
Abstract
Infarcted regenerative nodules in a cirrhotic liver is a rare condition that may be confused with hepatocellular carcinoma on imaging. We report here a case of a 58-year-old man with live cirrhosis who presented with abdominal pain and distension and sudden onset of haematemesis. Computed tomography (CT) showed diffuse multinodular infarcted regenerative nodules and gastric bleeding. Physicians should include infarcted regenerative nodules in any differential diagnosis of multiple hepatic lesions in liver cirrhosis, particularly in patients with gastrointestinal varices.
Introduction
Liver cirrhosis is a common disease with many known complications including variceal bleeding, ascites, hepatic encephalopathy, hepatorenal syndrome, hepatopulmonary syndrome, and portopulmonary hypertension. 1 However, infarction of regenerative nodules is a rare condition that is observed mainly in patients who have had a previous episode of gastrointestinal haemorrhage. 2 We report here a case of multiple infarcted regenerative nodules in the liver, spleen and kidney after gastrointestinal haemorrhage.
Case report
A 58-year-old man with a past medical history of alcoholic liver cirrhosis presented to hospital with a 3-day history of abdominal pain and distension. The patient had tested negative for hepatitis B and had a two-year history of atrial fibrillation and diabetes mellitus.
His initial blood pressure was 92/50 mmHg, pulse rate 86 beats/minute, temperature 37.2° and breathing rate 20 times/minute. His physical examination was negative for lymphadenopathy and he did not have liver palms or spider nevi. Breath sounds were normal and his heart rate was 89 beats/minute with arrhythmia. Inspection of his abdomen showed superficial varicose veins, abdominal bulging and subcostal liver and spleen. There was tenderness in the whole abdomen, especially in the right abdomen.
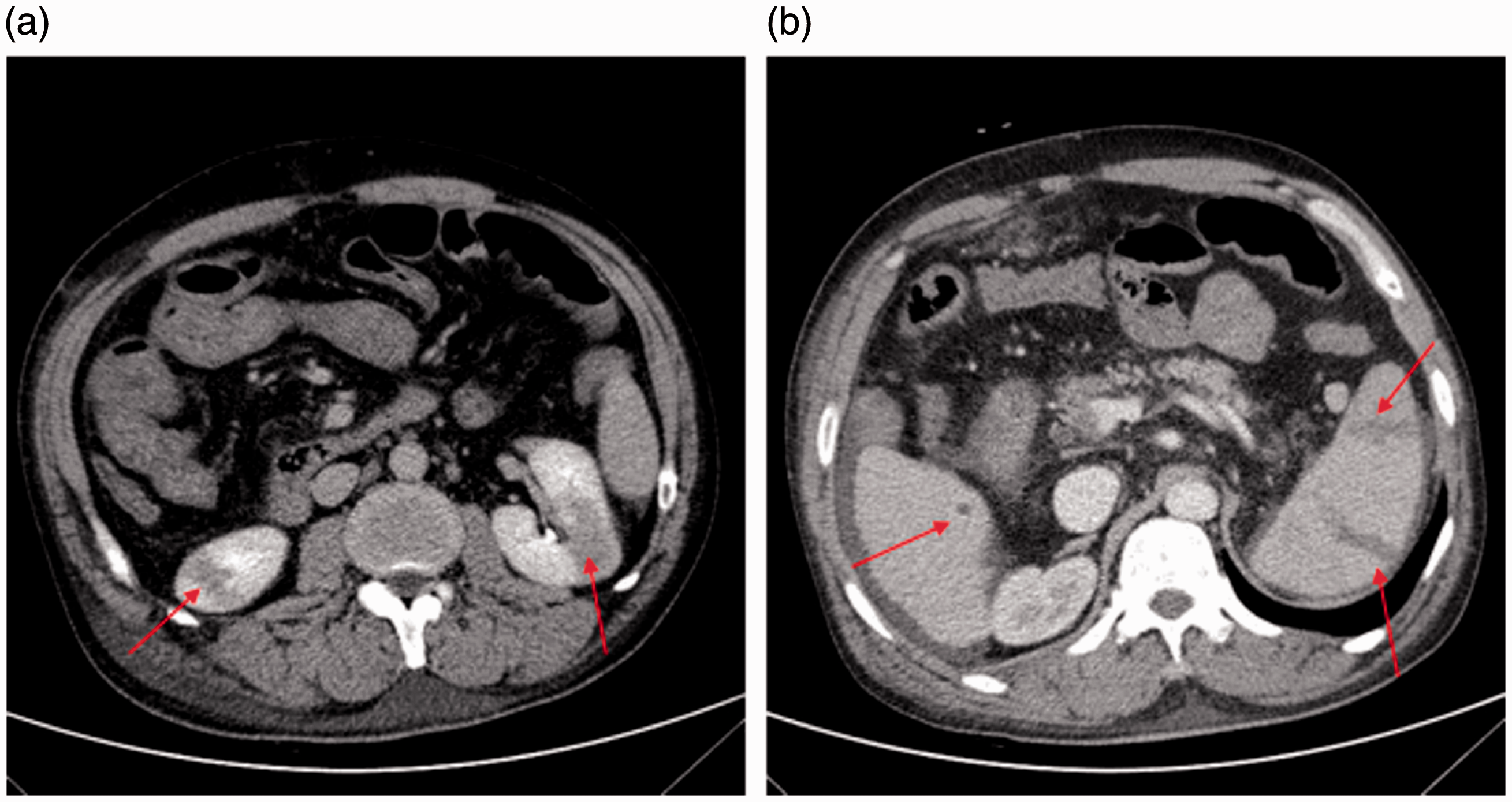
Laboratory tests showed marked anaemia (haemoglobin (Hb) 3.28 g/dl [normal range, 11.5–15.5 g/dl]) and slightly increased serum transaminases (alanine aminotransferase [ALT] 83 U/l [normal range, 3–50 U/l]; glutamic oxaloacetic [GOT] 60 U/l [normal range, 8-40 U/l]). Other test results were as follows: white blood cells (WBCs) 9.3 × 109/l (normal range, 4.0–10.0 × 109/l); neutrophils 7.86 ×109/l (normal range, 1.80–6.40 × 109/l); platelets 93 × 109/l (normal range, 100–300 × 109/l); C-reactive protein (CRP) 65.81mg/l (normal range, 0–3.3 mg/l); lactate dehydrogenase 203 U/l (normal range, 60–245 U/l). Non-contrast computed tomography (CT) of the whole abdomen showed liver cirrhosis, splenomegaly and signs of local abdominal infection (Figure 1a).

(a) Abdominal non-contrast computed tomography (CT) on hospital admission. Liver cirrhosis, splenomegaly and signs of local abdominal infection (blue arrows) without abnormal density of liver, spleen and kidney were observed. (b) Abdominal CT three days later showing multiple low-density lesions with a clear boundary in the liver (red arrows).
On the day of admission, the patient developed a sudden and massive hematemesis of 1000 ml and required aggressive fluid resuscitation and red blood cells to correct the shock. The patient subsequently received sulperazone (2.0 g, intravenously, q8 h), octreotide (0.6 mg intravenously, q12 h), and pantoprazole (40 mg intravenously, q8h).
Three days later, contrast-enhanced CT scans showed multiple intrahepatic low-density lesions and multiple infarctions, abdominal wall and gastric fundus oesophageal varices and perihepatic effusion (Figure 1b and Figure 2). CT scans also showed multiple splenic and bilateral kidney infarctions and partial portal vein thrombosis (Figure 3). The patient underwent gastroscopic oesophageal variceal ligation and following the operation his bleeding improved significantly.

(a) Multiple low-density lesions in the liver without enhancement on contrast-enhanced computed tomography (CT) scan (red arrows). (b) Low-density lesion shown in the liver (red arrow); Arc filling defect and portal vein thrombosis were seen in the portal vein (yellow arrow).
(a) Multiple segmental low-density lesions were seen in the parenchyma of both kidneys, with no obvious space-occupying effect and no enhancement in the focus area in the enhanced computed tomography (CT) scans (red arrows). (b) Multiple low-density fan-shaped and wedge-shaped lesions were seen in the spleen (red arrows). The boundary of the lesions was clearly seen in the portal venous and delayed phases in the enhanced computed tomography (CT) scans.
On the fifth day after admission, laboratory tests were as follows: WBCs 8.7 × 109/l; neutrophils 5.76 × 109/l, Hb 7.2 g/dl, platelets 89 × 109/l; CRP 34.54 mg/L; ALT 136 U/l; GOT 121 U/l; lactate dehydrogenase 313 U/l. After the bleeding had stopped, the patient was transferred to a second hospital for a transvenous intrahepatic portosystemic stent shunt. No further details are available because the patient was lost to follow-up.
Informed written consent was obtained from the patient prior to publication of this report and ethical approval was given by Hangzhou Red Cross Hospital.
Discussion
The liver has a dual vascular supply and there is significant collateralization between the two systems; therefore, blockage of these vessels alone does not commonly cause liver infarction. 3 Indeed, an infarction of regenerative nodules in liver cirrhosis is rare. 2 It has been suggested that regenerative nodules are mainly supplied by portal blood flow and therefore, the cause of the infarction may result from a sudden reduction in portal and arterial blood flow after blood loss or shock induced ischemic necrosis.4–6 Moreover, most patients with infarcted regenerative nodules have experienced previous episodes of gastrointestinal hemorrhage. 2 , 3 , 7 On histological analysis, the lesions are characterized by a central coagulation of necrotic tissues and peripheral granulation tissue containing numerous small vessels. 5
Although rare, the condition is an important abnormality because on CT or magnetic resonance imaging (MRI) the multiple infarcted nodules in a cirrhotic liver may resemble multifocal hypovascular hepatocellular carcinomas, diffuse metastasis or multiple dysplastic nodules.4,8 Therefore, where this condition is suspected, serial imaging or a liver biopsy might be helpful in the differential diagnosis. Furthermore, in a cirrhotic liver, both benign and malignant lesions may lack typical imaging features and so definitive diagnosis may require comparison with previous studies, imaging follow-up, or tissue sampling. 9
Our case report is unique in that this patient with liver cirrhosis and gastric bleeding had multiple infarcted regenerative nodules not only in the liver, but also in the spleen and kidney. The cause of the infarctions in the spleen and kidney may have also resulted from a sudden reduction in blood flow after blood loss or shock.
The purpose of this case report was to highlight that this is an uncommon but important abnormality that can resemble malignant tumours on CT imaging. Importantly, variceal bleeding or septic shock can induce hypotension, which may lead to infarction of the nodules. 7 Physicians should be aware of this condition and add infarcted regenerative nodules to the list of differentials when presented with similar signs and symptoms. Prompt diagnosis may lead to appropriate treatment and a better outcome for the patient.