
Abstract
Nonselective β blockers (NSBBs) combined with esophageal variceal ligation (EVL) are recommended for secondary prophylaxis of esophageal variceal bleeding (EVB) in cirrhotic patients according to the current practice guidelines and consensus. However, until now, there is a paucity of recommendations regarding the use of NSBBs in cirrhotic patients who achieved variceal eradication. In this review paper, we firstly introduced a case who achieved variceal eradication after additional use of NSBBs for secondary prophylaxis of EVB and then did not require further endoscopic therapy during repeated endoscopic surveillance, and subsequently discuss the importance of NSBBs for secondary prophylaxis of EVB, the effect of NSBBs after variceal eradication, adherence to NSBBs, screening for variceal recurrence, and timing of endoscopic surveillance after variceal eradication.
Keywords
Introduction
Esophageal variceal bleeding (EVB) is one of the most severe and common complications of portal hypertension in cirrhotic patients. Rebleeding rate is up to 60% in the absence of secondary prophylaxis. 1 Nonselective β blockers (NSBBs) (i.e. propranolol and nadolol), which can antagonize β2 receptors to reduce portal pressure, in combination with esophageal variceal ligation (EVL) are the first-line choice for secondary prophylaxis of EVB according to current guidelines and consensus.2–5 Pharmacological alternatives to NSBBs, such as carvedilol, which has also an intrinsic anti-α1 receptor activity, possibly leading to a greater reduction in portal pressure, and long-acting nitrates, such as isosorbide mononitrate (ISMN), which can further reduce portal pressure, 6 but is used less frequently due to its common side effects (i.e. dizziness and headache) and absence of superiority in decreasing rebleeding and mortality compared with NSBBs therapy alone. 7 Meta-analyses also suggest that a combination of drug and endoscopic therapy significantly decreases the rate of rebleeding and mortality as compared with endoscopic therapy alone (Table 1).7–18
Combination therapy versus endoscopic therapy alone for secondary prophylaxis of esophageal variceal bleeding: an overview of meta-analyses.

EVL, Esophageal variceal bleeding; EVS, esophageal variceal sclerotherapy; NSBBs, nonselective β blockers; ISMN, isosorbide 5-mononitrate; OR, odds ratio; RR, risk ratio; IRR, incidence rate ratio; CI, confidence interval; NA, not available.
Despite such a critical role of NSBBs, there is a serious concern about the safety and tolerance of NSBBs. First, there are many contraindications for NSBBs, for instance, asthma, sinus bradycardia, peripheral vascular diseases, advanced heart failure, cardiogenic shock, and atrioventricular block. Second, some patients adhere poorly to NSBBs, because NSBBs can lead to drug-related side effects, and monitoring of heart rate and blood pressure is necessary during the use of NSBBs. 2 Third, NSBBs may be harmful in cirrhotic patients with spontaneous bacterial peritonitis as well as those with refractory ascites.19,20 Certainly, recent evidence from meta-analyses also suggested that the mortality was not significantly influenced by NSBBs in cirrhotic patients with ascites.21,22 Fourth, the use of NSBBs is also considered as a risk factor for the development of portal vein thrombosis.23,24
Generally, physicians should fully weigh the benefits and potential risks of NSBBs in each individual. If variceal eradication is achieved, some uncertainties remain regarding whether NSBBs should be stopped, as well as when to stop NSBBs. Herein, we reported a cirrhotic patient who developed EVB after initial endoscopic therapy alone, but achieved variceal eradication after additional use of NSBBs for secondary prophylaxis. In this setting, we discussed the importance of the use of NSBBs in secondary prophylaxis of EVB, whether NSBBs should be maintained after variceal eradication, drug adherence during the use of NSBBs, approach of screening for variceal recurrence, and timing of endoscopic surveillance after variceal eradication.
Case presentation
On March 26, 2015, a 60-year-old male (FL) with an 8-year history of hepatitis B virus (HBV)-related liver cirrhosis was admitted to the Emergency Department of our hospital due to hematemesis and melena for 1 day. He did not receive antiviral therapy. The laboratory data are listed in Supplementary Table 1. At that time, he was treated with intravenous infusion of vasoconstrictors, and was subjected to immediate EVL for EVB. After controlling the bleeding episode, he was discharged. Notably, he neither received NSBBs nor underwent regular endoscopic surveillance.
On October 13, 2016, the patient was admitted to the Department of Gastroenterology due to the recurrence of hematemesis. Again, intravenous infusion of vasoconstrictors and EVL were given for the management of variceal bleeding. At that time, NSBBs were not yet prescribed.
On February 14, 2017, he was readmitted to the Department of Gastroenterology due to hematemesis and melena for 2 days. After successful treatment of variceal bleeding by vasoconstrictors and EVL, propranolol was initiated according to the current practice guideline. Additionally, a regular follow-up endoscopic surveillance was recommended.
On April 6, 2017, he underwent follow-up endoscopy without hematemesis or melena. Notably, he adhered to propranolol well. He underwent prophylactic EVL for mild esophageal varices. After discharge, a regular follow-up endoscopic examination every 6 months was recommended.
On November 1, 2017, May 10, 2018, and January 10, 2019, he underwent follow-up endoscopy without hematemesis or melena. He adhered to propranolol. At these admissions, only mild varices were found on endoscopy, and EVL was not recommended by our endoscopist. His heart rate ranged from 57 to 68 beats per minute (bpm) with a blood pressure of 90–150/70–100 mmHg.
On February 24, 2019, a telephone follow up showed that he was well, without any complaints (Figure 1). He took propranolol regularly, and his heart rate was about 60 bpm, and blood pressure was about 140/90 mmHg.

Disease courses of this case receiving NSBBs and EVL.
Discussion
Importance of NSBBs for secondary prophylaxis of EVB
Evidence from 12 meta-analyses comparing the efficacy of NSBBs as add-on therapy with endoscopic therapy for secondary prophylaxis of EVB were systematically reviewed (Table 1).7–18 Among them, 11 meta-analyses defined EVL alone as endoscopic therapy alone group and EVL + NSBBs ± ISMN/sucralfate as combination therapy group,7,8,10–18 but 1 meta-analysis defined either EVL or endoscopic variceal sclerotherapy (EVS) as endoscopic therapy alone group and EVL/EVS + NSBBs ± ISMN/sucralfate as combination therapy group. 9 As for variceal rebleeding evaluated in nine meta-analyses,7,9,10,12,14–18 six meta-analyses showed that combination therapy group significantly decreased the rate of variceal bleeding compared with endoscopic therapy alone group,9,10,12,14,15,18 and three meta-analyses found no statistically significant difference.7,16,17 As for overall rebleeding evaluated in 12 meta-analyses,7–18 10 meta-analyses showed that the combination therapy group significantly decreased the rate of overall rebleeding compared with the endoscopic therapy alone group,8,9,11–18 and two meta-analyses found no statistically significant difference.7,10 As for overall mortality evaluated in 12 meta-analyses, 1 individual patient data meta-analysis showed that combination therapy group significantly decreased the rate of overall mortality compared with endoscopic therapy alone group, especially for Child-Pugh class B/C cirrhotic patients, 17 but 11 conventional meta-analyses found no statistically significant difference.7–16,18 Taken together, the addition of NSBBs on the top of endoscopic therapy seemed beneficial for secondary prophylaxis of EVB in terms of reduction of rebleeding and mortality.
Evidence from eight meta-analyses comparing the efficacy of drug therapy (i.e. NSBBs with or without ISMN) alone versus endoscopic therapy alone for secondary prophylaxis of EVB were systematically reviewed (Table 2).7,9,10,13,18,25–27 Among them, two meta-analyses defined either EVS or EVL as endoscopic therapy alone group and NSBBs ± ISMN as drug therapy alone group,7,9 and six meta-analyses defined EVL as endoscopic therapy alone group and NSBBs ± ISMN as drug therapy alone group.10,13,18,25–27 As for variceal rebleeding evaluated in five meta-analyses,7,9,18,26,27 none of them found statistically significant difference between the two groups. Overall rebleeding was evaluated in eight meta-analyses,7,9,10,13,18,25–27 none of which found a statistically significant difference between the two groups. As for overall mortality evaluated in seven meta-analyses,7,9,10,18,25–27 three meta-analyses showed that drug therapy alone group significantly decreased the rate of overall mortality compared with endoscopic therapy alone group,7,26,27 and four meta-analyses found no statistically significant difference.9,10,18,25 Taken together, the findings from meta-analyses suggested that drug therapy alone was not inferior to endoscopic therapy alone in terms of reduction of variceal rebleeding and overall rebleeding; more importantly, drug therapy alone might be superior to endoscopic therapy alone in terms of survival benefit.
Endoscopic therapy alone versus drug therapy alone for secondary prophylaxis of esophageal variceal bleeding: An overview of meta-analyses.
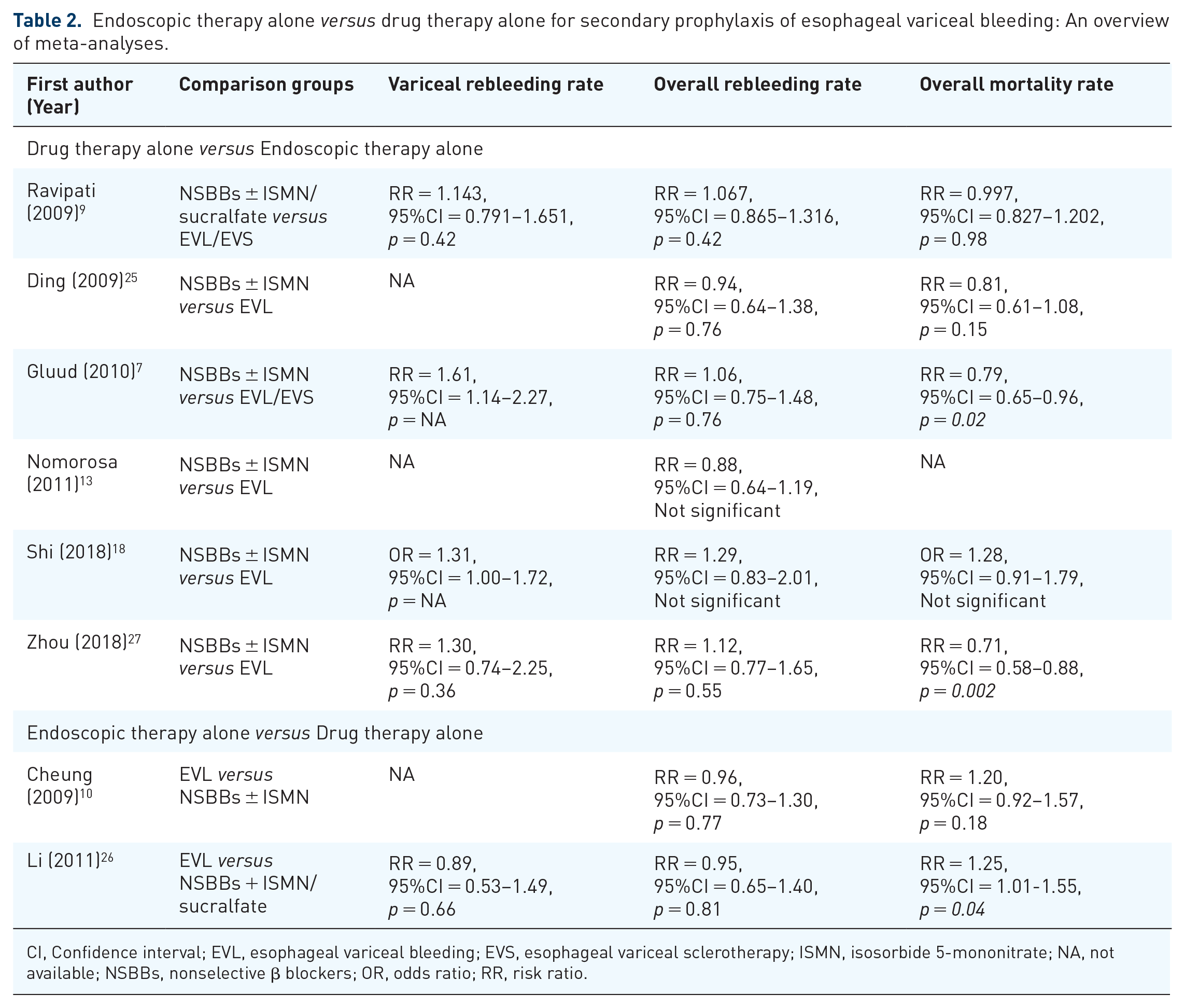
CI, Confidence interval; EVL, esophageal variceal bleeding; EVS, esophageal variceal sclerotherapy; ISMN, isosorbide 5-mononitrate; NA, not available; NSBBs, nonselective β blockers; OR, odds ratio; RR, risk ratio.
Effect of NSBBs after variceal eradication
The recommendations of current guidelines and consensus regarding the use of NSBBs for preventing from no to small varices or from small to large varices under primary prophylaxis are summarized in Table 3.2–5 For patients with high-risk small varices (i.e. red color sign and/or Child-Pugh class C patients), all guidelines consistently recommended the use of NSBBs.2–5 On the contrary, for patients without varices, the use of NSBBs was not recommended.2,4 For patients with small varices but without red color sign, evidence regarding the use of NSBBs was deemed to be lacking.2,4 Several meta-analyses have analyzed the efficacy of NSBBs in the prevention of variceal progression from small to large in patients under primary prophylaxis of EVB (Table 4).28–30 One meta-analysis included patients with no or small varices and found that the incidence of developing large varices was similar between patients treated with placebo and NSBBs. 28 Another two meta-analyses included patients with small varices alone and also achieved a consistent finding.29,30 Besides, it should not be neglected that NSBBs led to more adverse effects and brought no benefit in decreasing the rate of first bleeding and mortality.28,30
Practice guidelines/guidance and consensus recommendations regarding the use of NSBBs in cirrhotic patients with small or no varices.

The quality of evidence and grading of recommendations were ranked according to self-defined system.
The quality of evidence and grading of recommendations were ranked according to Oxford System.
The quality of evidence and grading of recommendations were ranked according to AGREE II tool.
AASLD, American Association for the Study of Liver Diseases; EASL, European Association for the Study of the Liver; LC, liver cirrhosis; NA, not available; NSBBs, nonselective β blockers.
NSBBs versus placebo for prevention of variceal progression in small or no varices: An overview of meta-analyses.

CI, Confidence interval; LC, liver cirrhosis; NA, not available; NSBBs, nonselective β blockers; OR, odds ratio; RR, risk ratio; UGIB, upper-gastrointestinal bleeding; VB, variceal bleeding.
By comparison, our patient also presented with mild varices, but he was under secondary prophylaxis. However, the recommendation regarding the use of NSBBs in such population remains obscure. Regardless, the primary goal of management should be to prevent variceal recurrence after variceal eradication. The evidence was systematically reviewed as follows.
There were seven randomized controlled trials (RCTs) and two cohort studies exploring the rate of esophageal variceal eradication and recurrence in patients receiving NSBBs ± ISMN/sucralfate as add-on therapy to endoscopic therapy (Table 5).31–39 Among them, five RCTs defined EVL + NSBBs ± ISMN as combination therapy group and EVL alone as endoscopic therapy alone group,31–33,36,37 two RCTs and one cohort study defined NSBBs + EVS as combination therapy group and EVS alone as endoscopic therapy alone group,34,38,39 and one cohort study defined EVL/EVS + NSBBs as combination therapy group and EVL/EVS as endoscopic therapy alone group. 35 First, the rate of variceal eradication ranges from 52% to 89% in the combination therapy group and from 40% to 98% in the endoscopic therapy alone group.31–34 Second, the rate of variceal recurrence in patients who achieved variceal eradication was reported to be numerically lower in the combination therapy group than endoscopic therapy alone group, with a range of 14–68% in combination therapy group and 26–97% in the endoscopic therapy alone group (Figure 2).31–39 In order to clarify this issue, we performed meta-analyses of these studies.31–39 Overall meta-analysis demonstrated a significantly lower rate of variceal recurrence in combination therapy group [OR = 0.58, 95% CI (0.36–0.94), p = 0.01] with a potential heterogeneity (I2 = 49%; p = 0.05) (Figure 3). Subgroup meta-analysis of studies comparing EVS + NSBB versus EVS also demonstrated a significantly lower rate of variceal recurrence in combination therapy group [OR = 0.32, 95% CI (0.13–0.77), p = 0.01] with a potential heterogeneity (I2 = 50%; p = 0.14).34,38,39 Subgroup meta-analysis of studies comparing EVL + NSBBs ± ISMN versus EVL suggested a potential trend of EVL + NSBBs ± ISMN over EVL alone in decreasing the risk of variceal recurrence, but the difference was not statistically significant [OR = 0.68, 95% CI (0.40–1.14), p = 0.14].31–33,36,37 Based on the current evidence reviewed and pooled data, the continuation of NSBBs might be preferred after variceal eradication in a ‘secondary prophylaxis’ population.
Combination therapy versus endoscopic therapy alone for variceal eradication and recurrence: An overview of individual studies.

EVB, Esophageal variceal bleeding; EVL, esophageal variceal bleeding; EVS, esophageal variceal sclerotherapy; ISMN, isosorbide 5-mononitrate; LC, liver cirrhosis; NA, not available; PH, portal hypertension; RCT, randomized controlled trial; UGIB, upper gastrointestinal bleeding; VB, variceal bleeding.

Rates of variceal recurrence in patients undergoing endoscopic therapy alone and combined with nonselective β blockers.

Forest plots comparing the rates of variceal recurrence between patients undergoing endoscopic therapy alone and combined with NSBBs.
Adherence to the use of NSBBs
Poor adherence increases both morbidity and mortality. By contrast, an adherence rate of over 80% will improve clinical outcomes. 40 Debernardi Venon and colleagues found that only 62.5% (60/96) of patients took NSBBs after variceal eradication. The use of NSBBs was the only independent predictor associated with a lower risk of variceal recurrence (OR = 2.30). 41 Nonadherence is associated with multiple factors, such as social and economic, healthcare-system-related, therapy-related, condition-related, and patient-related factors. 42 For cirrhotic patients who should receive NSBBs for secondary prophylaxis of EVB, the need for life-long use, the presence of contraindications, drug-related adverse effects, patient intolerance, and modification of dosage by monitoring heart rate and blood pressure may be associated with poor adherence. Dos Santos and colleagues initially prescribed NSBBs for secondary prophylaxis in 43 cirrhotic patients younger than 18 years, of whom only 15 had good adherence; the remaining patients discontinued NSBBs due to contraindications, adverse effects, and for reasons that were unclear. 35 In the study by Pfisterer and colleagues, only 66.2% (319/482) of patients needing secondary prophylaxis were treated with NSBBs and EVL, and the remaining patients (163/482, 33.8%) were treated with EVL monotherapy without NSBBs due to unknown reasons (121/163) and contradictions and intolerance (40/163). 43 Therefore, a good adherence to NSBBs or continuity of NSBBs was potentially useful for preventing variceal recurrence.
Screening for variceal recurrence after variceal eradication
Among patients who achieve variceal eradication, it is important to define a suitable technique and interval to predict and screen for variceal recurrence and rebleeding. Hepatic venous pressure gradient (HVPG) measurement seems to play a critical role in assessing the risk of variceal recurrence and rebleeding as well as in predicting the efficacy of NSBBs. Unfortunately, HVPG measurement in our patient, to identify the effect of NSBBs on portal pressure, was unavailable. Studies suggest that HVPG responders treated with NSBBs have better outcomes; by contrast, HVPG nonresponders have worse outcomes.44–51 Thus, HVPG-guided strategy is preferred to clearly identify candidates for continuing NSBBs. However, it should be noted that not all HVPG responders are free of rebleeding episodes. The rate of rebleeding is 5.6–43% among HVPG responders (Figure 4A). Similarly, not all HVPG nonresponders will develop rebleeding episodes. The rate of free of rebleeding is 12.5–75% among HVPG nonresponders (Figure 4B). Therefore, HVPG is not perfect, and a HVPG reduction does not fully reflect a decline in the risk of rebleeding. Additionally, HVPG measurement is invasive and requires a skilled interventional radiologist or hepatologist. Considering that variceal bleeding and its related morbidity and mortality are hard endpoints, an upper gastrointestinal endoscopic finding showing variceal recurrence or eradication should be more clinically relevant.

Rates of rebleeding and no rebleeding in hepatic venous pressure gradient responders (Upper Panel) and nonresponders (Lower Panel).
Timing of endoscopic surveillance after variceal eradication
The appropriate timing of endoscopic surveillance for cirrhotic patients who have achieved variceal eradication after secondary prophylaxis of EVB remains to be discussed. The first time point of endoscopic surveillance after variceal recurrence should be 3–6 months, 1–3 months, or 3 months according to 2016 American Association for the Study of Liver Diseases (AASLD) practice guidances, 2 2007 AASLD practice guidelines, 52 and 2015 UK guidelines, respectively. 5 Considering these heterogeneous recommendations among the guidelines, a RCT assigned cirrhotic patients under primary or secondary prophylaxis of EVB to 3- and 6-month interval groups to first screen for variceal recurrence; no significant difference was found between the two groups. 41 The next time interval of endoscopic surveillance should be every 6–12 months according to the 2016 AASLD practice guidance and 2007 AASLD practice guideline2,52 or 6 months according to the UK guideline, 5 if there is neither variceal recurrence nor a need for endoscopic therapy. By comparison, relevant recommendations are lacking in the 2018 European Association for the Study of the Liver guideline and Baveno VI consensus (Table 6).3,4
Practice guidelines/guidance and consensus recommendations regarding the endoscopic surveillance in cirrhotic patients after variceal eradication.

The quality of evidence and grading of recommendations were ranked according to AGREE II tool.
The quality of evidence and grading of recommendations were ranked according to the American College of Cardiology and the American Heart Association Practice Guidelines.
AASLD, American Association for the Study of Liver Diseases; EASL, European Association for the Study of the Liver; EGD, esophagogastroduodenoscopy; NA, not available.
Conclusion
The critical role of NSBBs for secondary prophylaxis of EVB has been firmly established. After variceal eradication, the use of NSBBs should be continued for prevention from variceal recurrence and rebleeding. Endoscopic surveillance remains warranted for screening for variceal recurrence and rebleeding. However, its optimal timing needs to be further explored (Figure 5).

A schematic diagram regarding the secondary prophylaxis of esophageal variceal bleeding in cirrhotic patients.
Supplemental Material
Supplementary_table_1_7 – Supplemental material for Use of nonselective β blockers after variceal eradication in cirrhotic patients undergoing secondary prophylaxis of esophageal variceal bleeding: a critical review of current evidence
Supplemental material, Supplementary_table_1_7 for Use of nonselective β blockers after variceal eradication in cirrhotic patients undergoing secondary prophylaxis of esophageal variceal bleeding: a critical review of current evidence by Xiangbo Xu, Xiaozhong Guo, Frank Tacke, Xiaodong Shao and Xingshun Qi in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Authors Xiangbo Xu, Xiaozhong Guo, Frank Tacke contributed equally.
Author contribution
Xiangbo Xu: provided pharmaceutical care of NSBBs for this case, reviewed the literature, and drafted this manuscript.
Xiaozhong Guo: treated this case, participated into the discussion regarding the management of this case, and gave critical comments.
Frank Tacke: gave critical comments and revised the manuscript.
Xiaodong Shao: performed endoscopic examinations and treatment and participated into the discussion regarding the management of this case.
Xingshun Qi: an attending physician for this case, conceived this work, gave critical comments, and revised the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Grant from the Natural Science Foundation of Liaoning Province (no. 201800050) for Xingshun Qi.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.