
Abstract
Aims:
In response to the rapid spread of COVID-19, this paper provides health professionals with better accessibility to available evidence, summarising findings from a systematic overview of systematic reviews of the neurological symptoms seen in patients with COVID-19. Implications of so-called ‘Long Covid’ on neurological services and primary care and similarities with other neurological disorders are discussed.
Methods:
Firstly, a systematic overview of current reviews of neurological symptoms of COVID-19 was conducted. Secondly, the implications of these findings are discussed in relation to the potential effect on neurological services and the similarities in the experience of patients with COVID-19 and those with other neurological disorders. A total of 45 systematic reviews were identified within seven databases, published between 11 April 2020 and 15 October 2020, following a search in June 2020, updated on 20 October 2020.
Results:
The results indicated that COVID-19 exhibits two types of neurological symptoms; life-threatening symptoms such as Guillain–Barre Syndrome (GBS) and encephalitis, and less devastating symptoms such as fatigue and myalgia. Many of these so-called lesser symptoms appear to be emerging as longer-term for some sufferers and have been recently labelled Long Covid. When compared, these less devastating symptoms are very similar to other neurological conditions such as chronic fatigue syndrome (CFS) and functional neurological disorder (FND).
Conclusion:
Implications for neurological healthcare services in the United Kingdom (UK) may include longer waiting times and a need for more resources (including more qualified health professionals). There is also a possible change-effect on health professionals’ perceptions of other neurological conditions such as CFS and FND. Future research is recommended to explore changes in health professionals’ perceptions of neurological symptoms because of COVID-19.
Keywords
Introduction
As of 29 October 2020, over 44 million people worldwide have been affected by the novel coronavirus disease COVID-19. 1 COVID-19 has been found to cause neurological manifestations in up to 50% of patients. 2 Several systematic reviews have been conducted into the neurological symptoms of COVID-19. However, some reviews focussed purely on specific types of symptoms such as olfactory symptoms, whilst others focussed on studies only in specific countries; for example, a quarter of the studies within the reviews were undertaken in China. It was therefore deemed necessary firstly to conduct a systematic overview of previously conducted systematic reviews to summarise the neurological symptoms of COVID-19 seen so far.
Secondly, it is becoming clear that COVID-19 affects many patients neurologically and, in some cases, symptoms are persisting. A recent British Medical Journal (BMJ) webinar discussed the emergence of so-called ‘Long Covid’.3,4 This paper further discusses the concerns about the short- and long-term effects of COVID-19 on medical and holistic neurological practice, and where future resources will be required.
Thirdly, as COVID-19 is a new disease, the potential similarities with other neurological conditions have not yet been explored in the literature. The authors of this paper identified that many of the neurological symptoms of COVID-19 appear similar to the symptoms of functional neurological disorder (FND). In addition, the BMJ webinar and recent articles discussed the similarities between so-called ‘Long Covid’ and chronic fatigue syndrome (CFS), as it has become increasingly noticeable that symptoms are similar.4,5 Whilst FND is generally regarded as a psychological disorder, the authors of this paper argue that the emerging discussions about supporting patients with Long Covid should relate to other neurological disorders such as FND and CFS,6,7 questioning how these conditions are judged and how treatments are resourced for them as well as for Long Covid.
Neurological services in the United Kingdom (UK) offer diagnosis and treatment to patients with disorders of the nervous system. 8 This research is therefore aimed at health professionals and commissioners in the field of neurology and in primary care in the UK. It aims to inform future service provision for those who develop long-term neurological symptoms due to COVID-19, as well as exploring the effect of COVID-19 on health professionals’ perceptions towards those with symptoms of FND.
Methods
A systematic overview of current systematic reviews was conducted to explore the potential impact of the longer-term neurological symptoms of COVID-19. The review protocol was not registered previously to avoid delay in researching and publishing findings related to COVID-19, particularly as the subject is of immediate concern. The implications of the findings of this overview were discussed, including potential effects on neurological and primary care services and on perceptions towards patients with other neurological disorders such as CFS and FND.
To conduct the systematic overview of systematic reviews, the recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement were followed (Figure 1). 9 Following these recommendations reduces the risk of bias or selective reporting and demonstrates transparency in the process conducted. In June 2020, updated on the 20 October 2020, the following databases were searched, with date limitations between December 2019 and November 2020: ‘PubMed Central’, ‘Cochrane Database of Systematic Reviews,’ ‘Ovid’ ‘ScienceDirect’ ‘Biomed Central’ ‘BMJ’ and SAGE Journals. The following keywords within the title or abstract were used to conduct each search: ‘coronavirus’, ‘COVID-19’, ‘SARS-COV-2’, ‘neurological’, ‘nervous’ and ‘review’. For example, PubMed Central was searched using the following search terms: (((COVID-19 OR SARS-COV-2 OR coronavirus[Title]) OR (COVID-19 OR SARS-COV-2 OR coronavirus[Abstract])) AND ((neuro* OR nervous[Title]) OR (neuro* OR nervous[Abstract])) AND ((review[Title] OR (review[Abstract]))). Limitations: Date: 1 December 2019–1 September 2020. Only systematic reviews published in academic journals in English were retrieved. Reference lists of retrieved systematic reviews were also searched to ensure literature saturation.
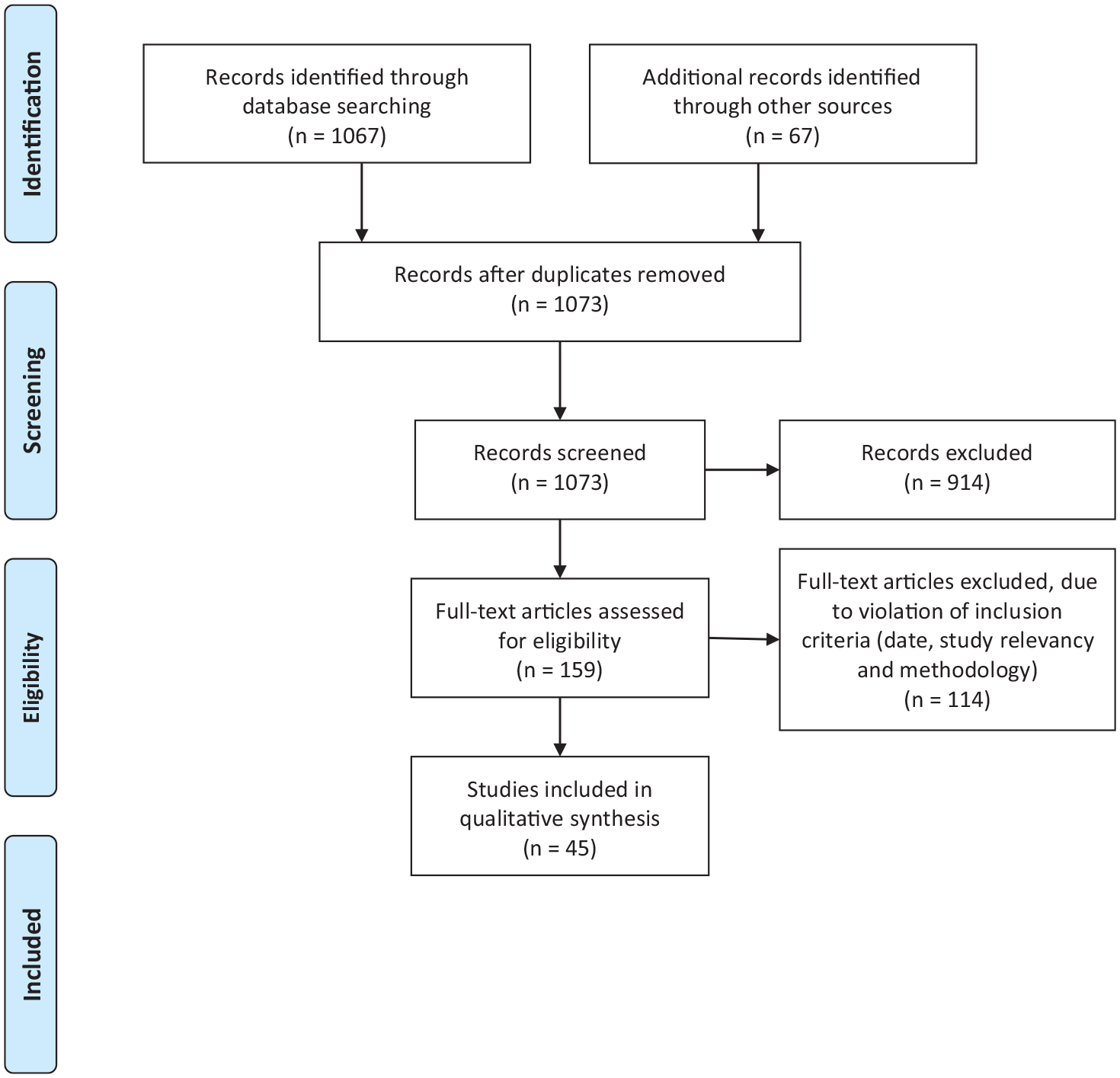
PRISMA flow diagram.
The inclusion criteria consisted of systematic reviews only relating to neurological symptoms seen in patients with COVID-19 since 1 December 2019. Both authors participated through each step of the review independently (screening, eligibility and inclusion). Reviews were screened for relevancy against the inclusion criteria within title and abstract. Full-text reports for all potentially relevant reviews were obtained, including those where there was any uncertainty. The authors screened the full-text reports for relevancy and resolved any disagreement through discussions. Neither of the authors were blind to the journal titles, the authors’ of the reviews or institutions.
The Critical Appraisal Skills Programme (CASP) checklist for systematic reviews (2018) was used to establish the quality of each review included within this systematic overview. 10 CASP does not suggest a scoring system, asking only whether each of the 10 criteria is achieved. However, for clarity the authors of this review included a ‘partly achieved’ option. All included reviews were deemed high quality, as they fulfilled at least 7 of the 10 criteria. The quality evaluation is set out in Table 1 (Supplemental Material 1). From our evaluation, 37 reviews fully achieved 9 of the 10 criteria, 7 reviews fully achieved 8 of the 10 criteria, whilst 1 review fully achieved 7 of the 10 criteria. None of the reviews met criterion eight: their findings could not be applied to a larger population as they explored predominantly specific symptoms of COVID-19 and/or its effects within a specific population.
Quality assessment using CASP criteria. 10

Q1 Did the review address a clearly focused question? Q2 Did the authors look for the right type of papers? Q3 Do you think all the important, relevant studies were included? Q4 Did the review’s authors do enough to assess quality of the included studies? Q5 If the results of the review have been combined, was it reasonable to do so? Q6 What are the overall results of the review? (are they clear?). Q7 How precise are the results? Q8 Can the results be applied to the local population? Q9 Were all important outcomes considered? Q10 Are the benefits worth the harms and costs?
CASP, critical appraisal skills programme; n, no; y, yes.
All reviews were read in full by both authors. Microsoft Excel was used to compile a list of all the included reviews and the neurological symptoms mentioned in each. This list was completed and checked by both authors.
Next, neurological symptoms of COVID-19, CFS and FND were placed into a table to compare the symptoms, which led to a consideration of the implications for neurological healthcare services and primary care in the UK, and to the possible change-effect on perceptions towards CFS and FND.
Results
A systematic overview of systematic reviews of neurological symptoms of COVID-19
PRISMA guidelines were followed for the search strategy of the systematic overview as seen in Figure 1. The database search identified 1067 papers, with a further 67 papers identified within the reference lists of the included reviews; 61 duplicates were removed. From a total of 1073 papers, 914 were excluded after title and abstract review for relevance. The remaining 159 papers were reviewed in full. Of these, 114 were excluded as they did not meet the inclusion criteria (date, study design or methodology). Finally, 45 systematic reviews met the inclusion criteria and were included in this overview.11 –55
The 45 systematic reviews were published between 11 April 2020 and 15 October 2020. The characteristics of the reviews can be seen in Table 2; the number of relevant studies reviewed within each review, the number of participants in each relevant study and the aims of each study. As mentioned, the CASP checklist was utilised to check for risk of bias in each review.
Characteristics of the reviews and number of studies in each country.

Many reviews referenced the same papers, in some cases reviews stated a different number of studies than were referenced within the review, some reviews did not state number of participants, or total number of participants, (number in brackets is total no. of studies/participants where the review included studies not relevant to this review, for example, reviews of symptoms of other coronaviruses, or number stated differed from no. found), when reviews differed in their report of participants numbers within the same study a consensus was assumed.
AIS, acute ischemic stroke; CNS, central nervous system; COVID-19, novel coronavirus disease 2019; GBS, Guillain–Barre syndrome; HCoV, human coronavirus; MERS, Middle East respiratory syndrome; OGD, olfactory and gustatory dysfunction; SARS, severe acute respiratory syndrome.
As can be seen in Table 2, some of the reviews explored issues outside the scope of this review. Within scope of this review, 611 studies relating to neurological symptoms of COVID-19 were reviewed within the 45 reviews. Most of the reviews included the same studies. For instance, Mao et al. was included in 30 reviews. 56 Whilst numbers of participants were not always stated, more than 67,529 participants were included across the 611 studies reviewed.
Table 3 shows how many studies were carried out in each country. A quarter of the studies took place in China (107 studies with at least 27,445 participants). France, Italy, South Korea, Spain, Sweden, UK and the United States (US) also researched more than 2000 participants in each country. This gives an overview of the countries in which neurological symptoms of COVID-19 are under investigation, although it was not determined whether all participants were within the country stated. There may also be publication bias as this review excluded reviews that were not in English.
Number of studies and participants in each country.

Throughout the 611 studies, 18 neurological symptoms were described. These are summarised in Table 4. As can be seen, neurological manifestations of COVID-19 include catastrophic symptoms such as cerebrovascular disease (CVD), encephalitis and Guillain–Barre Syndrome (GBS), which are understandably hugely concerning and have therefore generated intense discussion and research. COVID-19 has also been found to cause symptoms such as fatigue, dizziness, ataxia, dysphagia and headache, which, although more benign, can be disabling if they become chronic.
Neurological symptoms of COVID-19.

These studies specifically looked only at these symptoms.
Including strokes and blood clots thought to cause stroke.
Including confusion.
Including meningitis, encephalopathy.
Including Miller Fisher Syndrome.
Including suicidal ideation, psychosis, anxiety, depression.
Including ataxia, dystonia (specifically sustained upward gaze, dystonic bilateral leg extension, tongue deviation), hypertonia, hypotonia, myalgia, myasthenia gravis, muscle injury, muscle weakness, spasms.
Fatal respiratory failure in sleep.
Including epilepsy.
Including amblyopia.
Including insomnia.
A comparison between the neurological symptoms of COVID-19 and the most common symptoms of FND and CFS
The most common symptoms experienced by people with FND and those with CFS are compared with the neurological symptoms of COVID-19 in Table 5. The symptoms of FND and of CFS were collated from key National Health Service (NHS) sources and DSM-5.57–60 Neurological symptoms of COVID-19 include catastrophic symptoms requiring emergency care such as stroke, brain haemorrhage, encephalitis and GBS. However, 12 other neurological symptoms were shown to be similar in COVID-19 and FND and/or CFS (highlighted in Table 5). In fact, every non-catastrophic symptom of COVID-19, including the much-researched symptom of hyposmia, is also described as a symptom of FND and/or CFS. Furthermore, most of the symptoms of FND and CFS have been experienced by some people with COVID-19 neurological symptoms, particularly those with Long Covid.
Comparison between neurological symptoms in COVID-19, FND and CFS.

Including strokes and blood clots thought to cause strokes.
Including confusion.
Including meningitis.
Including Miller Fisher Syndrome.
Including suicidal ideation, psychosis, anxiety, depression.
Including myalgia, muscle injury, ataxia, spasms, dystonia.
Fatal respiratory failure in sleep.
Including epilepsy.
Including amblyopia.
Including insomnia.
CFS, chronic fatigue syndrome; FND, functional neurological disorder.
Discussion
From these results, this paper argues three main points: (1) COVID-19 appears to be becoming chronic for some patients, presenting similar neurological symptoms to FND and to CFS; (2) the long-term neurological effects of COVID-19 may impact neurological and wider health care services; (3) the neurological symptoms seen in COVID-19 may (and should) affect health professionals’ perceptions of FND and CFS.
Long Covid, FND and CFS present similar neurological symptoms
Long Covid, FND and CFS present similar neurological symptoms; every non-catastrophic symptom of COVID-19 (except for hypogeusia) is described as a symptom of FND and/or CFS. In addition, every symptom of FND (except bladder and bowel issues), and of CFS, (except flu symptoms and heart palpitations) have been experienced by some people with COVID-19. Notably, the main symptoms of Long Covid are increasingly similar to symptoms of CFS (fatigue, inability to concentrate, myalgia, headache). 3
The impact of these findings on neurological healthcare services and primary care
Echoing concerns raised recently by the British Medical Association, 7 the findings of this review highlight the impact that short- and long-term neurological symptoms of COVID-19 may have on current health services. Symptoms seen in Long Covid such as facial pain, muscle issues, neuralgia, fatigue and insomnia, may become long term and disabling, requiring sustained support from healthcare services such as pain-, fatigue- and sleep-clinics, neurological services and primary care. This is supported by other research that suggests rehabilitation required by patients following COVID-19 infection may be ‘very much along the same lines as existing services but with double the demand’. 61 Consultant-led neurological services such as chronic fatigue clinics and headache clinics are already overstretched, with a shortage of neurology consultants and long waiting lists. 62 Neurological symptoms of Long Covid may increase demand for these clinics and may indicate a need for more qualified health professionals and specialists in neurology. The effects of COVID-19 on these services is hard to predict, as the neuropathy, myopathy and sensory deficits of SARS resolved within 3 months of recovery. 46 However, as COVID-19 appears to be becoming Long Covid for up to 10% of patients, 3 support is likely to be required, potentially for a significant number of people, if their symptoms do not resolve spontaneously.
Additionally, COVID-19 is causing a wider impact on patient populations. For example, COVID-19 has affected delivery of health care services, through reduction in use of emergency services during the peak of the pandemic in the UK as patients were worried about contracting the virus from hospitals. 63 There is evidence that some patients with long-term conditions have improved their self-care techniques, such as better use of medication and alternative therapies such as physiotherapy, cognitive behavioural therapy, and exercise. On the other hand, most outpatient appointments and elective surgeries were postponed, leading in some cases to deaths as an indirect result of COVID-19. 64 There are now questions about whether there will be a rebound in demand, potentially overwhelming NHS services, or whether the reduction in demand can be sustained. Combined with the previously mentioned potential increase in demand for neurological services, there are likely to be wide reaching financial implications. This research is therefore useful for aiding future patient management while helping to develop policies for response to COVID-19 and its critical outcomes.
The effect of COVID-19 on perceptions of FND and CFS
Key sources differ in their description of FND symptoms, indicating that there is no comprehensive list of all FND symptoms.57 –60 It is likely that this contributes to health professionals’ uncertainty in diagnosing FND. 65 In addition, patients with both FND and CFS have experienced many years of scepticism from health professionals with negative consequences, 5 including lack of support and poor access to services often contributing to poor mental health. 66 In addition, lower value is given to health professionals’ role in managing poorly defined symptoms. 67 FND and CFS, alongside other ambiguous uncertain conditions (e.g. fibromyalgia), are considered amongst the lowest conditions on the hierarchy of importance of conditions. 68
Conversely, COVID-19 can be diagnosed quickly and easily with a test (leaving aside the possibilities of false results). The authors of this research are concerned that, within neurological services, priority may be given to patients who have had COVID-19, who may actually experience some level of prestige because they have survived a disease feared by all, and any neurological symptoms they experience might be automatically accepted, extensively researched and supported, to the detriment of other neurological conditions. There is already evidence of this skewing of services, as large sums of money and research at pace are contributing to a greater understanding of long-term symptoms of COVID-19, 69 and the NHS has declared its intention to provide a COVID-19 rehabilitation service. 6 Also, there is indication that the presence of Long Covid is unquestionably ‘believed’ by health professionals, as doctors and other professionals have written about their experiences with it and are recommending each other’s papers.3,5
However, some patients with emerging Long Covid have similar experiences to those with less accepted conditions, particularly those who were unable to get a test early in the pandemic. 70 Patients feel doctors dismiss their symptoms, they feel desperate and disagree with diagnoses of anxiety. As Garner (2020) explained: ‘Doctors need to stop diagnosing this as anxiety. We have messed up before, let’s not do it again with long-term covid-19 illness.’ 5
It is important to highlight the similarities between symptoms of Long Covid and other conditions, providing education for health professionals, informing future practice and illustrating the need for more funding for neurological services to meet increased demand. Whilst research and services for COVID-19 are gaining funding, there is a lack of funding and research into understanding, treatment and support for those who suffer from FND and CFS. 71 FND and CFS are likely to have lower prestige than COVID-19; however, the realisation that COVID-19 causes neurological symptoms similar to FND and CFS may lead to a potential shift in perceptions towards these conditions. They may be taken more seriously, and more funding may be made available for appropriate neurological services unrelated to the cause of the symptoms.
Limitations
Scientific reports centred on neurological effects of COVID-19 are still scarce, and risk of publication bias is high. For example, within the reviews included in this research, a quarter of the studies were undertaken in China (148) and a further quarter in Europe (179). Only three studies were conducted in the African continent and nine were conducted in the South American continent. Despite the status of COVID-19 as a pandemic, research into the neurological effects of COVID-19 so far has not been conducted worldwide.
This systematic review is grounding its results on previous reviews’ findings; thus, it is difficult to assess how reliable some of these results can be, for example many of the reviews (156) did not state the source country of their findings. Quality assessment has, however, been undertaken as described earlier and the reviews were deemed high quality. Retrospective and prospective studies of larger cohorts are necessary to correctly assess nervous system involvement, which has not been possible yet for COVID-19 as it is a very new disease and it is unclear how much it mimics other coronavirus diseases.
Conclusion and implications for future research
There is an array of evidence to show that COVID-19 causes neurological symptoms and, although it is difficult to ascertain how long term the symptoms may become, there is increasing evidence of the presence of Long Covid, symptoms persisting beyond 3 months. Although this paper is primarily UK-focussed, these concerns are likely to be similar in other countries. This research collates the evidence so far and provides insight into the neurological effects of COVID-19 in relation to FND symptoms. Concerns about the potential impact of these findings on the delivery of neurological and wider healthcare services are considered alongside the potential effect COVID-19 may have on perceptions of neurological symptoms, particularly those relating to FND and CFS. Further research is recommended to explore whether the neurological symptoms of COVID-19 will improve acceptance and understanding of FND, or whether this will worsen the experience for those who suffer from FND. Further thought for future planning of health care resources also needs to be taken into consideration in light of this pandemic.
Supplemental Material
sj-pdf-1-taj-10.1177_2040622320976979 – Supplemental material for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services
Supplemental material, sj-pdf-1-taj-10.1177_2040622320976979 for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services by Tamar Wildwing and Nicole Holt in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-pdf-2-taj-10.1177_2040622320976979 – Supplemental material for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services
Supplemental material, sj-pdf-2-taj-10.1177_2040622320976979 for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services by Tamar Wildwing and Nicole Holt in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-pdf-3-taj-10.1177_2040622320976979 – Supplemental material for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services
Supplemental material, sj-pdf-3-taj-10.1177_2040622320976979 for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services by Tamar Wildwing and Nicole Holt in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-pdf-4-taj-10.1177_2040622320976979 – Supplemental material for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services
Supplemental material, sj-pdf-4-taj-10.1177_2040622320976979 for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services by Tamar Wildwing and Nicole Holt in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-pdf-5-taj-10.1177_2040622320976979 – Supplemental material for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services
Supplemental material, sj-pdf-5-taj-10.1177_2040622320976979 for The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services by Tamar Wildwing and Nicole Holt in Therapeutic Advances in Chronic Disease
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.