws would increase owing to the vertebral rotation. Owing to the vertebral rotation, misplaced pedicle screws are associated with potential risk factors. During the screw insertion process, we typically determine the Cobb angle according to the vertebral rotation to ensure the accuracy of screw insertion. For patients with ADS, the effects of the vertebral rotation on the screw insertion have been studied by several researchers. In the present research, it was revealed that the vertebral rotation has no significant influence on the position of the aorta in patients with ADS. Therefore, the position of the aorta in patients with ADS did not change with vertebral rotation. In other words, the aorta is maintained in a relatively normal position in patients with ADS. Thus, we can evaluate the thread angle of a screw and the position of the aorta simultaneously according to vertebral rotation. It not only ensures the safety of screw insertion, but also avoids aortic injury.
There are a number of limitations in the present study. First, patients mainly lay in supine position during MRI, while surgery was carried out in prone position. However, it is not clear whether the position of the aorta changes from supine position to prone position. Second, the vertebral rotation mainly affects the coronal balance, while its influence on sagittal balance remains elusive. Therefore, the conclusion may not be applicable to all ADS cases. Third, the number of the cases in the current study was relatively small, thus, further studies with larger sample size need to be conducted.
Conclusion
In summary, there was a positive correlation among vertebral rotation, Cobb angle, and coronal horizontal movement, and it was revealed that vertebral rotation degree could be calculated by Cobb angle or coronal movement without MRI findings. Surgeons can use this strategy to evaluate the severity of deformity for patient with ADS. There was no significant correlation between the vertebral rotation and the position of the aorta, which indicated that the aorta was maintained in a relatively normal position in patients with ADS. Thus, the approach is of great significance for surgeons in order to avoid aortic injury.
Footnotes
Acknowledgements
We acknowledge Yonggang Zhang who contributed towards the study by making substantial contributions to design and acquisition of data.
Author contributions
Yan Liang carried out the molecular genetic studies, participated in the sequence alignment and drafted the manuscript. Shuai Xu and Yongfei Zhao participated in the design of the study and performed the statistical analysis. Keya Mao and Haiying Liu conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
Please contact author for data requests.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Consent for publication
All individual persons’ consent to publish their data.
Ethics statement
This retrospective study was approved by the Institutional Review Board (IRB) of Peking University People’s Hospital and 301 Hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China. NO: 51772328. National Key R&D Program of China (grant number: 2016YFC0105606). The procurement of Government of National Health Commission of China, Grant number: 2127000218.
Informed consent
All patients involved in the study consent to participate in the study. And the written consent has been obtained from all the patients.