
Abstract
Objective:
People with nondialysis-dependent chronic kidney disease (CKD) and renal transplant recipients (RTRs) have compromised physical function and reduced physical activity (PA) levels. Whilst established in healthy older adults and other chronic diseases, this association remains underexplored in CKD. We aimed to review the existing research investigating poor physical function and PA with clinical outcome in nondialysis CKD.
Data sources:
Electronic databases (PubMed, MEDLINE, EMBASE, Web of Science, Cochrane Central Register of Controlled Trials) were searched until December 2017 for cohort studies reporting objective or subjective measures of PA and physical function and the associations with adverse clinical outcomes and all-cause mortality in patients with nondialysis CKD stages 1–5 and RTRs. The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42016039060).
Review methods:
Study quality was assessed using the Newcastle-Ottawa Scale and the Agency for Healthcare and Research Quality (AHRQ) standards.
Results:
A total of 29 studies were included; 12 reporting on physical function and 17 on PA. Only eight studies were conducted with RTRs. The majority were classified as ‘good’ according to the AHRQ standards. Although not appropriate for meta-analysis due to variance in the outcome measures reported, a coherent pattern was seen with higher mortality rates or prevalence of adverse clinical events associated with lower PA and physical function levels, irrespective of the measurement tool used. Sources of bias included incomplete description of participant flow through the study and over reliance on self-report measures.
Conclusions:
In nondialysis CKD, survival rates correlate with greater PA and physical function levels. Further trials are required to investigate causality and the effectiveness of physical function and PA interventions in improving outcomes. Future work should identify standard assessment protocols for PA and physical function.
Introduction
Chronic kidney disease (CKD) is a long-term condition affecting approximately three million people in the UK and over 61,000 people have end-stage renal disease and require dialysis or a renal transplant. 1 Research into kidney disease has historically tended to concentrate on patients with severe renal impairment requiring renal replacement therapy, however there is a significant proportion of the UK population living with earlier stage CKD and interventions to promote a healthy lifestyle with this group are starting to emerge.
People living with nondialysis CKD experience a high symptom burden with progressively impaired physical function and low levels of physical activity (PA). These negatively affect quality of life (QoL) and independence.2,3 In patients with nondialysis CKD, even a small increase in regular PA levels can improve self-reported quality of health and life, as well as improving exercise tolerance and cardiovascular reactivity. 4 In older adults, 5 and in other chronic disease populations such as diabetes,6,7 it is well established that both reduced physical function and PA are associated with an increased risk of cardiovascular disease (CVD) and all-cause mortality.8,9 Whilst evidence is limited in nondialysis CKD populations, it is well established in patients undergoing dialysis that both self-reported10–13 and objective13–15 physical function is a significant and independent predictor of all-cause mortality and future hospitalization. Notably, regularly physically active dialysis patients have a decreased risk of CVD and death, 16 however the physiological and social impact of dialysis is such that findings in this group are not directly transferable to a patient population that does not require renal replacement therapy. Although renal transplant recipients (RTRs) generally report improved physical function, PA, and QoL following transplantation, it often remains poor,17,18 and patients who have undergone transplantation remain at high risk of CVD. 19
Physical function and PA are two key ‘modifiable’ lifestyle factors that may reduce mortality and clinical adverse events and have a positive impact on quality of life in nondialysis CKD and RTRs. Furthermore, early identification, using simple physical function or PA measures, of patients at risk of clinical adverse events may focus interventions (e.g. exercise or nutrition) designed to improve such outcomes.
Physical function and PA should be viewed as two independent concepts. Physical function is the ability to perform activities of daily living, and is assessed using simple tests to reflect these tasks (e.g. getting out of a chair) or by subjectively rating competency in completing different tasks. 13 PA is any bodily movement produced by contraction of skeletal muscle that increases energy expenditure above a basal level. 20 PA and physical function correlate significantly and both concepts are important to clinicians and patients, hence this review will explore the relationship of each with clinical outcomes.
We performed a systematic review to identify the association between physical function and PA with all-cause mortality and other adverse clinical outcomes in nondialysis CKD (i.e. including RTRs). No systematic review of the current literature has been performed on this association in this patient group. We hypothesized that patients with nondialysis CKD who are functionally limited or less physically active will demonstrate a higher risk of all-cause mortality and adverse clinical outcomes.
Methods
Protocol and registration
The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42016039060). Data are reported in line with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISMA) guidelines. 21
Search strategy and selection criteria
We aimed to identify observational studies that explored the link between physical function, PA, and adverse clinical outcomes and all-cause mortality in nondialysis CKD. The primary question of interest was the association between objective and subjective measures of physical function, PA, and the likelihood of death (i.e. all-cause mortality) and adverse clinical outcomes in patients with CKD not currently requiring dialysis therapy. For the purpose of this review, an ‘adverse clinical outcome’ was defined as one (or more) of the following events: end-stage renal disease (i.e. the need for/time to dialysis), unforeseen hospital admission, or nonfatal cardiovascular event (e.g. myocardial infarction, stroke, etc.). The primary outcome of interest was all-cause mortality.
Data sources and search strategy
The following electronic databases were searched from their date of establishment to July 2016 and a further search was performed in December 2017 to gather any new literature. National Centre for Biotechnology Information (NCBI) PubMed [which includes the Medical Literature Analysis and Retrieval System Online (MEDLINE)], Excerpta Medica dataBASE (EMBASE), Web of Science (WOS) (which includes the KCI-Korean Journal Database, MEDLINE, Russian Science Citation Index, and SciELO Citation Index), and the Cochrane Central Register of Controlled Trials (CENTRAL). The search strategy was tailored to each database and used a combination of key words and medical subject headings (MeSH). MeSH search terms were: ‘kidney diseases’, ‘kidney transplantation’, ‘physical activity’, ‘mortality’, ‘death’, ‘cardiovascular event’. Other non-MeSH search terms used were: ‘renal impairment’, ‘physical function’, ‘physical performance’, ‘disability’, ‘all-cause mortality’, ‘cardiovascular diseases’, ‘adverse event’, ‘hospital admission’.
As per the PRISMA statement, an example full electronic search strategy can be found for the NCBI PubMed database in supplementary material 1.
Article eligibility criteria
The eligibility for full text review of each citation was independently evaluated by two authors (HJM, TJW) on the basis of title and abstract. Any article deemed potentially relevant was retrieved for full text review. The reference lists of any relevant articles were also screened to identify studies which may have been missed in the search.
Inclusion criteria
Human adults (aged 18 years or over).
CKD (any stage) or RTRs.
Cohort studies including secondary analysis of randomized control trials and abstracts.
Reporting physical function or PA outcome measures.
Reporting association with adverse clinical outcomes and all-cause mortality in either unadjusted or adjusted terms.
Specific exclusion criteria
Renal failure; any dialysis modality.
Review articles.
Animal trials.
Non-English articles.
Data extraction
Following a preliminary pilot search in NCBI PubMed, a data extraction form was created to capture relevant information from included studies. Each article was reviewed by two independent members of the research team during the data extraction process. The following information was extracted for each study:
Study characteristics: such as the year of publication, study design, and sample size.
Patient characteristics, such as mean age, sex distribution, race, and comorbidities.
Definitions and incidences of CKD, physical function (or its associated domains), PA, clinical adverse events, and all-cause mortality.
Reported association of physical function or PA with adverse clinical outcomes or all-cause mortality in either unadjusted or adjusted terms (e.g. hazard or odds ratio).
Evaluation of quality and risk of bias
Each study was evaluated for quality and risk of bias using the Newcastle-Ottawa Scale (NOS) 22 independently by two reviewers. Discrepancies in scoring were settled by mutual agreement. The primary authors (HJM and TJW) had the final verdict decision. The NOS is a quality evaluation method for nonrandomized studies which uses three criteria: selection, comparability, and outcome. Each study is designated a number of stars for each section, based on predetermined queries. 22 The NOS has been extensively used to evaluate quality and bias for systematic reviews and meta-analyses and is recommended by the Cochrane Collaboration. 23 Scores from the NOS were transformed into Agency for Healthcare Research and Quality (AHRQ) standards (‘good’, ‘fair’, and ‘poor’ quality). 22
Results
Study selection
A total of 6299 records were identified by systematic searching and 249 were deemed appropriate based upon the title and abstract alone. Upon removal of 211 duplicates, 38 records were assessed against the full eligibility criteria and 14 records were removed. One additional source was identified during the original review process. In December 2017, a re-search found four additional studies. A total of 29 trials were reviewed (see Figure 1).
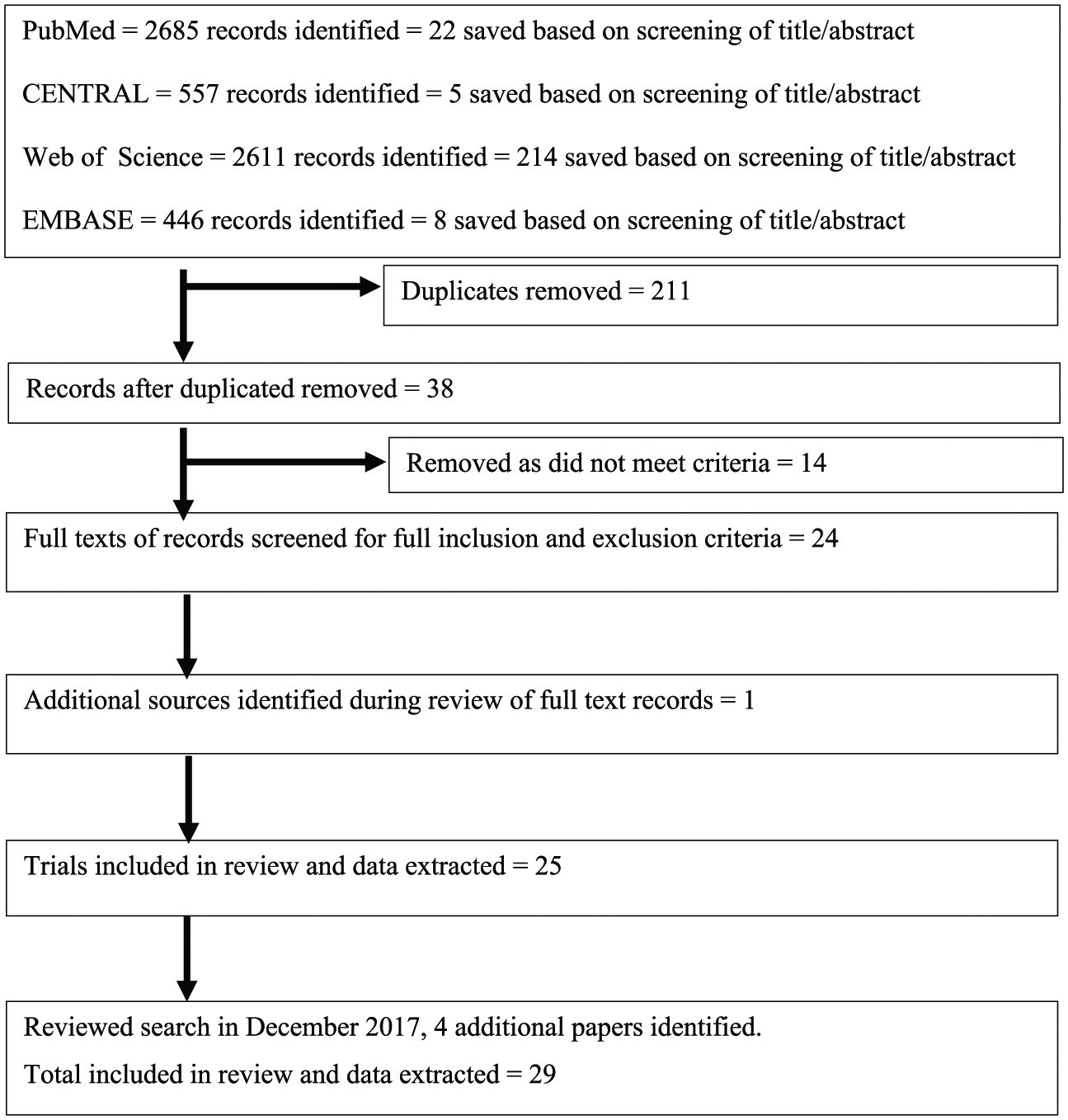
PRISMA flow diagram.
Study characteristics
Overall, the articles demonstrated a range of follow-up times (median follow up = 7.0 years; range 1 24 –15.9 years 25 ) and sample sizes (median = 719; range 26 26 –50, 620. 27 ) Studies were conducted in the USA,25,28–41Taiwan,27,42–44 Estonia, 26 the Netherlands, 45 Korea, 46 the UK,47,48 Italy, 24 Hungary, 49 Brazil, 50 Finland, 51 and Slovakia, 52 ensuring data from a variety of cultures are included which, although increasing generalizability, may mean culturally specific behaviour trends are masked. Studies included single-25,26,38,42–45,47,49,50,52 and multicentre investigations,24,30,33–37,39–41,48,51 and population-wide surveys.27–29,31,32,46 The majority of these studies are observational, except Pechter and colleagues 26 who described a 10-year programme of supervised hydrotherapy exercise, and Chen and colleagues 30 who reported observational data collected as part of a randomized controlled trial investigating the effects of different diets in kidney disease.
The disease populations studied varied, with 19 investigations conducted in nondialysis CKD,24,26–33,35,37,39,40,42,43,46,47,50 7 with RTRs,36,38,41,45,48,49,52 and Tikkanen-Dolenc and colleagues 51 studied both CKD and RTRs. Some studied all five stages of CKD,24,26–28,34,39,43,44,46,47,51 whilst others studied a fixed estimated glomerular filtration rate (eGFR) range.29–34,37,40,42,50 Gulati and colleagues 25 studied a female-only population with no pre-existing diagnosis of CKD, however the mean eGFR of the study population was 53.7 ml/min/1.73 m² and 79% were found to have an eGFR less than 60 ml/min/1.73 m². Further, Robinson-Cohen and colleagues 34 conducted a general population study but calculated hazard ratio (HR) for stratified eGFR bands and, henceforth, both of these papers have been included in the review. Two papers39,50 investigated physical function as a subset of another concept: Delgado and colleagues 39 investigated frailty in CKD, whilst Periera and colleagues 50 studied the incidence of sarcopenia. Similarly Chang and colleagues 43 measured hand-grip strength (HGS) to investigate the effects of protein-energy wasting.
The associations between physical function and all-cause mortality or adverse clinical outcomes are summarized in Table 1, and studies reporting the association between PA and outcomes can be found in Table 2. Ten papers investigated physical function, whilst 15 studied PA. Two papers used cumulative measures using both PA and physical function,34,38 however these have been included in the table corresponding to the main emphasis of the individual trial. Tsai and colleagues 44 investigated physical function as ‘indices’ of the person’s ability to engage in PA in addition to reporting PA behaviour.
Summary of findings; association between physical function and all-cause mortality or adverse clinical outcomes.

6MWD, 6 min walk distance; ADL, activities of daily living; CES-D, Centre for Epidemiologic Centres Scale for Depression; CI, confidence interval; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate (ml/min/1.73 m²); HGS, hand grip strength; HR, hazard ratio; HRQoL, health-related quality of life; KDQoL, Kidney Disease Quality of Life; MDRD LTPAQ, Modification of Diet in Renal Disease Leisure Time Physical Activity Questionnaire; MET, metabolic equivalent task; MR, mortality rate; N/A, not applicable; PA, physical activity; PCS, physical composite score; PF, physical function; RTR, renal transplant recipient; SD, standard deviation; SF-36, 36-item Short Form survey; SPPB, Short Physical Performance Battery; TUAG, timed-up-and-go; IADL, instrumental activities of daily living; mGFR, measured glomerular filtration.
Unadjusted model; $adjusted for age; ‡adjusted for sex; §adjusted for body mass index; ¶adjusted for eGFR; ||adjusted for additional covariants (see reference for full analysis).
Summary of findings; association between physical activity level and all-cause mortality or adverse clinical outcomes.
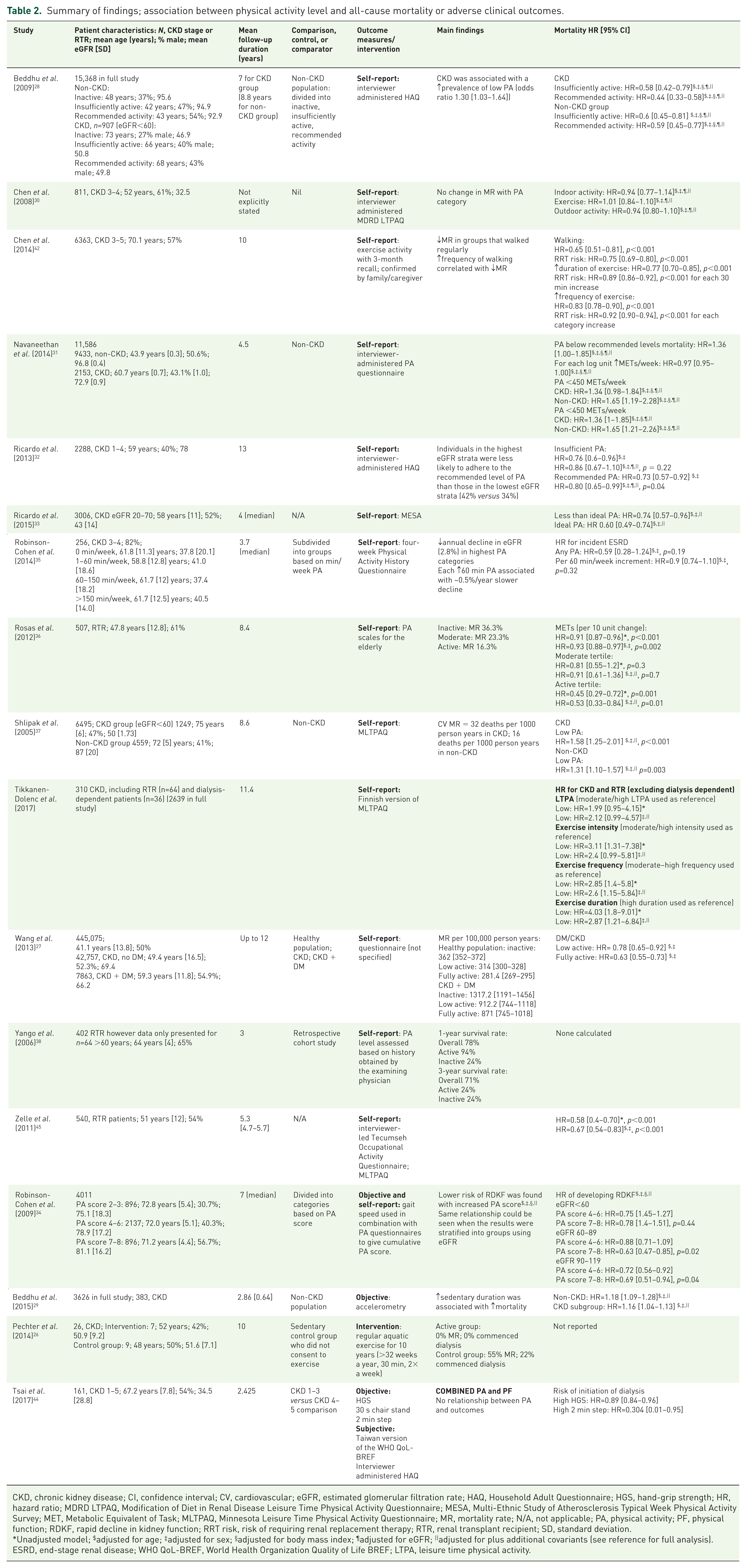
CKD, chronic kidney disease; CI, confidence interval; CV, cardiovascular; eGFR, estimated glomerular filtration rate; HAQ, Household Adult Questionnaire; HGS, hand-grip strength; HR, hazard ratio; MDRD LTPAQ, Modification of Diet in Renal Disease Leisure Time Physical Activity Questionnaire; MESA, Multi-Ethnic Study of Atherosclerosis Typical Week Physical Activity Survey; MET, Metabolic Equivalent of Task; MLTPAQ, Minnesota Leisure Time Physical Activity Questionnaire; MR, mortality rate; N/A, not applicable; PA, physical activity; PF, physical function; RDKF, rapid decline in kidney function; RRT risk, risk of requiring renal replacement therapy; RTR, renal transplant recipient; SD, standard deviation.
Unadjusted model; $adjusted for age; ‡adjusted for sex; §adjusted for body mass index; ¶adjusted for eGFR; ||adjusted for plus additional covariants (see reference for full analysis). ESRD, end-stage renal disease; WHO QoL-BREF, World Health Organization Quality of Life BREF; LTPA, leisure time physical activity.
Outcomes reported
The majority of the papers studied mortality, either as all-cause24–33,36,38–43,45–52 or cardiovascular mortality.37,45 Other outcomes reported included prevalence of frailty, 39 sarcopenia, 50 protein-energy wastage, 43 major adverse cardiovascular event, 44 first hospitalization, 44 rate of decline of renal function,34,35 or risk of requiring dialysis.26,42-44 One study reported an odds ratio of developing diabetic nephropathy. 27
Overall, the results showed that poorer physical function and lower PA were associated with increased mortality rates, however differing methodologies preclude meta-analysis. HRs were reported in some studies (summarized in Table 1) varying from 1.04 52 to 5.7, 24 dependent on measurement type and population studied.
Only 4 papers36,38,45,51 reviewed the importance of being active with a renal transplant and 441,48,49,52 of the 10 papers investigating physical function studied RTRs. Outcomes studied were all-cause mortality,36,38,41,45,48,49,51,52 cardiovascular mortality, 45 graft failure,38,45,48,49 and death with a functioning transplant.36,49 Higher PA levels both prior to transplantation 36 and post transplant38,45 were associated with lower mortality rates. Similarly lower physical function levels were associated with increased mortality HRs.48,49,52
Objective physical function
Six papers used objective measures of physical function, including the Short Physical Performance Battery (SPPB),24,41 HGS,43,44,50 using a Bruce protocol treadmill test to determine cardiorespiratory fitness, 25 the ‘timed-up-and-go’ (TUAG), 40 the 6 min walk test (6MWT), 40 30 s chair stands, 44 2 min step 44 and gait speed. 40 The Short Physical Performance Battery (SPPB), TUAG, the 6MWT, and gait speed were independently associated with increased all-cause mortality.24,40,41 Greater scores in the 2 min step were correlated with a reduced risk of commencing dialysis. 44 The number of chair stands achieved in 30 s was shown to correlate with reduced risk of a major adverse cardiovascular event and with all-cause hospitalization. 44 Since both TUAG and the SPPB include measures of a person’s gait speed and ability to stand from a chair, it may be inferred that a measure of physical function utilizing walking and standing provides a useful measure of physical function in CKD when outcomes are to be studied.
HGS was measured in three studies,40,43,50 with inconsistent results. Pereira and colleagues 50 measured HGS as a marker of sarcopenia which was demonstrated to correlate with mortality risk; Roshanravan and colleagues 40 found HGS was relatively preserved compared with lower limb strength, as 6MWT, gait speed, and TUAG had greater area under the Receiver Operating Characteristic (ROC) values than HGS. However, Chang and colleagues 43 found that HGS was an independent outcome predictor in CKD.
Cardiorespiratory fitness was found to modify the association between eGFR and mortality. 25 A maximum cardiorespiratory fitness level of less than 5 METs (metabolic equivalent of task ~17.5 ml/kg/min) combined with an eGFR of under 45 ml/min/1.73 m² was associated with increased mortality rates compared with those with better fitness and higher eGFR. 25
Objective physical activity
Only one study 29 used an objective PA measure (i.e. accelerometry), whilst another 34 combined gait speed with a questionnaire to give a cumulative PA score.
Subjective physical function
Self-report measures of physical function were used by six papers.39,46–49,52 The 36-item Short Form survey ‘SF-36’ was used in three of these,48,49,52 and a significant relationship between the ‘Physical Component Score’ (PCS) and outcomes was consistently demonstrated. The other subjective methods used included ‘Modification of Diet in Renal Disease (MDRD) Quality of Wellbeing measure’, 39 ‘Korean version of ADL’s’, 46 ‘Instrumental ADL’, 46 ‘Health Related Quality of Life (HRQoL)’ 48 and ‘Kidney Disease Quality of Life measure (KDQoL)’, 49 which included ‘HRQoL’, ‘SF-36’ and ‘Center for Epidemiologic Studies Depression Scale’ (CES-D). Similar trends were seen between poorer outcomes and lower physical function.
Subjective physical activity
Thirteen studies which explored PA associations used questionnaires, including ‘Household Adult’ questionnaire28,32 (a translated version was used by Tsai and colleagues 44 ), ‘Leisure Time Physical Activity Questionnaire’, 31 ‘Modified Diet in Renal Disease Leisure Time Physical Activity Questionnaire’ (MDRD LTPAQ), 30 ‘Four-Week Physical Activity History Questionnaire (FWH)’, 35 ‘Multi-Ethnic Study of Atherosclerosis (MESA) Typical Week Physical Activity Survey’, 33 ‘Physical Activity Scales for the Elderly’ (PASE), 36 ‘Minnesota Leisure Time PA’ questionnaire37,45 (a translated version was used by Tikkanen-Dolenc and colleagues 51 ), and ‘Tecumseh Occupational Activity Questionnaire’. 45 One study 27 failed to report which method was used and two used clinician judgement to classify PA.38, 42 Questionnaires were frequently used in conjunction with a compendium of activities to give MET score for further analysis.27,28,31–33,36,44,45,51
The most common PA reported was walking, with data showing that increasing walking duration and intensity correlates with favourable health benefits. The dose–response relationship remains unclear. Navaneethan and colleagues 31 and Ricardo and colleagues 33 demonstrated reduced mortality risk only when guideline PA levels were achieved (i.e. >150 min/week moderately vigorous PA) whilst Beddhu and colleagues 29 found replacing sedentary time with light activity resulted in a lower mortality risk but upgrading to moderate or vigorous PA did not reduce the risk further. Robinson-Cohen and colleagues 35 found the risk of developing end-stage renal disease decreased with every 60 min/week increase in PA, with the largest reduction when more than 150 min was achieved. Similarly, Tikkanen-Dolenc and colleagues 51 stratified HRs according to intensity, duration, and frequency of PA, and demonstrated increased HRs when each of these differed from the guideline amounts, with the greatest increase in risk when target duration of PA was not achieved. In contrast, Tsai and colleagues 44 found no change in HRs with PA levels as measured by questionnaires, but found that various functional measures were significant. Whilst these studies demonstrate interesting, although conflicting, conclusions, despite large sample sizes, the p values reported are often not significant 35 or not specified.29,31,33
Risk of bias
Each study was evaluated for quality and risk of bias using the Newcastle-Ottawa Scale and Agency for Healthcare Research and Quality (AHRQ) standards. These results are summarized in Table 3. Overall the quality of these papers was mixed, with 20 classed as ‘good’, 7 as ‘fair’, and 2 determined to be ‘poor’ quality. Sources of potential bias identified included not fully describing the participant flow through the study and the use of self-report measures.
Papers reviewed, Newcastle-Ottawa Scale score, and bias criteria.

AHRQ, Agency for Healthcare and Research Quality.
Discussion
Summary of review findings
Overall, our review has shown that, in patients with nondialysis CKD, reduced physical function and PA levels are associated with increased mortality and adverse clinical events, including decline in renal function, increased risk of requiring renal replacement therapy, and poor renal graft survival (RTRs only). Similar observations have been observed in dialysis patients 16 and in other chronic populations.6,7 This has important clinical implications, potentially providing an opportunity to improve outcomes. The concepts of PA and physical function have significant overlap and although engagement in functional tasks can be considered a category of PA, function can also be considered an antecedent of activity. The two concepts are also frequently intertwined in the literature, which necessitated the consideration of the two ideas in the same review.
Bias was assessed in this review using the NOS. Interestingly, the papers studying disease progression were scored negatively by the NOS as the outcome (i.e. CKD) was present at the start of the trial and this represents a weakness for this scoring system. HRs were reported in many, but not all, papers; however some studies reported mortality risk whilst others reported survival analysis, making the data unsuitable for meta-analysis. Studies which yielded HRs were calculated both as unadjusted models and adjusted for confounding variables, such as age, body mass index (BMI), sex, depression, and kidney function levels; however sensitivity analysis to confirm these findings was poorly reported.
It is important to state the difficulty deducing causality from the data presented, as patients with greater illness burden are often less active and have a reduced functional level. Further longitudinal studies are needed whereby interventions increase PA or physical function to assess resultant changes in outcomes. Further research is needed into the potential dose–response of PA, and whilst it appears that being active on most days, in line with the current PA recommendations, is beneficial, even low levels of PA may confer some benefit in renal patients. It is also important to consider that there is a physical function minima, below which PA is impossible. While, in principle, encouraging patients to be more active may be a straightforward suggestion, the complexity of successful behaviour change interventions should not be underestimated.
The data were not appropriate for meta-analysis due to the variance in the measurement outcomes and the analysis methods used. This demonstrates the need to identify accepted norm assessments of physical function and PA to use in the renal community to allow comparison between interventions. The paucity of research in the transplant population is also demonstrated in regard to both PA and physical function.
Physical function and outcome
Reduced physical function was found to correlate with frailty, sarcopenia, and protein-energy wastage which, in turn, are associated with mortality. Despite the potential confounders introduced by investigating these wider concepts, the value of maintaining functional ability and activity levels remained clear. Only one paper 49 assessed depression as a covariant when exploring the relationship between physical function and mortality. Once the HR analysis was adjusted, the significance of the model dropped. Due to the frequent concomitance of depression and functional loss, further investigations are required to determine whether this is a trend as yet uncharted, or a coincident pattern.
Doyle and colleagues 47 assessed physical function using the Barthel score, where ability to engage in activities of daily living is assigned an ordinal score, and demonstrating a higher score on hospital discharge was associated with a lower risk of all-cause mortality. Whilst this score is frequently used by clinicians as an objective measure, it is unclear in this paper whether it was used objectively or as a self-report tool. Ricardo and colleagues 32 calculated a ‘healthy lifestyle score’, based on BMI, PA levels, dietary intake, and smoking behaviour. Their results demonstrated a positive relationship between a ‘healthy’ lifestyle and mortality rates, but it is difficult to isolate the effect of PA.
Objective tests were more commonly used to measure physical function. A gait speed reduction of 0.1 m/s was associated with a 26% increased mortality risk, whilst a 1 s longer TUAG score correlated with an 8% increased risk of death. 40 Thus these objective tests could be useful prognostic tools in CKD, and may provide interventional targets yielding direct patient benefit. HGS measurement generated inconsistent results and hence requires further investigation before recommendations can be made about its use as an outcome measure in nondialysis CKD.
Physical activity and outcome
Interestingly, Pechter and colleagues 26 found 100% survival in patients who maintained engagement in a 10-year hydrotherapy programme compared with 55% in the control group (no exercise) who either died or required renal replacement therapy. However, it may be argued that only the patient group with a low comorbidity burden are able to engage continuously in this type of intervention, which may confound these results. It must be considered that financing such supervised exercise for the entire CKD population is untenable under modern health systems. Conversely, Chen and colleagues 30 reported no change in mortality risk with higher PA levels, although the authors acknowledge the data’s wide confidence intervals. Also, the sample studied was generally more active than a general CKD cohort, with 50% walking or exercising regularly.
Measurement of PA should be conducted using objective accelerometry if possible, however only one paper utilized this outcome measure. This diversity of PA measures also means that cutoffs determining ‘activity’ or ‘inactivity’ vary widely, and as such, different constructs are being compared. This also limits exploration of dose–response effects and potential benefits.
Outcome measure use
A key finding from this review was the large breadth of measures used to assess both physical function and PA. Both objective and subjective measures were used, and whilst each confer their own strength and limitations, the heterogeneity makes it difficult to compare effects and prevents meta-analysis. In many instances, questionnaire-based assessments were used, particularly in the measurement of PA level. This has substantial limitations in regard to recall bias and desirable responses, and for some of these questionnaires validity in the renal population remains undemonstrated. Some questionnaires were administered by interviewers,30–32,37,45 which may have increased completion rates and corrected one of the common criticisms of questionnaire use. In Yango and colleagues, 38 retrospective clinician judgement on patient PA level was used, and such subjectivity means minimal conclusions can be drawn from this trial. Methodological flaws were also demonstrated by Chen and colleagues 42 who asked participants and their caregivers to recall a 3-month history of PA. The ‘Minnesota Leisure Time Physical Activity’ questionnaire, used by three studies,37,45,51 has been criticized as it requires a full year’s recall which has been previously demonstrated to be limited by recall bias. 53 We propose future researchers should use commonly reported and validated measures to aid synthesis of data between clinical trials. The SF-36 was used by three papers48,49,52 and a one-point increase in the PCS correlated with a decrease in mortality risk in RTRs of between 1.8% 49 and 4%, 52 and hence this subjective outcome measure is recommended for further use.
Despite a consensus among nephrologists that PA is important for patients, assessment of physical function or PA advice is not a part of the routine management of CKD. Efforts to improve both physical function and PA by intervention should be actively encouraged in this group. In regard to physical function, it appears simple objective tests, such as the TUAG and gait speed (but perhaps not HGS), and self-reported measures, in particular the SF-36 (PCS), are useful prognostic tools in CKD. As such, research or clinical practice should use these physical function tests when assessing intervention effects. Complex and ‘laboratory’-based measures, such as those measuring VO2 or using an accelerometer or isokinetic dynamometer, provide high-quality and reliable data, however these assessments are often impractical in a clinical setting and poorly tolerated by patients. More pragmatic measures of physical function and physical activity, such as the TUAG, gait speed, or via self-report, can be quickly and cheaply conducted in a clinic waiting room and hence provide a real-world method of assessing the patient’s functional status which correlates with morbidity and mortality. When assessing either physical functioning or activity, a researcher or healthcare professional should be aware of the relative strengths and limitations of each assessment.
Conclusion
This is the first systematic review elucidating the relationship between physical function and PA with clinical outcomes in the underexplored area of nondialysis CKD. Better physical function and greater PA levels both correlate with improved outcomes, including both reduced all-cause and cardiovascular mortality risk, reduced risk of rapid decline in renal function, reduced prevalence of frailty and sarcopenia, and graft survival in transplant recipients. However, causality as yet remains unproved and further research is needed.
Clinical messages
Reduced physical function and PA levels are associated with increased mortality risk and increased risk of adverse clinical outcomes in both nondialysis CKD and in RTRs. Further work is needed to investigate causality within this relationship. Consistent use of outcome assessments is critical to allow meta-analysis.
Supplemental Material
Supplementary_material_1_-_Example_PubMed_search_strat – Supplemental material for The association of physical function and physical activity with all-cause mortality and adverse clinical outcomes in nondialysis chronic kidney disease: a systematic review
Supplemental material, Supplementary_material_1_-_Example_PubMed_search_strat for The association of physical function and physical activity with all-cause mortality and adverse clinical outcomes in nondialysis chronic kidney disease: a systematic review by Heather J. MacKinnon, Thomas J. Wilkinson, Amy L. Clarke, Douglas W. Gould, Thomas F. O’Sullivan, Soteris Xenophontos, Emma L. Watson, Sally J. Singh and Alice C. Smith in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Initial design: ACS, TJW, HJM; conducting searches: TJW, HJM; article retrieval: TJW, HJM; article review: HJM, TJW, ALC, DWG, ELW, TFO, SX, ACS; drafting manuscript: HJM, TJW; editing manuscript: HJM, TJW, ALC, DWG, ELW, TFO, ACS; mentoring: SJS, ACS. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research Leicester BRC, CLAHRC EM or the Department of Health and Social Care
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report is independent research supported by the National Institute for Health Research Leicester Biomedical Research Centre and the NIHR Collaboration for Leadership in Applied Health Research and Care East Midlands (CLAHRC EM). We also gratefully acknowledge additional funding from The Stoneygate Trust.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.