
Abstract
Background:
The capacity of children with hemiplegia to be engaged in anticipatory action planning is affected. There is no balance among spatial, proprioceptive and visual information, thus altering the affected upper limb visuomotor coordination. The objective of the present study was to assess the improvement in visuomotor coordination after the application of a unimanual intensive therapy program, with the use of unaffected hand containment compared with not using unaffected hand containment.
Methods:
A simple blind randomized clinical trial was realized. A total of 16 subjects with congenital infantile hemiplegia participated in the study with an age mean of 5.54 years old (SD:1.55). Two intensive protocols for 5 weeks of modified constraint-induced movement therapy (mCIMT) or unimanual therapy without containment (UTWC) were executed 5 days per week (2 h/day). Affected upper limb visuomotor coordination (reaction time, task total time, active range, dynamic grasp) was measured before–after intensive therapy using a specific circuit with different slopes (10°/15°).
Results:
Statistically significant inter-group differences were found after the intervention, with clinically relevant results for the mCIMT group not seen in UTWC, in the following variables: reaction time 10°slope (p = 0.003, d = 2.44), reaction time 15°slope (p = 0.002, d = 2.15) as well as for the task total time 10°slope (p = 0.002, d = 2.25), active reach 10°slope (p = 0.002, d = 2.7), active reach 15°slope (p = 0.003, d = 2.29) and dynamic grasp 10°/15°slopes (p = <0.001, d = 2.69). There were not statistically significant inter-group differences in the total task time with 15°slope (p = 0.074, d = 1.27).
Conclusions:
The use of unaffected hand containment in mCIMT would allow improvements in the affected upper limb’s visuomotor coordination. Thus, it would favor clinical practice to make decisions on therapeutic approaches to increase the affected upper limb functionality and action planning in children diagnosed with infantile hemiplegia (4–8 years old).
Introduction
Infantile hemiplegia is the second most frequent type of cerebral palsy, 1 causing a motor deficit of the hemibody contralateral to the injured hemisphere, with more affectation in the upper limb than the lower limb.2,3 Children with hemiplegia have a lesion in the corticospinal tract that produces an alteration in the grasp and the production of force in advance (anticipation control), altering the affected upper limb visuomotor coordination.4–6 An important aspect of motor control is motor planning. Motor planning can be defined as the ability to take the upcoming task demands into account when first taking hold of an object.6–8 Reaching and grasping require the neural system to preplan a motor plan(s) (i.e. feedforward control) and use sensory feedback (i.e. feedback control) to monitor motor errors and modify ongoing movements accordingly. 9 The affected upper limb moves more slowly and less continuously during reaching than the upper limb of children of typical development. 10
Constraint-induced movement therapy (CIMT) is designed to improve the affected upper limb motor function after stroke and consists of three key components: (1) repetitive, task-oriented training; (2) adherence-enhancing behavioral strategies (transfer package); and (3) constraining the use of the less affected arm, usually by wearing a mitt. 11 Modified CIMT (mCIMT) was reported by Page et al. 12 using less than 3 h of therapy per day. mCIMT has been shown to be an effective method to promote the functional use of the more affected upper limb in children with hemiplegia, and its application at home provides a rich natural context to facilitate motivation, engagement, and repetition in everyday functional activities.13–15 Therapy at home is an essential way to increase the amount of training. Families educated by therapists can carry out a daily therapy intervention, which has shown great contribution to and satisfaction in learning new skills in their children. 16 Thus, mCIMT applied at home would improve visuomotor coordination and, therefore, action-planning control. This could be due to the use of unaffected hand containment and the execution and repetition of unimanual tasks with the affected hand; 17 its effect was demonstrated through the increase in the quality of movement and spontaneous use of the affected upper limb in children with hemiplegia (4–8 years old). 18 In addition, Tervahauta et al’s. 19 systematic review showed that the results in the affected upper limb function (measuring spontaneous use, quality of movement, bimanual functional performance, manual ability, etc.) after the application of intensive therapies such as mCIMT and bimanual intensive therapy (BIT) are similar. 19 That is why it is suggested that the main ingredient, and therefore the key to success, may be sufficient repetitions over many hours of training.20,21 However, the benefits within visuomotor coordination in the comparison of both therapies have not been studied.
When the same dose of mCIMT is compared with other interventions such as conventional therapy, even greater benefits are obtained after mCIMT, with improvements in the reaction time. 14 This may suggest that the unaffected hand containment within a protocol of intensive unimanual therapy (mCIMT) could be a factor to be considered to promote visuomotor coordination of the affected upper limb. The assessment of visuomotor coordination through a specific circuit with a mobile object at different speeds allows determination of the reaction time, total task execution time and the executed reach, including the dynamic grasp used and how the visuomotor coordination is adapted with speed changes, which is related to action planning and anticipation. 22
In addition, the present study was focused on determining which intensive therapies allow favoring visuomotor coordination in children with hemiplegia, by addressing these limitations using intensive therapies with unaffected hand containment, like mCIMT, or without containment. This method allows assessment of the efficacy of unaffected hand containment and, therefore, enables choosing the most beneficial intervention to increase visuomotor coordination of the affected upper limb in infantile hemiplegia, as well as improving action planning. Thus, the objective of the present study was to assess the improvement in visuomotor coordination after the application of a unimanual intensive therapy program with the use of unaffected hand containment compared with not using unaffected hand containment.
Methods
Study design
A single-blind, randomized, controlled, pilot trial was conducted in which objective was to study the feasibility, the measurement instrument, the study variables, and the adaptation of children and families in the execution of the protocol at home, to know if the proposed activities were suitable for children, if the therapist–family follow-up was a necessary support, or if different aspects should be modified, before developing a research project with a greater number of participants. For this, it was necessary to run a preliminary study to know the results obtained in the measurement test used and thus be able to establish a correct difference in the variables to obtain the calculation of the randomized clinical trial sample size that may be developed in the future. The study protocol was approved by the Clinical Research Ethics Committee of the CEU-San Pablo University of Madrid (reference number 060-13). This pilot trial has been registered with ClinicalTrials.Gov, and the registration number is NCT02178371.
Participants
The participants were recruited from the rehabilitation department of the Hospital of Toledo (Spain) from January 2015 to December 2017. Through convenience sampling, 16 children diagnosed with congenital hemiplegia were recruited, following the inclusion and exclusion criteria, and randomly divided into experimental and control groups. A blinded physiotherapist performed the randomization. The randomization method was carried out through the Epidat software version 4.2 which, following a process of simple randomization and consecutive sampling, divided the participants into two groups (experimental and control) with eight participants per group. A number sequence was obtained, and kept in opaque closed envelopes. The envelope was opened by the blinded physiotherapist, who decided randomly, according to the randomization sequence.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) congenital infantile hemiplegia, (2) aged between 4 and 8 years, (3) lack of use of the affected upper limb (levels from 2 to 7 of the Modified House Classification (MHC), 23 (4) exceeding 10° extension of metacarpophalangeal and interphalangeal joints and completing 10° active extension of the wrist joint, (5) levels I–III in the Manual Ability Classification System (MACS), 24 and (6) adequate cognitive development to understand verbal orders for the proposed tasks and cooperation in their execution. The exclusion criteria were defined as follows: (1) severe visual problems that prevent the independent execution of unimanual tasks, (2) significant balance disturbances that impede the execution of the tasks, (3) diseases not related to hemiplegia, (4) pharmacoresistant epilepsy, and (5) botulinum toxin infiltration within 3 months prior to the intervention.
Intervention pre-conditions, intervention, and follow-up
Before conducting intervention, an informational meeting was held for all families and children, who were informed about the therapies and the protection of their data, and their right to leave the study freely and without penalties. A physiotherapist provided verbal and written information about the study to the families and checked the inclusion and exclusion criteria, and then the families were informed about the possible complications: low tolerance to daily intensity and refusal to use the affected hand in the activities or wear containment on the unaffected hand. Finally, parents signed the informed consent and children affirmed their agreement verbally. This physiotherapist was also in charge of collecting the signed informed consent and then randomizing the participants to the corresponding group. A neuropediatric physiotherapist was responsible for performing all the patients’ assessments.
After the meeting, families were trained by a physiotherapist in the execution of the specific therapy, teaching them how they should carry out the unimanual activities at home. The therapy was only started once all families were confident about the treatment use.
Two intensive 5-week protocols were carried out: mCIMT (experimental group) and unimanual therapy without containment (UTWC) (control group). In both groups, the protocol was programmed to last 2 h per day (not continuous; that is, separated by at least 30 min of rest) from Monday to Friday, with a total therapeutic dose of 50 h, and the therapies were carried out by the children’s families in their usual environment to encourage the learning of the affected upper limb within daily activities. The unimanual tasks were the same for both groups, based on shoulder flexion–elbow extension, forearm supination and grasp–release of objects with the affected hand (Table 1). Each activity had to be conducted for 10 min. The unaffected hand was partially contained for mCIMT and free for UTWC; each family built the partial containment as a glove with a rigid cardboard base to avoid mirror movements, leaving the wrist joint free (Figure 1). The families had to fill in a table with the execution time of each activity and the child’s behavior on it. Weekly online follow-up between the families and the therapist was implemented to avoid any complications and increase treatment adherence. In this follow-up, the therapist explained the activities and the families conducted them, accordingly, commenting their doubts. The families could contact the therapist every day to make possible changes if the child could not perform the tasks or was not motivated. This fostered adherence to and motivation for the intervention.
Examples of the designed tasks to perform with mCIMT and UTWC.
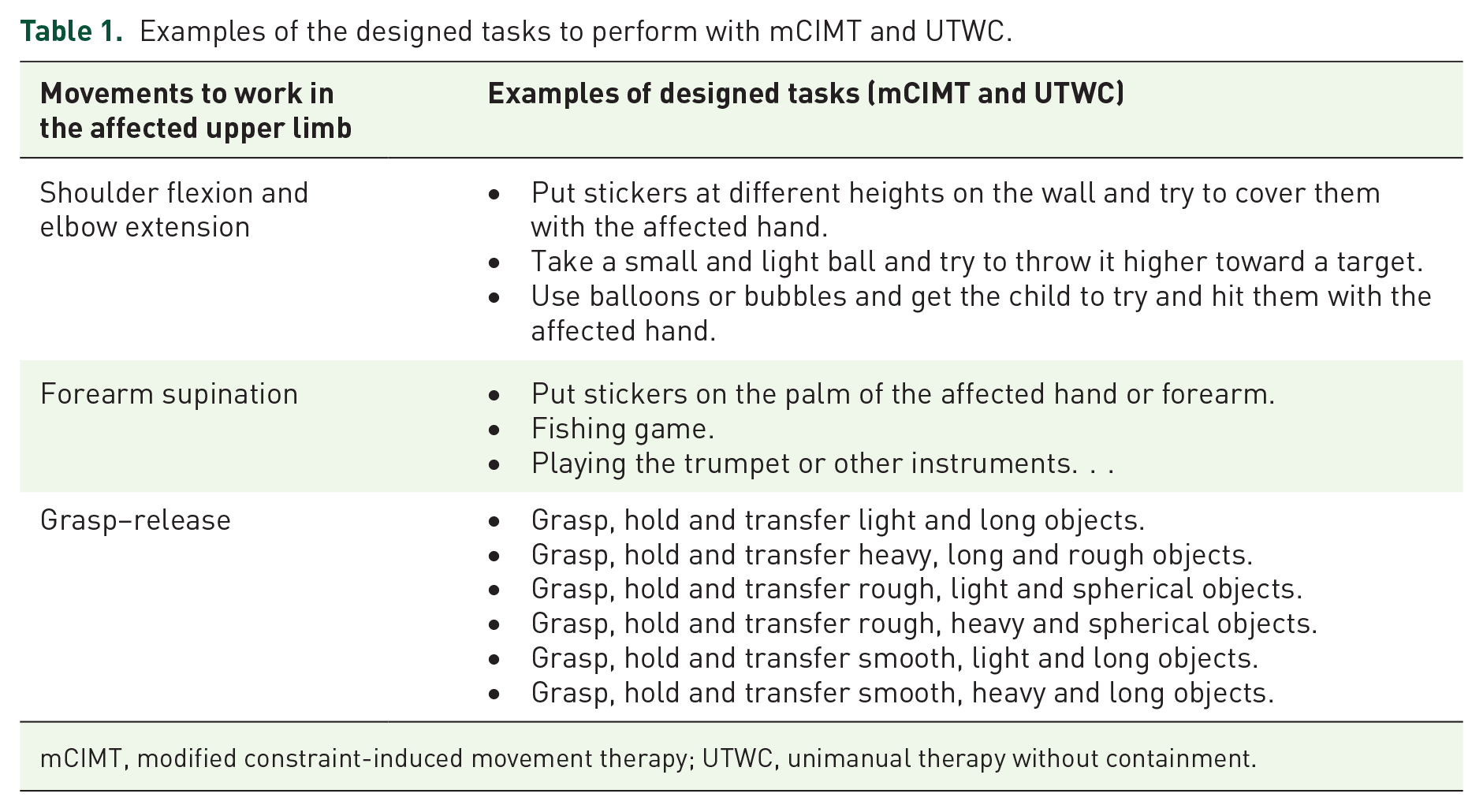
mCIMT, modified constraint-induced movement therapy; UTWC, unimanual therapy without containment.

Unimanual therapy with and without containment. The first image (a) shows the activity: grasp, hold and transfer rough, light and spherical objects, without containment. The second image (b) shows that the unaffected hand is containment and the child executes the same movement (grasp–release) with the affected hand, in the similar activity with smaller objects.
Data collection
Two assessments were performed. The first assessment was focused on obtaining the data before the treatment, that is, in week 0 (baseline situation, immediately before starting treatment), and the second assessment was conducted at the end of the treatment, that is, in week 5 (a total dose of 50 h).
Outcome measures
The visuomotor coordination of the affected upper limbs is distributed in three variables: reaction time (seconds, s), total movement time to execute the proposed task (seconds, s) and affected upper limb active range when stopping a car in motion (centimeters, cm). Thus, it was measured with a wooden circuit consisting of a ramp with two possible slopes (10° and 15°) based on the Mak study. 22
The reaction time assessment started when the child received the verbal command “now,” and he/she had to press a switch placed at the lower end of the ramp with the affected hand and pick up the car (with a dynamometer 25 ) in motion. The active range and the dynamic grasp were assessed when the child pick up the car. The total movement time of the task was registered from the moment the child pressed the switch until he/she placed the car on the tray situated on a chair by the healthy side (Figure 2). A total of five trials were allowed, and only those in which the children took the car were counted as valid. Two slopes (10° and 15°) were used to study the influence of speed.

Circuit with different slopes to assess visuomotor coordination, with a car attached to an electromagnet with a dynamometer. Figure shows the child receiving the verbal order “now” and pressing the switch with the affected hand to activate the car. Then, child must transport the car to the tray placed homolateral to the healthy upper limb, thus completing the task, and the total execution time.
Statistical analysis
Statistical analysis of the data was performed using SPSS v20.0 for Windows (SPSS Inc., Chicago, IL, USA). Given the small sample size, non-parametric analyses were used with the Mann–Whitney U-test to determine the inter-group differences for the variables. The Wilcoxon test for paired samples was performed to compare before–after treatment results in the same group for both therapies. Fisher’s exact test was used to determine inter-group differences according to sex, MACS level and the affected hemibody. The effect size (d) of differences was calculated to know the magnitude of the difference between groups. The results are shown as the median and interquartile range (IQR) with a confidence interval of 95%. All those values with p value < 0.05 were considered statistically significant.
Results
A total of 32 subjects were recruited, of which 14 were excluded for not meeting the inclusion criteria and another two eventually decided not to participate. The remaining 16 subjects met the inclusion criteria established and were randomly allocated in either of the two intervention groups. Eight children were included in the mCIMT group and the other eight children in the UTWC group (Figure 3).
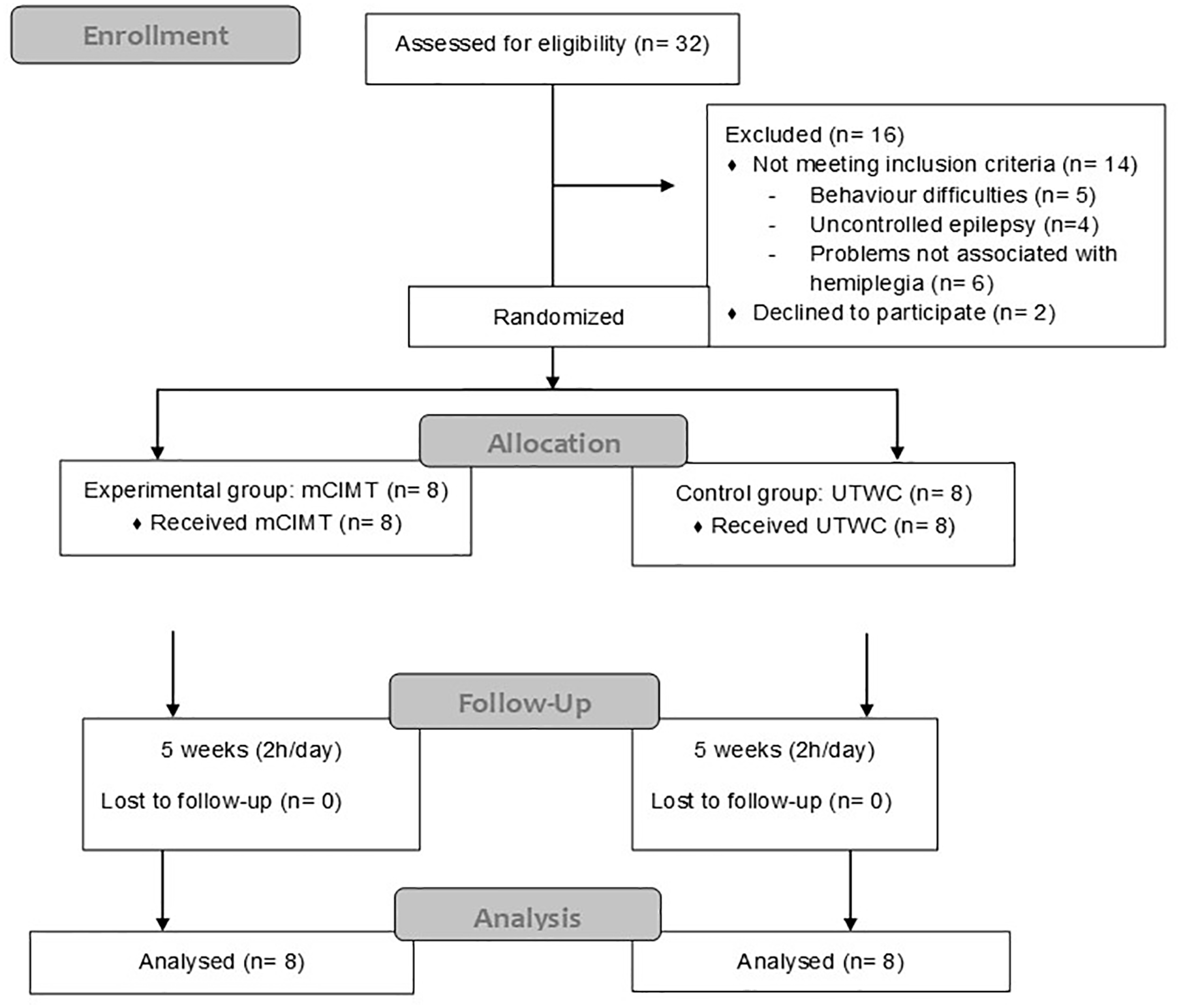
Consort flow diagram. Allocated of sample, performed therapies and analysis.
The age range of the participants was 4–8 years, with an average of 5.54 years (SD = 1.55). Fifty percent were males and the other 50% were females, of which 62.50% had left hemiplegia, with the involvement of the right half of the body being less representative (37.5%), and the affected side was the non-dominant in all participants. In the MACS, 56.25% were classified as level II. All these children were classified as MHC level 5 (fair active assist: can actively grasp object and stabilize it well), and perinatal stroke was the cause of the infantile hemiplegia in 100% of participants (Table 2). Fisher’s exact test did not show significant differences for sex, MACS level and the affected side of hemiplegia (Table 2). In the Mann–Whitney U-test, there were not statistically significant inter-group baseline differences for age (p = 0.78, Table 2), task total time with 10°/15° slopes (p = 0.073; p = 0.071), reaction time with 10° slope (p = 0.064) and dynamic grasp with 10°/15° slopes (p = 0.32 for both), shown in Table 3.
Characteristics of participants.

F, female; M, male; MACS, Manual Ability Classification System; mCIMT, modified constraint-induced movement therapy; UTWC, unimanual therapy without containment.
Statistical significance when p value is < 0.05 (inter-group differences).
Results for visuomotor coordination at baseline (week 0) and after intervention (week 5) in both intervention groups.
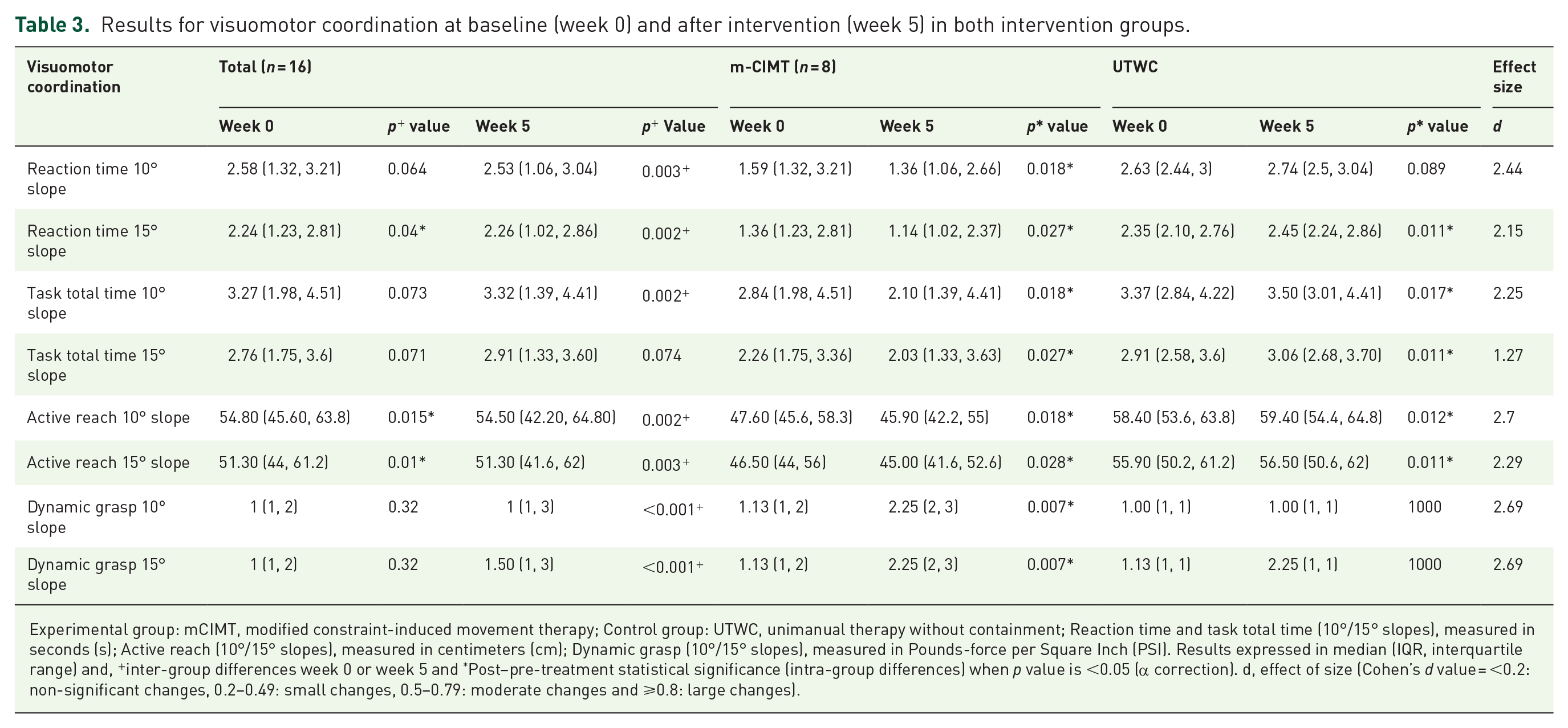
Experimental group: mCIMT, modified constraint-induced movement therapy; Control group: UTWC, unimanual therapy without containment; Reaction time and task total time (10°/15° slopes), measured in seconds (s); Active reach (10°/15° slopes), measured in centimeters (cm); Dynamic grasp (10°/15° slopes), measured in Pounds-force per Square Inch (PSI). Results expressed in median (IQR, interquartile range) and, +inter-group differences week 0 or week 5 and *Post–pre-treatment statistical significance (intra-group differences) when p value is <0.05 (α correction). d, effect of size (Cohen’s d value = <0.2: non-significant changes, 0.2–0.49: small changes, 0.5–0.79: moderate changes and ⩾0.8: large changes).
Statistically significant inter-group differences were found after the intervention, with clinically relevant results for the mCIMT group, but not for UTWC, in the variables: reaction time with 10°slope (p = 0.003, d = 2.44), reaction time with 15°slope (p = 0.002, d = 2.15) as well as for the total task time with 10°slope (p = 0.002, d = 2.25), active reach with 10°slope (p = 0.002, d = 2.7), active reach with 15°slope (p = 0.003, d = 2.29) and dynamic grasp 10°/15°slopes (p = <0.001, d = 2.69). There were not statistically significant inter-group differences in the task total time 15°slope (p = 0.074 d = 1.27). All results are shown in Table 3.
For the mCIMT group, a greater reduction in the reaction time was obtained for the 10° slope (0.23 s; p = 0.018) compared with that obtained for the 15° slope (0.22 s; p = 0.027), as well as for the total task time for the 10° slope (0.74 s; p = 0.018) and for the 15° slope (0.23 s; p = 0.027). In the active range, there was a 0.2 cm reduction for the 10° slope (p = 0.018) with respect to the 15° slope (p = 0.028). In the dynamic grasp, the same increase (1.12 PSI) in force was obtained for both slopes (before and after treatment) (p = 0.007).
All the parents completed the weekly follow-up, recording the activities carried out and the time dedicated to each activity until completing the 2 h of daily treatment. It was also recorded when the hours were not completed, in order to calculate the total treatment dose. In relation to compliance to treatment, the mean total dose recorded for the mCIMT and UWTC groups was 48 h (96% of total dose) and 47 h and 30 min (95% of total dose), respectively. Therefore, they achieved more than 92% of the compliance to treatment proposed in our study, based on the research of Ferre et al. 16 on intensive home therapies.
Discussion
Children with hemiplegia have visual delay when paying attention to an object, which generates a deficit in action planning, as vision precedes motor action, and the action is delayed by the analysis of the task and its sequence. 26 The affected upper limb visuomotor coordination assessed in this study obtained a favorable result after applying mCIMT therapy performed at home compared with UTWC, which suggests that children would be able to adapt their movement to an increase in car speed (with a 15° slope). This could be due to the fact that the task was simple and did not require a previous thinking strategy at different speeds,6,8,26 and thus, instead of planning the end of the action, they were shown to use a step-by-step planning strategy. That is, they first plan the movement toward the object, and only after having grasped the object do they subsequently plan the next movement.6,8 Thus, better results are obtained for the 10° slope than for the 15° slope, as it would be necessary to modulate the trajectory of the movement to the increase in the speed at which the car descends on the 15° slope in order to complete the task. Speed is a factor that could influence the time that children with hemiplegia require to perform a task with different actions, as task analysis and action planning are altered in this population. Lin et al. 27 found that action planning occurs in children who execute the mCIMT protocol compared with those who do conventional therapy, as there is a reduction in reaction time that also favors the task execution approach. Moreover, as in the mCIMT group of this study, in that of Lin et al. 27 an improvement in the active range was obtained after the intervention with constraint.
The increase in slope, as well as in the speed of the car, did not influence the dynamic grasp for mCIMT or UTWC, as the values were the same for both slopes. When the speed increases, more force is generated in the affected hand to grasp the car. Children with impaired coordination are able to modulate the clamping force at a higher speed for the moving object; compared with a typically developing child, they use more force to give stability. 22 However, children with hemiplegia using the same force without variations compared with a child with typical development are not able to adapt the force in the affected hand, perhaps due to a restriction in movement, a deficit of sensory information, or little unimanual exploration experience. 9 A longer treatment time (over 5 weeks of intervention) may be needed by these children with impaired fine-motor adjustment and lack of dissociation of their fingers, as well as proprioception in their affected hand, to gain experience (trial–error) at adapting the grasp to the shape, texture and weight of the object, thereby allowing the execution of a previous thinking strategy (anticipatory control) to achieve precision in the grasp and to adjust the force to take hold of the object adequately.9,10 An improvement in the stability and force of the grasp allows greater hand functionality when taking objects of various characteristics and holding them during the execution of selective and precision tasks, such as throwing a small ball at an object, keeping the fork stable with the affected hand and bringing food to the mouth during the feeding phase.28,29 Most children with unilateral brain injuries do not develop an adequate grasp force in the coordination of unimanual activities carried out by the affected upper limb. 2 A pathological pattern or an immature state of grasps are produced for this age, resulting in an inadequate synergy of the coordination force that is related to manipulative skill deterioration in the affected hand, depending on the level of injury.30,31
In addition to the intensity of the treatment and the repetition of the tasks, the execution of the latter at home also favors visuomotor coordination. However, the main element that makes this possible is the containment of the healthy upper limb. This was verified in 30 h of mCIMT in the study of Lin et al., 27 in which the reaction time was reduced with respect to that of conventional therapy. This suggests that the containment of the healthy upper limb is essential to allow an increase of visuomotor coordination in the affected upper limb, as well as improving the reach and grasp without the interference of the unaffected hand, as it remains free. The cortical representation and presence of the affected segment would be reduced. 30
The lack of abandonment of intensive care therapies, as well as the correct management at home, as there were appropriate family-therapist follow-ups and no complications, suggests that therapies could be carried out by the parents, thereby guaranteeing that the functional gains are transferred within daily activities.27,31,32 The adherence of the family and child to treatment, active participation and the non-generating parental stress are phenomena that show that the family-centered model is functional thanks to the empowerment of parents through the therapist and allowing the child to experiment and participate in their own environment, leading to greater learning opportunities. 33 The stability of parental stress throughout the intervention would suggest that this may have been an effective strategy for avoiding disruption of the psychosocial family dynamic. In the study of Ferre et al., 34 caregivers who applied 90 h of BIT at home with their children (diagnosed with hemiplegia) demonstrated parental stress levels that are similar to caregivers of typically developing children, because of that in our study, the presence of stability in parental stress levels could be considered due the family adherence of treatment.
Weaknesses and strengths
Although positive results were obtained in the mCIMT group, these should be evaluated with caution due to the small sample size, and it is not possible to generalize the obtained results to the population of children with infantile hemiplegia. Additionally, the sample was not homogeneous in the baseline situation, and although inter-group statistically significant differences were not found for MACS levels, it should be noted that children in the UTWC group showed poorer manual ability than children in the mCIMT group. Therefore, to draw a robust conclusion about the treatment effect, further study in clinical trials with more participants would be worthwhile. There was no long-term follow-up of the results, thus further studies must be performed to prove these results. Despite these limitations, to the best of our knowledge, this study is the first to assess visuomotor coordination divided into these variables to analyze its increase in children with hemiplegia applying unimanual therapy with and without containment. Correct decision-making and clinical practice are important in clinical rehabilitation to improve the affected upper limb function in infantile hemiplegia.
Footnotes
Acknowledgements
We would like to express great thanks all the families and children who participated, and also Santiago Angulo for the statistical analysis.
Author contributions
R.P.C. conceived the study, participated in its design and coordination, collected the data, supported the data analysis, interpreted the data and wrote the article. E.B.E. provided interventions, interpreted the data and wrote the article. S.A.L. provided interventions and interpreted the data. H.R.B. participated in its design and coordination, supported the data analysis, interpreted the data and wrote the article. P.L.M. supported the data analysis and interpretation. I.M.G. supported the data analysis and interpretation. All authors have read and approved the final manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Clinical trial register
ClinicalTrials.gov Identifier: NCT02178371.