
Abstract
Background:
Children with unilateral spastic cerebral palsy (USCP) receive different treatments, including the application of modified constraint induced movement therapy (mCIMT) or bimanual intensive therapy (BIT) to increase affected upper limb functionality. The aim of this study was to compare the effectiveness of two protocols with different proportions and orders of mCIMT/BIT within combined intensive home-therapy in children with USCP (6–8 years old) with high bimanual functional performance, applied by the family.
Methods:
The protocols were performed on 20 children with an average age of 7.12 years [standard deviation (SD): 0.70], allocated to two different combined therapies. The protocols were designed by 100 h of dose for 10 weeks: 80 h of mCIMT followed by 20 h of BIT (mCIMT-B group) and 80 h of BIT followed by 20 h of mCIMT (BIT-mCI group). Bimanual functional performance was measured with Assisting Hand Assessment Scale (AHA) and the affected upper limb-use experience with Children’s Hand-use Experience Questionnaire (CHEQ). Parent satisfaction and expectations with therapy were measured using a specific questionnaire. There were five assessment timepoints (week 0, week 4, week 8, week 10 and week 34).
Results:
There were no statistically significant (p > 0.05) inter- and intra-group changes in the bimanual functional performance of both groups. The affected upper limb-use experience obtained significant changes in BIT-mCI group, with statistically significant differences in the pairwise comparisons between week 0–10 and week 4–10 (p = 0.028) for use of the affected hand and the use of the affected hand to grasp between week 4 and week 8 (p = 0.028). Grasp efficacy and discomfort acquired statistically significant differences only in the BIT-mCI group for pairwise comparisons week 0–week 10/week 4–week 10 (p = 0.035). Although task execution time compared with a typically developing child of the same age obtained statistically significant differences only in the group mCIMT-B for pairwise comparisons week 0–week 8 (p = 0.03), week 0–week 10 (p = 0.03), week 4–week 8 (p = 0.04) and week 4–week 10 (p = 0.03). Family satisfaction and expectations acquired an increase between week 0 and week 10 (p ⩽ 0.02).
Conclusion:
Applying 80 h of BIT for 8 weeks in children with high bimanual functional performance USCP (6–8 years old), executed at home with family involvement would be sufficient to obtain improvements in affected upper limb-use experience, without the need to use combined protocols of 100 h. However, no statistically significant increase in bimanual functional performance would be obtained, with the basal situation of the child being a factor to consider for the execution of mCIMT and BIT.
Registration number and name of trial registry: [ClinicalTrials.gov identifier: NCT03465046]
Introduction
Unilateral spastic cerebral palsy (USCP) is a type of cerebral palsy (CP) that affects the motor control and muscle function of the hemi-body contralateral to the affected hemisphere. 1 The affected upper limb is frequently ignored, and this produces an overcompensation with the unaffected upper limb use, which hinders bimanual tasks. 2 Upper limb dysfunction can range from mild to severe depending on the timing, location, extent and nature of the brain injury. 2 The ability to use the affected upper limb spontaneously is reduced in activities of daily living [conceptualized within the broad ‘Activities and Participation’ domain of the International Classification of Functioning, Disability and Health (ICF)], which has an impact on the patient’s quality of life.3,4 Consequently, children with USCP need to improve their bimanual performance and learn to use the affected upper limb. 5 Experience through therapy should reverse the common behaviour of the affected upper limb and reward its use even in simple tasks such as stabilising (use of the affected hand to hold an object while it is manipulated by unaffected hand within a bimanual task). 5 Different upper-limb interventions are found to improve functionality of the affected upper limb 6 : unilateral capacity, bimanual performance and task performance in children with unilateral USCP as virtual reality, 7 goal-directed training, 8 action observation therapy, 9 robotics, 10 electrical stimulation, 11 mirror therapy, 12 home programs, 13 bimanual therapy and constraint induced movement therapy.14–19
Functional therapy emphasises the learning of motor abilities that are meaningful for the child’s environment in functional situations. They involve the child having an active role in finding solutions to motor problems by practicing repetitive goal-related tasks. 20 The child’s natural environment (home) offers a comfortable and enriched place to encourage learning during the therapy practice for children and their parents, increases the amount of training, favouring the generalisation of learning. 21 Due to the high repetition and opportu-nities offered within the home, the long-term maintenance of the effects obtained from the intervention could be facilitated. 22 Home-based programmes allow the possibility of continuing with an intervention in situations when it is necessary to stay at home for a period of time, such as after surgery, illness or confinement. 23 Further-more, parents can be more involved throughout the process, increasing opportunities for parent–child interaction. 24 This concept means that the family is a key component of the child’s environment, and the relationship with the therapist (through follow up) can be used as the context to deliver critical components (i.e. intensity, repetition, feedback) of the therapies established with the child.25–34
Home-based bimanual intensive therapy (BIT) and constraint-induced movement therapy (CIMT) are found to be among the most used intensive treatment approaches directed to USCP because their application reduces the limitations within the child’s daily activities, obtaining more participation in the natural environment due to increasing functionality of the affected upper limb.28,29,31,32 BIT is a form of functional training (with intensive repetitive practice) and focuses on improving coordination of the two hands using structured task practice embedded in bimanual play and functional activities. It uses the principles of motor learning feedback and neuroplasticity.35,36 CIMT combines repetitive task practice, behavioural training techniques and containment of the unaffected upper limb for 90% of the waking day for at least 2 weeks for ⩾3 h per day.37,38 In CIMT, repetitive practice is delivered along with shaping, during which patients engage in meaningful functional activities with measurable progressions for which they receive positive feedback as the activities become increasingly more difficult.36–38 CIMT is focussed on increasing spontaneous use of the affected upper limb, and two possible mechanisms may lead to more use of the affected limb: overcoming the learned non-use of the more affected arm and use-dependent cortical reorganization. 39 Modified CIMT (mCIMT), which comprises variation to the original CIMT mode, specifically the type of containment, nature of intensive therapy and the hours per day (<3 h) and duration in weeks of the program to improve the adherence of the family and child to the therapy and allow them to follow the protocol.40,41 A significant number of modified mCIMT models have been developed. 4 An essential component of the success of BIT and mCIMT is the application of goal-directed activities and the progression of intensity and frequency across the intervention.33–35 Constraint-induced movement therapy and modified protocols have a significant limitation, that is, they do not allow practice of bimanual tasks. Goals identified by children and their caregivers tend to be bimanual in nature.42–44 This has led to the development of hybrid/combined models of therapy that combine mCIMT and BIT. Different studies have also affirmed the need for bimanual training to follow CIMT and have developed a ‘transfer package’ to address this requirement,45–47 so it would be a treatment option to consider. Children with Manual Ability Classification System (MACS) I–MACS III can be included in either programmes because both would offer assisting hand training. However, in the Hybrid-CIMT programme, strength needs to be sufficient in order to be able to grasp and hold in the first part of the programme where CIMT is performed, and the hand is trained unimanually. 45 The dosage of mCIMT and BIT differs among the articles found in the literature33,44–48; evidence shows that BIT and mCIMT have similar effects when the same dose is compared in children with moderate bimanual functional performance.33,48,49 In the study of Deppe et al., applied in children with unilateral cerebral palsy or other non-progressive hemiplegia (aged 3.3–11.4 years), 45 two intensive protocols were performed with a total dose of 80 h: hybrid-CIMT protocol comprised of 60 h of CIMT and 20 h of BIT in a clinical setting. The results of this study suggested higher treatment gains for more severely impaired children with hybrid-CIMT. This might be explained by assuming that, in these patients, the improvement of isolated unilateral motor functions was of greater value for bimanual hand use and coordination than in those who already exhibited a useful amount of assisting hand abilities in bimanual coordination. 45
Considering the total dose used in the study by Deppe et al. (80 h), 45 we aim to determine whether the application of 80 h of mCIMT or BIT in 8 weeks (2 h/day: 5 days per week: 80 h), at home and conducted by parents, produces similar results in both groups of children with high functional performance who use both hands together in play, spontaneously holding objects in the affected hand with a stable or nearly stable grasp. 50 In addition, we wondered whether a combination of therapies would be necessary after 80 h of the first intervention, adding 20 h of complementary therapy. 45 Thus, two protocols were implemented, with different proportions and order of mCIMT/BIT (80 h of mCIMT, followed by 20 h of BIT; and 80 h of BIT, followed by 20 h of mCIMT) within combined intensive therapy.
This would allow us to address concepts that have not previously been studied with the following objectives: (1) to compare the effectiveness of two protocols with different proportions and order of mCIMT/BIT within combined intensive home-therapy applied by the family; and (2) to know if the order of execution of one therapy or another, the dosage used, or the type of intervention would influence the functionality of the affected upper limb of USCP (6–8 years old) with high bimanual functional performance.
Methods
This study was approved (Reference N: 260) by the Ethics Committee of Toledo hospital complex according to the World Medical Association Declaration of Helsinki. Before the study began, the written informed consent of the children’s families was provided.
Study design
A single-blind (evaluator) comparative effectiveness study was conducted. Participants were allocated randomly into two groups: mCIMT-B and BIT-mCI. Software EPIDAT, version 4.2, generated a list of random numbers that paired both a unique sequential number and the intervention type. Someone outside the study sealed the pairs in tamper-evident envelopes.
Participants
A total of 20 participants were recruited from the association of unilateral cerebral palsy in Spain, HEMIWEB, following the established inclusion and exclusion criteria. Children were allocated randomly to mCIMT-B (n = 10) or BIT-mCI (n = 10) groups. The inclusion criteria were the following: USCP, high bimanual functional performance (63–100 AHA units score; these children used both hands together in play, spontaneously holding objects in the affected hand with a stable or nearly stable grasp, 50 aged between 6 and 8 years, level I–II in MACS, 51 and level I–II in the Gross Motor Function Classification System (GMFCS). 52 The following exclusion criteria were defined: disease not associated with USCP, low cognitive level compatible with attending a special education school, presence of contractures in the affected upper limb that inhibits functional movement, surgery within 6 months prior to treatment, administration of botulinum toxin within 2 months prior to, or during, the intervention and pharmacologically uncontrolled epilepsy.
Intervention, referral physiotherapist training, family training, activities and follow up
Two protocols of combined intensive therapy were designed to be delivered at home: an mCIMT-B protocol consisting of 80 h of mCIMT followed by 20 h of BIT, and a BIT-CI protocol with 80 h of BIT followed by 20 h of mCIMT, with each protocol lasting 100 h and applied throughout a 10-week period (from Monday to Friday). The children were requested to perform the structured activities for two non-consecutive hours, separated by at least 30 min of rest. The families were advised to set aside 1 h in the early afternoon and another hour in the late afternoon to ensure that the child was attentive, frustration-free and effort-tolerant. The treatment was initiated only when the families and children were confident about it. To ensure family safety, the parents had to believe that their involvement in the treatment was adequate and the support they were going to receive from the therapist would help them with any existing complications. Prior to therapy, they had a week to prepare the games and the space where it would take place. During that week, the family was connected online so that they could show the referral physiotherapist the activities to be carried out and assess the proper execution and possible modifications and, if they agreed, the intervention would proceed.
Each family received the instructions and carried out the therapy and follow up with a referral physiotherapist, who received a 30-h training for 3 days in a row about the foundations of the mCIMT and BIT therapies. The first 26 h of training were given by a physiotherapist with extensive knowledge in intensive therapies and experience in its clinical application. The information given was the intervention protocol and the activities to be carried out; the variation of activities were explained taking into account the motivation of the child and the family. The training finished with a workshop (4 h), where a psychologist proposed different strategies to motivate the family and the child to avoid frustration and to improve adherence and active support by the referral physiotherapist.
The family training lasted 2 days (4 h each day) for both groups where the interventions were explained and all possible activities to be planned during both therapies (mCIMT and BIT) were taught. The home program was based on the motor-learning-based approaches, considering different aspects within both interventions: active involvement of the child and the family, goal-oriented, structured and individualised functional tasks for the child, and repetition of the task. 31 The referral physiotherapist and parents discussed the family situation and home environment, for example, objects available that are related to the individual intervention goals. In addition, to avoid complexity of task performance and to improve the family’s confidence, adjustments to the initial posture of the child in which the activity is performed, the choice of objects, etc., were implemented. Two goals (goal-oriented) were established with CHEQ (two goals based on the daily life activities of hygiene and feeding) to consider the child’s bimanual performance.
The activities were designed according to the interest of each child and his or her motivation, they were asked about it and they sent their interests via email to their referral physiotherapist to schedule the activities and practice them during the weekly follow up. For the mCIMT-B group, unimanual activities were defined to improve quantity and quality of movement in the affected upper limb (including specific movements: flexion, abduction and external rotation of the shoulder, extension of the elbow, supination of the forearm, extension of the wrist, and global and distal grasp). Each week, 12 tasks were programmed (six tasks for each hour). A glove glued on a cardboard base to prevent grasp and possible mirror movements was employed as a method of partial containment for the unaffected hand and was manufactured by each family according to the child’s interest (Figure 1).

Partial unaffected hand containment.
For the BIT-mCI program, each hand received a different role in the designed bimanual activities, beginning with the use of the affected hand as the assisting hand during the first 4 weeks and then changing to act as the operating hand in the last 4 weeks. For the 2 weeks of BIT in the mCIMT-B program, the affected hand was given the assisting role for the first week, and then the operating role for the second week. Some examples of activities for both therapies are shown in Table 1 and Figure 2.
Example of activities from the CIMT and BIT part of therapies in both protocols (mCIMT-B and BIT-mCI).

BIT, bimanual intensive therapy; mCIMT, modified constraint induced movement therapy.

Both pictures show a child with right USCP. The first picture shows a mCIMT activity: the child must throw the small ball with the affected hand (right) while the unaffected hand is contained (left hand). The second picture observes the child performing a BIT activity: the child must assemble and disassemble Lego bricks using both hands, where the affected hand has the operating role, and the unaffected hand is assisting.
When the treatment started, a weekly follow up was used to avoid any complications and increase treatment adherence. The families were requested to fill in a registration sheet with the execution time of each activity, the different activities that the child performed in the first and second hour, the time that the activity lasted and the child’s behaviour towards it. This registration sheet would be used to check the adherence to intervention. The follow up with the families was conducted online, reviewing all activities and modifying them if necessary in order to improve the child’s performance. The change of activities was made when practicing the activities (which were programmed according to the interests) in the online follow up, a great effort was observed in the execution, meaning that the child had to make great compensations, and even got frustrated, in which case they switched to easier activities to get it done. Families had the possibility of contacting the referral physiotherapist via email or telephone, at any time, to solve any doubt or urgent complication that would condition the execution of the therapy. The therapeutic goal of these on-line follow-up sessions was always to avoid the frustration of the child, the insecurity of the parents and to introduce satisfaction and children–parents–therapist feedback.
Outcome measures
Affected upper limb functionality
The affected upper limb functionality was divided into bimanual functional performance and experience of use of the affected upper limb in the ICF activity domain. 53
The bimanual functional performance of the affected upper limb was measured with the AHA v. 5.0 scale, 54 which has been validated previously for children aged between 18 months and 12 years with UCP and obstetric brachial palsy.54,55 The AHA v. 5.0 (school kids) is a valid and reliable tool that includes 20 items, each scoring from 1 (total lack of use) to 4 (effective use).54–56 The play session was recorded on video and later scored by a trained evaluator blinded to the group allocation. The Rasch model provides measures of equal intervals in logits (log odds probability units) by converting ordinal rating scale observations to interval levels. In order to facilitate the interpretation of results, the logit scale is converted to a user-friendly 0–100 scale that is still Rasch-based and presents interval level data (namely, AHA units). 54 In addition, a clinically meaningful change is obtained with 5 AHA units of difference pre–post treatment scores.54–57
The AHA in the five assessment timepoint was conducted by a member of research group who had been training and was official certificated in the AHA scale use. The scores were given by a blind external rater certificated in the same scale and the assessment timepoint was blinded to be assessed by the blind external rater.
The affected upper limb-use experience was assessed by the Children’s Hand-use Experience Questionnaire (CHEQ), 58 validated for children with unilateral affectation or disuse of one of their upper limbs in the age range of 6–18 years, in which the experience of children using the affected hand in 29 different bimanual activities of daily living is assessed. 59 Criteria of the CHEQ include whether the child used grasp or support when using the affected hand, the effectiveness of the affected upper limb use, the time to perform the activity compared with a child of the same age with typical development and if there was some discomfort when performing the activities of the questionnaire. These concepts were assessed on a score scale of 1–4, with 1 point representing least effective and 4 points corresponding to most effective. 58 CHEQ scales are rated on a four-point ordinal scale and raw scores: higher scores indicate a better grasp, less time taken and greater satisfaction. Previous investigations have shown acceptable unidimensional and high test-retest reliability (ICC 0.87–0.91) in children with UCP; the results indicate a possible ability to detect change. 59 The CHEQ was performed online (cheq.se) and the reports were sent to the evaluator.
Therapy satisfaction and expectations from parents
Parents must complete a questionnaire about their expectations before executing the therapy, based on an article on home-based bimanual intensive therapy, 25 and another questionnaire after completing 100 h of therapy, collecting information on satisfaction in the execution of the protocol. Both questionnaires consist of five questions, and each question has five possible answers depending on the question asked (see Appendix A: Table A1).
Data collection
Data were collected over five assessment timepoints for 10 weeks. The first assessment timepoint was focussed on obtaining data before treatment, that is, in week 0 (baseline situation, immediately before starting treatment), and in week 4 (after 40 h of mCIMT or BIT) and week 8 (after 80 h of mCIMT or BIT) (first part of the protocol), whereas the last assessment timepoint was conducted at the end of the treatment, that is, in week 10 (a total dose of 100 h). The satisfaction and expectations questionnaire data were collected in two assessment timepoints: week 0 and week 10. There was a post-treatment follow up at week 34. The assessment timepoints are shown in Figure 3.

Assessment timepoints performed in the study period for both intervention groups.
Sample size
According to CONSORT guidelines,60,61 the sample size estimates were based on the primary outcome measure, the AHA. The AHA scale’s responsiveness to change has been shown in a study by Eliasson et al. 62 Calculation by a statistician indicated that, for a 1.33 effect size at significant level of 0.05 and 80% power, a minimum sample size of 10 per group is required in the present study.
Statistical analysis
Statistical analysis of the data was performed using SPSS v20.0 for Windows (SPSS Inc., Chicago, IL, USA). Given the non-normality of the sample, non-parametric analyses were used with the Mann–Whitney U test to determine inter-group differences for the variables. Fisher’s exact test was used to determine inter-group differences according to sex and affected upper limb side. Firstly, the Friedman test was used to evaluate the existence of statistical significance for the assessments performed at different time points in each variable. Subsequently, a Wilcoxon pair test was performed on the variables that presented statistical significance, in order to observe statistically significant differences between pairwise comparisons, and post hoc Bonferroni test was used to reduce the bias. The qualitative variable of family satisfaction was converted to a quantitative variable, graduating it in five levels, from one (worst behaviour or expectation/satisfaction) to five (best behaviour or expectation/satisfaction). The results are shown as the median and interquartile range (IQR) with a confidence interval (CI) of 95%. All those values with p value <0.05 were considered statistically significant.
Results
Participants
A flow chart of participants of this study is shown in Figure 4. A total of 32 participants were recruited, of whom 10 (31.3%) were excluded for not meeting the inclusion criteria, thus 22 (68.8%) were potentially eligible for the study. Eventually two families (6.3%) decided not to participate. The remaining 20 (62.5%) participants met the inclusion criteria established and were allocated randomly to either of the two intervention groups: 10 children were included in the mCIMT-B group and the other 10 children in the BIT-mCI group. Once assigned to the intervention groups, three participants from the mCIMT-B group were excluded from the study before starting it because they received botulinum toxin infiltration and, therefore, no longer met the inclusion criteria.

Flow chart (consort style). Randomisation, allocation, follow up and analysis of the sample for both intervention groups.
Descriptive characteristics of the participants are shown in Table 2. Regarding demographic data, 47.10% of the participants were males and the other 52.90% were females. Of the entire sample, 52.90% had left USCP and the remaining 47.10% corresponded to right side affectation. The 64.71% were classified as MACS level II. All the children had USCP due to perinatal stroke. Participants were between 6 and 8 years old, with a median of 7.12 (0.70) years old. There were no statistically significant differences between groups for age (p = 0.81), sex (p = 0.73) or affected upper limb side (p = 0.79).
Baseline descriptive characteristics of the participants. Values are expressed as n (%) for categorical variables and mean (SD) for non-categorical variables. mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT.

Statistically significant inter-group differences when at p < 0.05.
BIT, bimanual intensive therapy; GMFCS, Gross Motor Function Classification System (levels I–V); MACS, Manual Ability Classification System (levels I–V); mCIMT, modified constraint induced movement therapy; SD standard deviation.
Regarding the dosage applied in each intervention group, participants in the mCIMT-B performed a mean of 76 h mCIMT/18 h BIT, with 77 h BIT-mCI/17 h in the BIT-mCI group. Participation was 94% in the mCIMT-B and 94% in the BIT-mCI (within the expected dose/amount of 90–95% taking as a reference the study by Ferre et al. 25 ). There was no follow-up dropout for any participant who finished the training. All parents from both groups understood and completed the weekly follow up.
Affected upper limb functionality
For bimanual functional performance (measured with AHA scale), there were no statistically significant inter-group differences (mCIMT-B and BIT-mCI) for the baseline situation (week 0) and measurements at different time points (week 4, 8, 10 and 34) (Table 3). Furthermore, there were no significant intra-group changes for the pairwise comparisons over time (p > 0.05). For the affected upper limb-use experience (measured with CHEQ questionnaire), no statistically significant inter-group differences were found for any of the variables. In the intragroup analysis, there were no statistically significant differences for the ‘Needs help’ and ‘Non- use of the affected hand’ variables (Table 4). There were statistically significant differences in the BIT-mCI group for pairwise comparisons week 0–week 10 and week 4–week 10 for use of the affected hand (p = 0.028) and the use of the affected hand to grasp between week 4–week 8 (p = 0.028) and statistically significant differences were not obtained in the mCIMT-B group (Table 5).
Bimanual functional performance measures using the AHA. mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT. Week 0 (before treatment), week 4 (40 h of treatment), week 8 (80 h of treatment), week 10 (100 h of treatment), week 34 (follow up). Values are expressed in AHA units (0–100) as median (IQR).

Statistically significant inter-group differences when at p < 0.05.
AHA, assisting hand assessment; BIT, bimanual intensive therapy; IQR, interquartile range; mCIMT, modified constraint induced movement therapy.
Affected upper limb-use experience: needs help and non-use AH variables, measured through the CHEQ in the mCIMT-B and BIT-mCI groups. Needs help and Non-use AH, are expressed in total number of tasks. Week 0 (before treatment), week 4 (40 h of treatment), week 8 (80 h of treatment), week 10 (100 h of treatment), week 34 (follow up). Values are expressed as median (IQR). mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT.
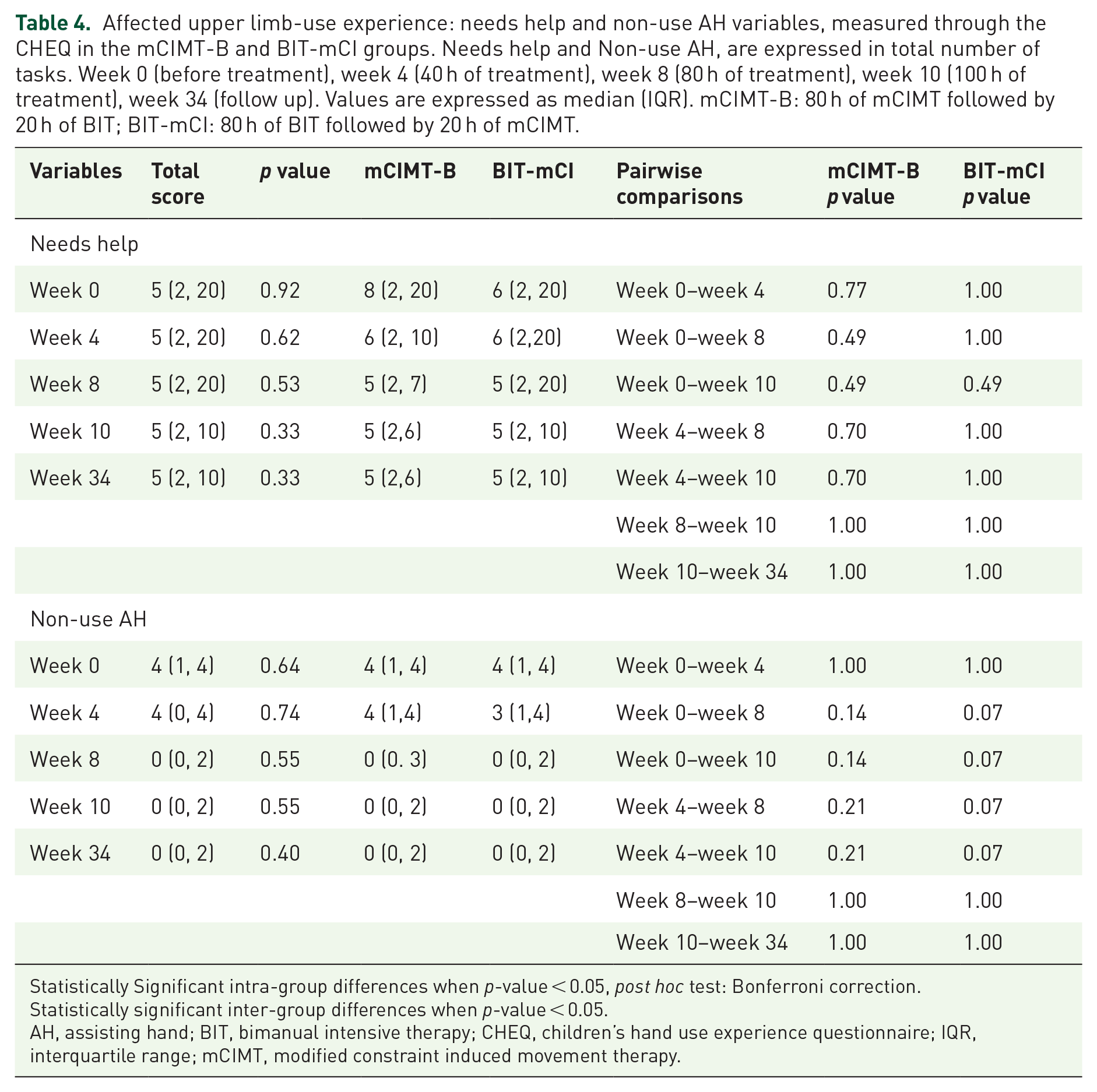
Statistically Significant intra-group differences when p-value < 0.05, post hoc test: Bonferroni correction.
Statistically significant inter-group differences when p-value < 0.05.
AH, assisting hand; BIT, bimanual intensive therapy; CHEQ, children’s hand use experience questionnaire; IQR, interquartile range; mCIMT, modified constraint induced movement therapy.
Affected upper limb-use experience: use of the AH and use of the AH to grasp variables, measured through the CHEQ in the mCIMT-B and BIT-mCI groups. Use AH and Use AH-grasp, are expressed in total number of tasks. Week 0 (before treatment), week 4 (40 h of treatment), week 8 (80 h of treatment), week 10 (100 h of treatment), week 34 (follow-up). Values are expressed as median (IQR). mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT.

Statistically significant intra-group differences when p-value < 0.05, post hoc test: Bonferroni correction.
Statistically significant inter-group differences when p-value < 0.05.
AH, assisting hand; BIT, bimanual intensive therapy; CHEQ, children’s hand use experience questionnaire; IQR, interquartile range; mCIMT, modified constraint induced movement therapy.
Grasp efficacy and discomfort acquired statistically significant differences only in the BIT-mCI group for pairwise comparisons week 0–week 10 and week 4–week 10 (p = 0.035), although task execution time compared with a typically developing child of the same age obtained statistically significant differences only in the group mCIMT-B for pairwise comparisons week 0–week 8, week 0–week 10, week 4–week 8 and week 4–week 10 with p value ⩽ 0.04 (Table 6).
Affected upper limb-use experience: grasp efficacy, task execution time and discomfort variables, measured through the CHEQ in the mCIMT-B and BIT-mCI groups. Efficacy, task time and discomfort are expressed on a scale of 1–4 (1: lowest, 4: highest). Week 0 (before treatment), week 4 (40 h of treatment), week 8 (80 h of treatment), week 10 (100 h of treatment), week 34 (follow up). Values are expressed as median (IQR). mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT.

Statistically significant intra-group differences when p-value < 0.05, post hoc test: Bonferroni correction.
Statistically significant inter-group differences when p-value < 0.05.
AH, assisting hand; BIT, bimanual intensive therapy; CHEQ, children’s hand use experience questionnaire; IQR, interquartile range; mCIMT, modified constraint induced movement therapy.
Therapy’s satisfaction and expectations from parents
In the parent’s questionnaire, intervention tolerance-child, intervention tolerance-family and intervention repeat-feeling showed statistically significant inter-group differences before intervention. There were statistically significant intragroup differences (p ⩽ 0.02) between week 0 and week 10 in all questions for both groups (Table 7).
Family expectations and satisfaction in both intervention groups. Week 0 (before treatment), week 10 (100 h of combined treatment). Values are expressed as median (IQR). mCIMT-B: 80 h of mCIMT followed by 20 h of BIT; BIT-mCI: 80 h of BIT followed by 20 h of mCIMT.
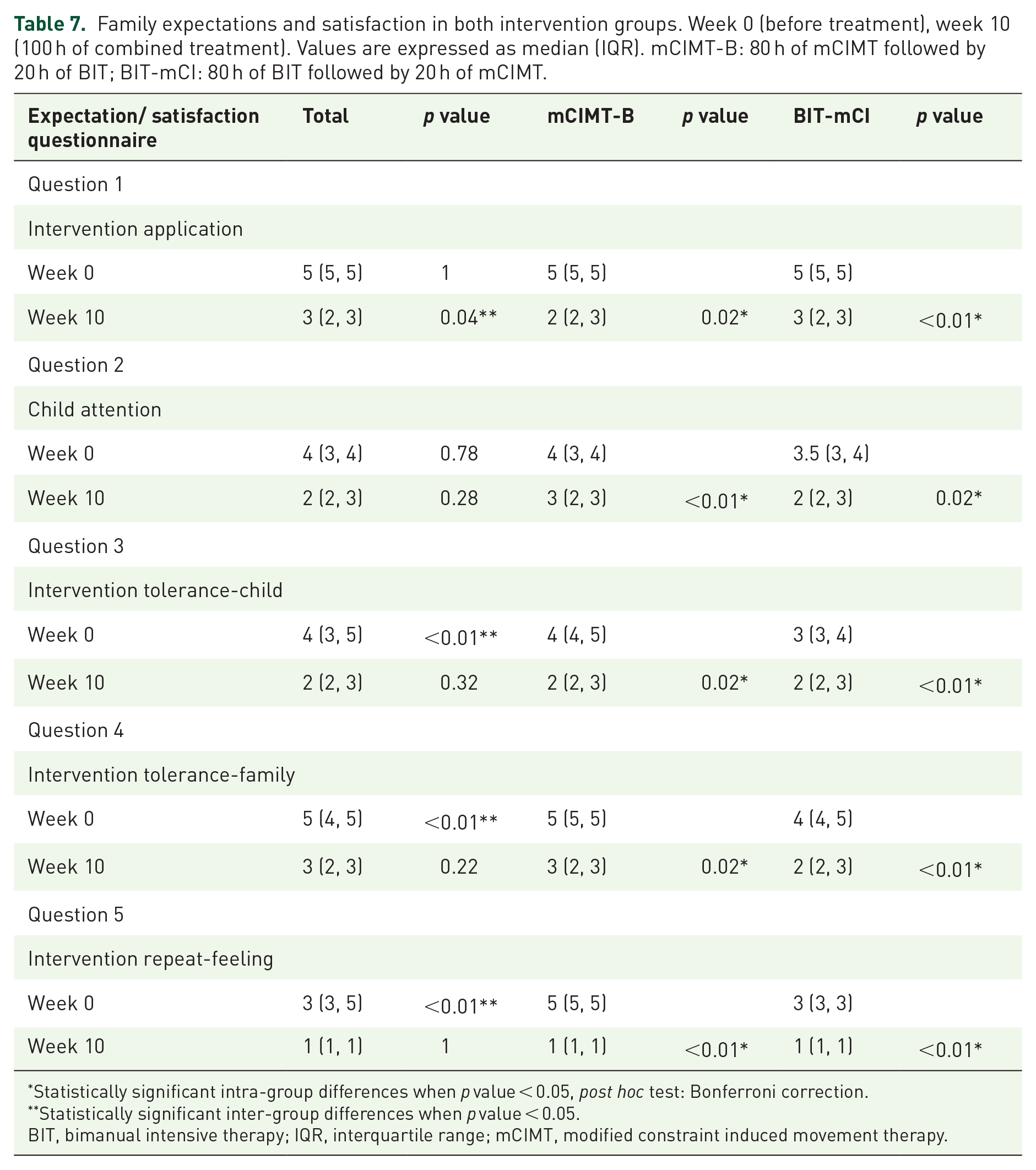
Statistically significant intra-group differences when p value < 0.05, post hoc test: Bonferroni correction.
Statistically significant inter-group differences when p value < 0.05.
BIT, bimanual intensive therapy; IQR, interquartile range; mCIMT, modified constraint induced movement therapy.
Discussion
The implementation of combined intensive therapies at home was possible due to families and children having a high involvement in the treatment and there was no follow-up drop-out. A study by Aarts et al. enrolled the targeted number of children with CP and reported not a single drop-out in the experimental group. 44 The authors noticed the treatment being attractive to children as a major strength. 44 Other facilitators of home-based programmes is the parents’ opportunity to adjust the training moments to their family routine and interests. If families succeed in performing relevant activities in a meaningful setting and at a convenient time, practice may not feel like therapy.63,64 The execution of previous training for therapy at home, deciding on the activities and times of the day to do them, as well as the weekly follow up, favour the family’s adherence to the intervention. 30 These programmes allow families to stay at home and not to travel to the therapy centre several times a week, arranging childcare for siblings, and requiring the child to be absent from school.65,66 As a barrier, these home-based programmes may be stress inductors for parents. 67 Parents may experience pressure to comply, especially when the program is demanding, alteration of parent–child interaction during training with the role of parent changing to that of a therapy provider. This may cause a conflict between their parenting style and their approach as a therapy provider. 67 Interventions in the centre may offer the family the opportunity to interact with other families, have social interactions and not to feel in the role of the therapist. Some parents prefer to limit themselves to their parenting role, instead of being a co-therapist. 67 They consider the home to be a safe environment for the child to unwind, wanting to be there for their child and to provide stimulation, but without forcing the child to practice activities. 68 The intention of parents to avoid emphasising the disability at home, in order to normalise the child’s condition, could be mentioned as a reason to decline home-based training. Parents may need guidance in stimulating and guiding their child in a playful way at home.68,69 In addition, the interventions should include motivation sessions for children and parents. Alternating therapy periods at the centre and at home might be performed in parents’ situations in which their involvement is not possible. To obtain the intervention goals, the level of participation should go along with the wishes of the family.
Regarding the bimanual functional performance measured with AHA scale, non-clinically relevant changes (considered 5 AHA units) 57 occurred at 80 h after the first intensive intervention (mCIMT/BIT) for both groups, but the application of BIT showed a greater increase than with mCIMT and closer to clinical changes (4 AHA units), maintaining stable values at week 10 and at follow up at week 34. Perhaps, the application of more than 80 h of BIT only, or in a combined protocol (BIT-mCI), could have shown significant and clinical changes in AHA scale as has occurred in other studies that applied and compared mCIMT and BIT.33,49 These studies obtained similar improvements for both mCIMT and BIT,33,49 possibly related to the dose application and the baseline situation of lower bimanual functional performance than in our study. When the 80 h of hybrid-CIMT (80 h mCIMT and 20 h BIT) are compared with the 80 h of BIT in the study by Deppe et al., 45 increases are obtained in the AHA scale for both protocols, being greater in the hybrid group because bimanual functional performance was lower, so that the baseline situation could be a conditioning factor in choosing a specific treatment. In our study, after 80 h of both therapies, there were no significant changes, so the combined execution of 20 h of dosage of another therapy (BIT or mCIMT) in children with high bimanual performance (score from 77 on the AHA scale) would not be necessary.
When the affected upper limb-use experience was assessed, participants with high bimanual functional performance had shown great use of the affected upper limb before treatment, with the use of grasping in 13 activities out of 17 performed independently. The goals set in both groups with the families were the same: more functional grasp in the activity of brushing the teeth and peeling an orange. Greater increases were obtained in use of the affected hand, grasp use and grasp efficacy within 80 h of BIT into the BIT-mCI protocol, and were not observed in execution of the mCIMT-B protocol. This translates into improvements within body function and activity domains of the ICF for the BIT-mCI group and only within activity for the mCIMT-B group by reducing the execution time of the bimanual task. This could suggest that the practice of bimanual functional activities in children with high functional performance would favour the acquisition of the proposed goals in the BIT-mCI group.
Similarities were found in the equilateral evolution of the efficacy of grasp in the affected hand and the discomfort of task execution in the present study for BIT-mCI group and the study of Cohen-Holzer et al. 70 This suggests that there may be a correlation between these two variables, independently of the dose and order of application of intensive therapies. Thus, the better grasp quality of the affected hand is translated into greater satisfaction in the execution of the bimanual task. However, this is not linked to greater use of the affected upper limb since, despite the increase in its use, children feel discomfort when introducing their affected hand in bimanual activities. 70 This could be a consequence of alterations in motor function and poor motivation for use of the affected hand.59,61 In the mCIMT-B group, changes were obtained, reducing the execution time of the task, since the application of mCIMT reduces reaction time and favours visuomotor coordination through unimanual practice and unaffected hand containment. 71 Thus, the child could develop functional strategies for the execution of activities with better action planning due to repetition of the task. 72
Therefore, the application of 80 h of BIT would be sufficient to obtain results in the affected upper limb-use experience. Thus, the application and the order of application of one intensive therapy or another would not be indistinct because the BIT protocol could offer better benefits in children with high performance. But it would not be the same in children with poor manual ability since, in the study of Eliasson et al., 62 children improved considerably more on the AHA after mCIMT than children with better hand ability. Another study by Sutcliffe et al. concluded that the presence of non-use at baseline predicted improvement of affected upper limb capacity and performance in bimanual tasks after mCIMT in children with USCP. 73 These findings again suggest the influence of the baseline situation of the affected upper limb when making decisions about a correct intensive therapy.
Significant changes were observed in family expectations with both protocols. Regarding intervention repeat-feeling, it should be noted that families of the mCIMT-B group considered, before starting therapy, that they would not want to perform the protocol again because they thought that it would really be very demanding; while families of the BIT-mCI group were not sure if they would perform the intervention again. After completing both protocols, despite the differences at the beginning, families would repeat the same intensive therapy protocols again. This indicates that parents believed the family environment could be broken, generating frustration or stress for the family and child. However, if families are properly trained in the therapy application, with a weekly follow up, where complications can be avoided, addressing the needs of families, the high adherence and satisfaction rates and reduced stress levels can be explained.74,75
Due to the findings obtained, for children with USCP who have already achieved high/very high functioning, who have an extensive use of their affected upper limb it would not be necessary to apply combined intensive therapies. But it could be positive to use an 80-h protocol of BIT to encourage the use of the affected hand and the hand’s grasp and to improve grasp efficacy within bimanual activities. The combination of bimanual therapy with other types of selective therapies could be beneficial, focussed on robotics or mirror therapy to improve the quality and behaviour of use of the affected upper limb into bimanual tasks.76–79
The main limitations of this study were the lack of standardised descriptions of family characteristics. It is very likely that successful completion of the program is determined by interactions between characteristics of the family with child characteristics such as age, severity, distractibility, etc. The recording of parental stress or situations of frustration of the family and the child during therapy and in different day-to-day situations could be useful to improve their perspectives and the application of therapy, optimising their motivation and adherence to the protocol. It is unknown if the increases on the AHA would have been obtained using a clinical setting and more therapist involvement or with the use of a mixed protocol combining the clinical and home environments. Another limitation was the small sample size (the findings and conclusions cannot be generalised), the absence of a control group and the lack of measures of movement quality variables and manual dexterity, because the sample had high bimanual functional performance that would indicate that children would have achieved great quantity of use and ability in their affected upper limb. Therefore, these intensive therapies with or without combination would not be essential to increase bimanual functional performance. For this reason, this would suggest that the AHA baseline situation on bimanual functional performance is a possible factor to consider when implementing use of intensive and combined intervention protocols to increase bimanual functional performance in children USCP with an AHA score lower than 77.20,40–44,59
Regarding the strengths of the present study, we highlight the high participation and family adherence to the intervention at home, due to the family training and follow up, the importance for therapists of knowing baseline bimanual functional performance before making a treatment decision and not choosing a therapy based exclusively on the child’s diagnosis.
Conclusions
Applying 80 h of BIT for 8 weeks in children with high bimanual functional performance USCP (6–8 years old), executed at home with family involvement would be sufficient to obtain improvements in the experience of use of the affected upper limb, without the need to use combined protocols of 100 h. However, no statistically significant increase in bimanual functional performance would be obtained, and the basal situation of the child is a factor to consider for the execution mCIMT and BIT.
Supplemental Material
sj-htm-1-taj-10.1177_20406223211034996 – Supplemental material for Combined intensive therapies at home in spastic unilateral cerebral palsy with high bimanual functional performance. What do they offer? A comparative randomised clinical trial
Supplemental material, sj-htm-1-taj-10.1177_20406223211034996 for Combined intensive therapies at home in spastic unilateral cerebral palsy with high bimanual functional performance. What do they offer? A comparative randomised clinical trial by Rocío Palomo-Carrión, Cristina Lirio-Romero, Asunción Ferri-Morales, Patricia Jovellar-Isiegas, María-Dolores Cortés-Vega and Helena Romay-Barrero in Therapeutic Advances in Chronic Disease
Footnotes
Author contributions
R.P.C. conceived the study, participated in its design and coordination, collected the data, supported the data analysis, interpreted the data and wrote the article. C.L.R. provided interventions, interpreted the data and wrote the article. P.J.I. provided interventions and interpreted the data. H.R.B. participated in its design and coordination, supported the data analysis, interpreted the data and wrote the article. A.F.M. supported the data analysis and interpretation. M.D.C.V. supported the data analysis and interpretation. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.