
Abstract
Background:
The aim of this study was to review available evidence for physical therapy treatment (PTT) after single-event multilevel surgery (SEMLS), and to realize a first step towards an accurate and clinical guideline for developing effective PTT for children with cerebral palsy (CP) after SEMLS.
Methods:
A qualitative systematic review (PubMed, Medline, Embase, CINAHL, and the Cochrane Library) investigating a program of PTT after SEMLS in children aged 4–18 years with CP classified by Gross Motor Function Classification System level I–III.
Results:
Six articles meeting the inclusion criteria were selected. The selected studies provide only incomplete descriptions of interventions, and show no consensus regarding PTT after SEMLS. Neither do they show any consensus on the outcome measures or measuring instruments.
Conclusions:
Based on the results of this literature review in combination with our best practice, we propose a preliminary protocol of PTT after SEMLS.
Keywords
Clinical Messages
There is no evidence to support consensus on a PTT in children with CP after SEMLS.
Clear description of the PTT (goals, frequency, duration, intensity, and method), co-intervention, devices and follow-up are necessary to reach consensus on the therapy that children with CP need after SEMLS.
Introduction
The term cerebral palsy (CP) covers a heterogeneous set of neurodevelopmental disorders caused by brain malformation or damage during early development. The defining characteristics are motor and posture impairment, spasticity, and reduced control, and muscle weakness that limits activities of daily live and self-care. 1 Affecting 2.11 per 1000 children worldwide, CP is the most common cause of physical disability in infancy. 2 CP is usually considered to be caused by a nonprogressive lesion of the developing brain. 3 Yet, the musculoskeletal deformities in the growing child with CP are often progressive. Indeed, as the child grows, the proportions of the musculoskeletal system may change with consequent disproportionate strength and lever arms. These secondary deformities, and a different positioning of the body’s center of gravity, mean that children run the risk of further deterioration in their daily functioning; this significantly reduces the quality of life of those affected children.3,4
Over the last 20 years, single-event multilevel surgery (SEMLS) has become an important treatment option for these secondary deformities in children with CP. 4 SEMLS is defined as two or more soft-tissue or bony surgical procedures at two or more anatomical levels during one operative procedure that requires only one hospital admission and one period of rehabilitation. 4 This medical intervention is used particularly for children walking independently, with or without walking aids, who are progressively threatened in their abilities to stand or walk [Gross Motor Function Classification System (GMFCS II, III)].5,6 The main goal of surgery is to improve stance and gait, both quantitatively and qualitatively, by optimizing the alignment and positioning of the joints in the lower extremities.3,7,8 The most important reasons for children and their parents to choose this extensive surgery are experiences with increasing pain, movement problems, including gait patterns, and fatigue, which interferes with their social relationships in school and everyday life.3,7–9 Dreher and colleagues performed a multicenter cohort study of 231 children after SEMLS, with a follow-up period of 6–12 years. They reported a significant long-term improvement in gait function on the gait profile score. 10 Rehabilitation after SEMLS is very complex and needs to be organized efficiently, and must be part of standard care after SEMLS. The Dutch guideline ‘Diagnosis and treatment of children with spastic cerebral palsy, 2014’ stresses the importance of intensive PTT in the healthcare for children with CP. 3 However, no information about what an effective rehabilitation strategy after a SEMLS procedure entails is presented in the guideline. As stated by McGinley and colleagues, we concluded that ‘there is little information in the available literature to guide clinicians and scientists as to the optimum post SEMLS rehabilitation.’ 4
In their systematic review of the efficacy of SEMLS for children with CP, McGinley and colleagues concluded that meticulous reporting of postoperative rehabilitation after SEMLS is often lacking or inadequate (50% of studies), despite widespread acknowledgment of its importance. 4 Unfortunately, McGinley and colleagues confine themselves to the rather general conclusion that the information these studies provide about duration and frequency of the rehabilitation program is often sparse, without substantiating this conclusion. This is probably because the focus of their review is on the effectiveness of SEMLS in general, not specifically on subsequent physiotherapeutic treatment. After analysis of the studies included in their review, it was concluded that they could have provided more detailed information to guide clinicians towards more substantive physical therapy treatment (PTT) programs. Based on this lack of results, we would like to identify and assess current evidence for PTT after SEMLS.
Our objective is to contribute to the production of an accurate and clinical guideline for developing an effective PTT for children with CP after SEMLS, based on evidence in the scientific literature. The research questions guiding our systematic search are:
(1) What PTT for children with CP after SEMLS has been described in scientific literature?
(2) What outcome measures are used?
(3) What instruments are used to measure the outcome measures?
In order to address our first research question, we utilize the framework of adequate reporting that McGinley and colleagues suggested in terms of which PTT for children needs to be described as a postoperative rehabilitation protocol after SEMLS. 4 This includes duration of the program, type, frequency and duration of physical therapy sessions, and orthotic intervention. McGinley and colleagues advocated the provision of more intervention details in online-only appendices or supplements in cases where results were published. 4
For our second and third research questions, we will not address the effects measured by the different measuring instruments, but will describe what outcome measures have been used by different authors, and what measurement tools were used. We expected the measured outcomes and the associated measuring instruments to match the outcome measures and measuring instruments used for daily, evidence-based practice within the CP population. McGinley and colleagues stated that many studies were underpowered to detect convincing effects of SEMLS intervention. 4
Methods
We applied a systematic review approach to summarize current literature on PTT interventions for CP after SEMLS in children, and to present a protocol for clinical practice based on the existing evidence of the elements of PTT. Prior to commencement of this systematic review, a protocol outline was registered via the PROSPERO register of systematic reviews (CRD 42015020599), and a detailed protocol was submitted for peer review. There were no deviations from the published protocol.
Identification and selection of trials
A search was performed and updated (up to April 2018) in the PubMed, Medline, EMBASE, CINAHL, and Cochrane libraries. The search strategy was developed by one of the authors (EvB). The detailed search string for PubMed is presented in Appendix 1. The terms are divided into four clusters: ‘Cerebral Palsy’, ‘physical therapy’, ‘child,’ and ‘surgery.’ MeSH terms related to the four clusters were used and these terms were connected by Boolean operators. The reference lists of suitable articles were screened manually for missing items. Eligible studies were randomized controlled trials (RCTs), clinically controlled trails, and cohort studies that reported on at least one PTT after SEMLS. Data were extracted for all outcome measures. Only literature in English from the period between 1990 to 1 April 2018 was eligible for inclusion. The directives of the ‘Preferred Reporting Items for Systematic Reviews and Meta-analysis’ (PRISMA) were used. 11
The literature search was carried out by a medical librarian specialist. Records retrieved by the search were assessed for eligibility by two reviewers (EvB, MA) working independently, initially based on titles and abstracts, with potentially eligible articles being assessed in full-text to confirm eligibility. Discrepancies were reviewed and consensus was achieved by discussion, or the decision was completed by consulting a third expert (PJ) in accordance with the inclusion and exclusion criteria of this study.
Inclusion criteria
Articles were included if they met the following criteria: children aged 4–18 years; CP as the main diagnosis; a spastic movement disorder classified GMFCS level I–III; participant having undergone SEMLS; a post-surgery PTT program has been described. Articles that only describe single-level surgery, surgical techniques, and use of specific measuring instruments instead of intervention were excluded.
Data extraction and analysis: assessment of literature
The following data were extracted from all eligible studies and tabulated: first author, year of publication, number of participants, GMFCS level, age, gender, unilateral or bilateral impairment, type of surgery, the description of the PTT, and outcome measures.
The included RCTs and cohort studies were assessed for methodological quality using the Cochrane Centre assessment forms. 12 Sum scores for the assessment forms are discouraged by The Cochrane Centre and for this reason were not established. 13
Results
Search yield
The electronic and reference search yielded 988 articles published in the period from 2006 to 2011. After removing duplicates and reviewing the titles and abstracts, 47 articles were selected. Following the application of the predefined inclusion and exclusion criteria, six articles were included in the process of reviewing (Figure1).

Flowchart detailing the literature search and selection process according to Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.
Study design
The included studies represented two cohort studies,14,15 and four RCTs.16–19 Three RCTs described the period after SEMLS and evaluated various physiotherapy approaches.17–19 One RCT described evaluation retrospectively after 2 years. 16 Two papers written by Patikas and colleagues appeared to be based on the same population. 16,17 We tried to contact the author for clarification, but did not receive any reply from the author’s correspondence address. We interpreted the articles as two different studies with similar designs. The study population ranged from 11 to 43 participants, with an exception of one cohort study (N = 85).14–19
Quality of the studies
In all studies, the subjects, therapists, and testers were not blinded; participants were distributed randomly; only the study of Seniorou and colleagues had no blind randomization. 18 The studies by Patikas et al. and Seniorou et al. did not mention ‘intention to treat.’17,18 The interventions (physical therapy programs) were insufficiently described in all articles. Although the results were described in cohort studies by Åkerstedt and Khan, no statistical testing took place.14,15 Khan 15 and Thomason et al. 19 mentioned the use of co-interventions (plaster, orthotics, devices), whereas in the other articles nothing was mentioned about co-intervention. Khan was not only the author but also the surgeon of all participants in his study, and additionally evaluated the outcomes. 15 This may cause a potential bias (see supplement Table 1).
Physiotherapeutic treatment options
Aims and conclusion are described in more detail per study. Supplement Table 2 shows the details of the study, population, surgery procedures, and follow-up. In Table 1 the treatment in each study is presented in detail, based on goal intervention, frequency, duration, intensity, and method of treatment; Table 2 presents outcome measures and results after SEMLS.
Physical therapy treatment in detail.

Hoffer MM, Feiwell E, Perry R, Perry J, Bonnett C. Functional ambulation in patients with myelomeningocele.
AE, active exercise group; CG, control group; CP, cerebral palsy; EG, exercise group; PRT, progressive resistance training; RPT, regular physical therapy; RM, repetion maximum; ROM, range of motion; SEMLS, single event multilevel surgery.
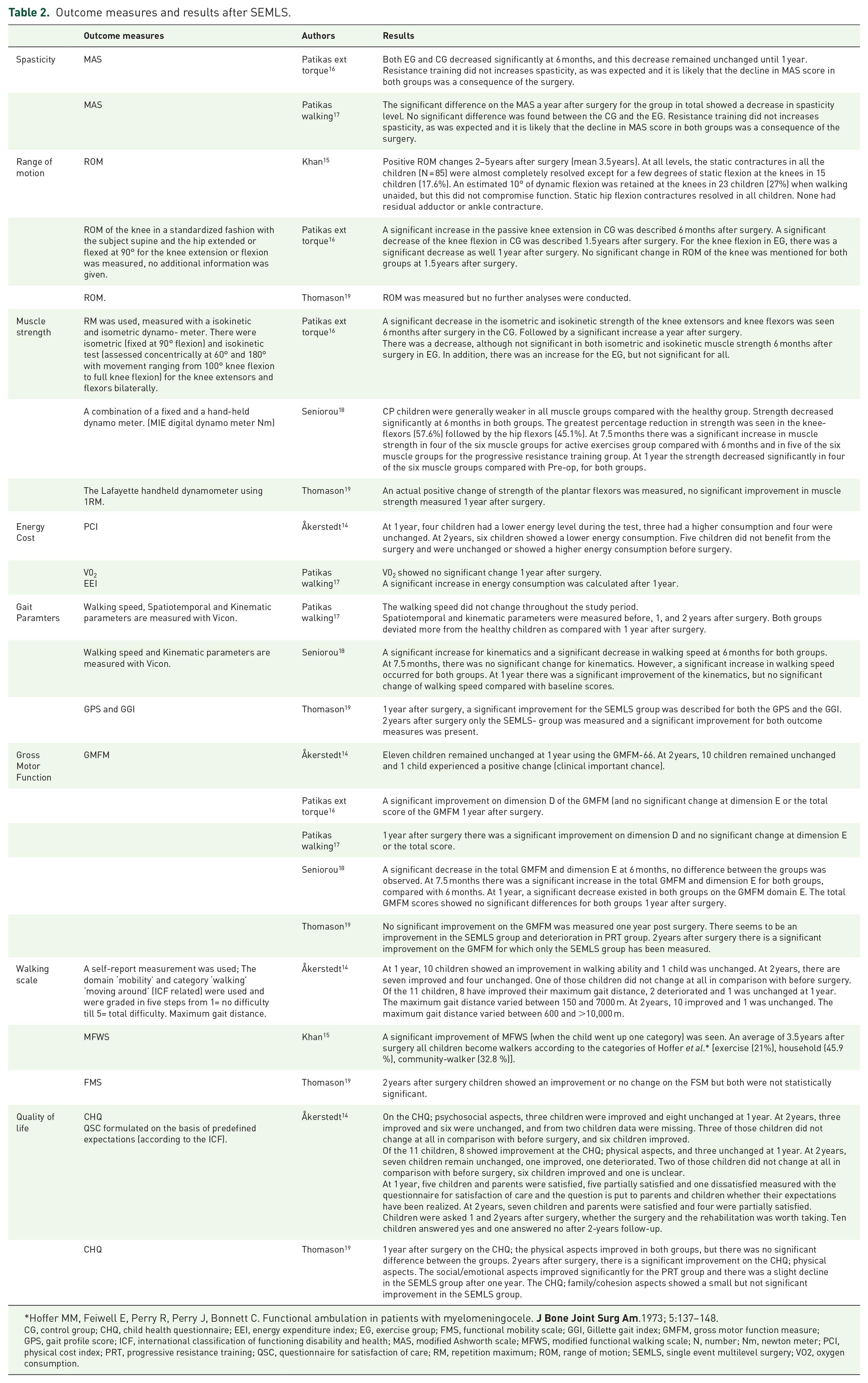
Outcome measures and results after SEMLS.
Hoffer MM, Feiwell E, Perry R, Perry J, Bonnett C. Functional ambulation in patients with myelomeningocele.
CG, control group; CHQ, child health questionnaire; EEI, energy expenditure index; EG, exercise group; FMS, functional mobility scale; GGI, Gillette gait index; GMFM, gross motor function measure; GPS, gait profile score; ICF, international classification of functioning disability and health; MAS, modified Ashworth scale; MFWS, modified functional walking scale; N, number; Nm, newton meter; PCI, physical cost index; PRT, progressive resistance training; QSC, questionnaire for satisfaction of care; RM, repetition maximum; ROM, range of motion; SEMLS, single event multilevel surgery; VO2, oxygen consumption.
Åkerstedt. 14
Aim of the study. This study evaluated SEMLS and rehabilitation from a broad perspective, that included clinical and self-reported functional measures at different levels of functioning according to the WHO ‘Classification of Functioning, Disability and Health’ (ICF) and a health-related quality of life (HRQOL). In addition, parents evaluated their satisfaction with the care given.
Conclusion. Self-reported walking ability improved after SEMLS and intensive rehabilitation. This result was partly supported by lower energy cost and improved Child Health Questionnaire (CHQ). Expectations and satisfaction were fulfilled for the majority of children.
Khan. 15
Aim of the study. By performing a SEML followed by a structural, supervised rehabilitation program (physiotherapy and orthotic support), walking is initiated in an untreated group. All participants presented as untreated nonwalkers, and had achieved sitting balance by the age of 5–6 years.
Conclusion. Children with CP who cannot walk and have not been treated can be helped by SEMLS, provided that inclusion criteria are followed and a structural, supervised rehabilitation program is in place.
Patikas. 17
Aim of the study. To investigate the effects of resistive exercise on the knee extension and flexion torque production during the rehabilitation period after multilevel orthopaedic surgery. The question was raised whether a home-based exercise program of 9 months duration, focused on muscle strength and which started 3–4 weeks after surgery (T1), would be better to maintain muscle power in comparison with regular physiotherapy (RPT). The former program is named the Exercise Group, or EG; the latter is the Control Group, or CG. It was advocated that RPT was executed in a standardized way.
Conclusion. The additional resistive exercise program had only marginal effects on preventing muscle weakness during the postoperative rehabilitation period. Additional long-term, home-based, low-cost, resistive exercise that starts soon after the operation of patients with CP was not more beneficial than conventional PTT only, in terms of strength and gross motor function measure (GMFM).
Patikas and walking. 16
Aim of the study. The purpose of this study was to examine the effect of a postoperative long-term strength-training program (EG) in addition to physiotherapy (CG) in children with CP after SEMLS, with minimal requirements in equipment and costs, and with exercises and movements that are important in everyday life.
Conclusion. The examined parameters may be more substantially influenced by factors such as the surgery outcome and the variability of pathologic characteristics than by the strength-training program per se. However, a more significant effect of strength-training may appear if more intense and short-term protocols are used, considering factors such as patients’ motivations, age and postoperative status.
Seniorou. 18
Aims of the study:
(1) The reliability of the isometric strength-testing protocol in a pilot study of healthy children and spastic diplegic cerebral palsy (SDCP).
(2) Quantified changes in lower-limb muscle strength, gait and motor function in children with SDCP following SEMLS.
(3) Evaluating two different methods of postoperative physiotherapy (resistance training/active exercise, both focused on muscle strengthening but based on different principles.
At 6 months postoperatively, the participants were divided in two groups: a progressive resistance training group (PRT) versus thane active exercises group (AE). Both groups started 6 months after surgery. The program duration was 6 weeks. Until the start of these specific programs, the children received RPT for 6 months.
Conclusion. The protocol for isometric muscle strength measurement is reliable. Despite kinematic improvements, there was significant reduction of muscle strength in all muscle groups at 6 and 12 months postoperatively. Following 6 weeks of intensive physiotherapy, both groups showed significant improvement in muscle strength, GMFM scores, and gait parameters.
Thomason. 19
Aim of the study. The aim was to evaluate the magnitude of change between groups and over time, based on gait indices, physical measures, function, activity, mobility, and health-related quality of life following SEMLS. The PRT group participated in PRT training. The randomized phase of the trial concluded at 12 months. The PRT group then exited the study and progressed to surgery, whereas the surgical group (SEMLS) continued to be followed in a prospective cohort study. The PRT group continued RPT the first 3 months, in the second 3 months they received PRT to match the intensive PTT received by SEMLS.
Conclusion. This article provides level-II evidence that SEMLS improves the gait of children with spastic diplegic cerebral palsy 12 months after surgery. Improvements in other domains, including gross motor function and quality of life, were not observed until 24 months after surgery.
Conclusion
This qualitative systematic review included six articles to answer the following questions: What physical therapy treatment for children with CP after SEMLS has been described in scientific literature? What outcome measures are used? What instruments are used to measure the outcome measures?
Related to the first research question, the review resulted in both an incomplete description of the PTT and a variety of treatment in all studies, with a small level of agreement (see Table 1). All studies described different goals. The goal of the physiotherapy treatment described entailed mainly improving muscle strength training, balance, range of motion (ROM), function, standing, and walking. RPT is mentioned without any description of methods.
All studies mentioned the frequency of the therapy, and the range was from less than one time per week to four times a week. The period for the training programs varied from 6 weeks to 2 years, or was not mentioned at all. The training session varied from 30 to 120 min. Intensity varied from two sets of five repetitions up to three sets of seven repetitions, and from five muscle groups to seven muscle groups per session.
The treatment descriptions varied from progressive resistance training to active exercise and passive movement, muscle strength training, stretching, balance, and gait training, to more complex functional tasks. No specific information was presented related to specific training methods. Because of the variation and the lack of description of the five domains of the PTT, it is difficult to draw straightforward conclusions related to the PTT.
Related to the second and third research questions, a wide range of outcome measures was described. The outcome measures and measurements are categorized into eight domains based on frequently used parameters in RPT in children with CP: spasticity, ROM, muscle strength, energy cost, gait parameters, gross motor function, walking scales, and quality of life, modified Ashworth scale (MAS), and ROM of the knee, hip, ankle using goniometers (see Table 2).20,21 Strength was measured both for different muscle groups in all studies, using different instruments, namely isokinetic and isometric dynamometer, the repetition maximum (RM) method, and a combination of a fixed and a hand-held dynamometer (MIE digital dynamometer Nm, and the Lafayette hand-held dynamometer). All authors measured knee-extensors with different results: a decrease, an increase, and no differences in muscle strength. All these studies indicated that the muscle strength is weaker post SEMLS than before surgery, up to 6 and 12 months after surgery. Different walking scales were used to measure effects on walking: a self-report measurement – the domain ‘mobility’ and category ‘walking’ ‘moving around’ (ICF-related), maximum walking distance, the Modified Functional Walking Scale (MFWS), and the Functional Mobility Scale (FMS). Quality of life was reported using the Child Health Questionnaire (CHQ) and the CHQ-Parent Form 50 (CHQ-PF50). Based on the PTT, a positive effect on walking, energy costs, improvement of the quality of walking after 1 or 2 years, and increase of walking speed. Furthermore, an improvement in GMFM 2 year post SEMSL has been shown, and variable results after 1 year. Harvey and colleagues support that gross motor function deteriorates post SEMLS, and starts to be more efficient 2 years after SEMLS. 22 The large variation in outcome measures, the different types of measurements and the noncomparable follow-up period (see Table 2) was expected due to the variety in the individualized treatment goals, such as performing transfers, standing on two legs, walking with heel strike, etc.
To conclude: the studies showed agreement only on muscle strength training, the use of RPT, use of GMFM, and duration of recovery time and intensive rehabilitation of more than 1 year after SEMLS. Because the studies do not provide clear suggestions for PTT after SEMLS, or measuring instruments and outcome measures, we developed a preliminary protocol of PTT after SEMLS (see appendix: supplement preliminary protocol). This protocol includes goals, frequency, duration, intensity, method, and the selection of instruments. We described the most important elements that should be incorporated in PTT based on evidence in SEMLS and CP, and we developed a protocol for PTT after SEMLS.
Supporting evidence for elements in PTT
It is not just the complexity of the surgery but also the period of immobilization following SEMLS that has a great physical impact on function, activity, and participation level (ICF-CY) of the child. 23 Any period of immobilization will reduce strength, coordination, and cardiovascular condition,14,16,17 and there is a reduced amount of mobility, which has great impact on the relevant standing and walking ability of the children.24–26 The period of immobilization will vary according to the type of surgery protocol, and will differ by center. On body and function level, strength training, coordination, ROM changes, balance during standing and walking, and fitness training are all essential elements in the treatment for the child to relearn to move within the new alignment. Motor skill and functional gait training are crucial to relearn a new motor pattern on standing and walking at the level of activity and participation.3,16–20,25,27–33 Muscle strength will be trained by using the progressive resistance exercise method according to FITT-factors (Frequency, Intensity, Time, and Type of training).27,34 Strength training deserves extra attention in the post-surgery PTT, as advocated by Dodd et al. and Heyrman et al.35,36 This is in line with conclusions in Dutch and international guidelines about strength training in children with CP.3,27 In addition, the decrease in muscle strength, even a considerable period after surgery, is an important outcome for managing the expectations of parents and children, and thus has a significant influence on the effect of treatment.24,25 Motor skill and functional gait training, especially quality of gait, will be supported with technology such as a partial body weight-supported treadmill and overground training and Gait Real-time Analysis Interactive Lab (GRAIL) training, and has a motivational and valuable influence in the treatment of these children.29–31,33,37 Coordination, ROM changes, balance during standing and walking, and fitness training will be integrated in this treatment.20,32 Because the prospect of improved quality of gait is decisive for the choice of SEMLS, it is important that possible future results related to quality of gait are transparent. The desired effects to achieve after SEMLS also require a long-term effort by parents and children. In order to make adequate use of the new alignment and gait opportunities (possibilities), co-interventions such as plaster, orthotics, and devices are needed in the post-surgery intervention plan. 19 It is therefore important for parents, child, and practitioners that the PTT program is very clear in advance; including goal, frequency, duration, intensity, and method of treatment, along with the logistics and the efforts needed pre, peri and post SEMLS. In order to monitor the treatment process, we suggest the importance of managing expectations. Furthermore, we firmly believe that the more active children and parents are engaged in the treatment process, the more effective PTT after SEMLS will be.9,25,26,28
Crucial factors to take into consideration after SEMLS are pain and fatigue due to a period of immobilization. These can be restrictive factors during PTT.25,26,28 It is important for the motivation of the child and parents to keep in mind the aim of performing SEMLS, and to link that aim to participation goals, which affect overall well being. 25 The newly developed gait outcome assessment list (GOAL questionnaire will be a good questionnaire to add. 38
Based on the description of these elements, we provide a protocol for PTT after SEMLS as a first set-up, based on best practice and available evidence in SEMLS and CP. We hope that the protocol provides directions on all ICF-CY levels. This protocol is described in an accompanying file (see appendix: supplement preliminary protocol).
Supplemental Material
Supplement_Combined_tables_and_appendices – Supplemental material for Physical therapy treatment in children with cerebral palsy after single-event multilevel surgery: a qualitative systematic review. A first step towards a clinical guideline for physical therapy after single-event multilevel surgery
Supplemental material, Supplement_Combined_tables_and_appendices for Physical therapy treatment in children with cerebral palsy after single-event multilevel surgery: a qualitative systematic review. A first step towards a clinical guideline for physical therapy after single-event multilevel surgery by Esther E.H. van Bommel, Marieke M.E. Arts, Peter H. Jongerius, Julia Ratter and Eugene A.A. Rameckers in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Special thanks goes to Koen Dortmans and Arnt Schellekens for editing the paper, and Tracey Keij-Denton for assistance with English language editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.