
Abstract
The most common extra-intestinal manifestation in patients with inflammatory bowel disease (IBD) is articular involvement, with a prevalence ranging between 17% and 39%. It is frequently characterized by an involvement of the axial joints but may also be associated with peripheral arthritis. The target of therapy in the management of arthritis associated with IBD is to reduce the inflammation and prevent any disability and/or deformity. This requires active cooperation between gastroenterologist and rheumatologist. The treatment of axial involvement has focused on the combination of exercise with nonsteroidal anti-inflammatory drugs. Immunomodulators have been efficacious in patients with peripheral arthritis and other extra-intestinal manifestations, but they are not effective for the treatment of axial symptoms of spondylitis. Tumor necrosis factor (TNF) α inhibitors have been proven to be highly effective in the treatment of IBD patients which are steroid-dependent or refractory to conventional therapy and in patients with associated articular manifestations. The treatment of peripheral involvement and/or enthesitis and/or dactylitis is based on local steroid injections, while sulfasalazine and/or low doses of systemic steroids may be useful in case of inadequate response to intra-articular steroids. Sulfasalazine induces only a little improvement in peripheral arthritis. Immunomodulators such as methotrexate, azathioprine, cyclosporine and leflunomide show their efficacy in some patients with peripheral arthritis and other extra-intestinal components. TNF-α inhibitors should be considered the first-line therapeutic approach when moderate-to-severe luminal Crohn’s disease or ulcerative colitis is associated with polyarthritis. The aim of this review is to provide a fair summary of current treatment options for the arthritis associated with IBD.
Introduction
Rheumatic manifestations have been described in patients with inflammatory bowel disease (IBD) for many years, but it was only in the late 1950s that the arthritis occurring in IBD patients was made distinct from classic rheumatoid arthritis (RA) [Steinberg and Storey, 1957; Bywaters and Ansell, 1958; McBride et al. 1963; Stewart and Ansell, 1963]. In 1964, the American Rheumatism Association classified arthritis occurring in IBD as an independent clinical form [Blumberg et al. 1964] and later Wright and Moll included enteropathic arthritis (EA) definitively in the spondyloarthritis (SpA) group [Wright and Moll, 1976].
The most common extra-intestinal manifestation in IBD patients is articular involvement, with a prevalence ranging between 17 and 39%. It is frequently characterized by an involvement of the axial joints, but may also be associated with peripheral arthritis such as synovitis and/or dactylitis and/or enthesopathy [Peluso et al. 2013b].
The spectrum of axial involvement ranges from inflammatory lower back pain with or without radiological evidence of sacroiliitis (sometimes asymptomatic) to spondylitis characterized by the classic clinical and radiologic features of the idiopathic ankylosing spondylitis (AS). The onset of axial involvement often precedes the onset of IBD and is not influenced by bowel surgery [Baeten et al. 2002].
The peripheral arthritis was categorized by Orchard and colleagues at the end of 1990s as two subtypes: type 1, the pauci-articular form (acute and self-limited, which may precede the diagnosis of IBD, generally running parallel to the intestinal disease); and type 2, the polyarticular form (with symptoms lasting for months or years, independently from IBD [Orchard et al. 1998]. Moreover, Smale and colleagues have supposed another type of peripheral arthritis (type 3) that includes patients with both axial and peripheral forms [Smale et al. 2001]; its onset was more recently studied by our research group [Peluso et al. 2012] using magnetic resonance imaging (MRI), an imaging technique usually accepted to evaluate the peripheral [Soscia et al. 2009; Amrami, 2012] and axial involvement of SpA [Lambert et al. 2009]. MRI may be useful for the early diagnosis of EA, or when there are not findings with conventional X-ray examination.
Moreover, the clinical spectrum of EA is also characterized by several extra-articular (intestinal) manifestations such as skin and mucous membrane lesions, eye involvement, genitourinary inflammation and cardiac complaints [Peluso et al. 2014]. Erythema nodosum and pyoderma gangrenosum are described as the most common cutaneous manifestations occurring in 10–25% of IBD patients [Ampuero et al. 2014]. Interestingly, in association with active bowel disease, family history of IBD, appendectomy, cigarette smoking, they are potential risk factors for arthritis in IBD patients [Manguso et al. 2004, 2005]. Acute anterior uveitis, aortic insufficiency and cardiac conduction disturbances are described with a frequency of 25%, 4–10% and 3–9%, respectively [Peluso et al. 2014]. They seem to be related to disease duration, axial joint involvement and to HLA-B27 positivity [Bergfeldt, 1997]. In addition, some data clearly suggest that IBD patients, as well as those with SpA [Di Minno et al. 2012a; 2012b], show an increased cardiovascular and thrombotic risk [Yarur et al. 2011]. A frequent occurrence of metabolic syndrome is also documented in IBD, particularly in ulcerative colitis (UC) [Yorulmaz et al. 2011]. Finally, renal and/or urinary involvement occurs in a range between 4 and 23%, and urolithiasis is the most common urogenital manifestation (12–28%) [Oikonomou et al. 2011].
The target of therapy in the management of arthritis associated with IBD is to reduce the inflammation and to prevent the disability and/or deformity; this requires an active cooperation between gastroenterologist and rheumatologist. Nevertheless, when IBD and SpA coexist, the therapeutic strategy should be modulated, taking into account the variable manifestations of IBD in terms of intestinal and extra-intestinal features, and the clinical manifestations of SpA with particular attention to peripheral enthesitis and dactylitis [Olivieri et al. 2014].
The aim of this review is to provide a fair summary of current treatment options for the arthritis associated with IBD.
Methods
PubMed (National Library of Medicine) was the main electronic database that was searched, using the search terms ‘arthritis’ and ‘spondyloarthritis’ in combination with ‘treatment’. Similar separate searches were made with ‘Crohn’s disease’ and ‘ulcerative colitis’ in combination with ‘treatment’ to ensure that no articles were missed. Search limits included links to full text only, humans, English language articles, males and females, and all adult ages. The ‘Related Articles’ function of PubMed was used to crosscheck for any additional relevant studies. There was no restriction set on how far back the literature was cited, but the studies that were generated were primarily from the 1980s to the present. Titles and abstracts identified in the broad search were examined, and the studies were included in the review if they were directly relevant to IBD and one of the trigger areas. Retrieved articles were also reviewed for relevant citations. Research studies published only in abstract form were excluded. Finally, each article was then reviewed for quality and clinical relevance.
Management of axial involvement
The treatment of axial involvement in SpA has focused on the combination of exercise with nonsteroidal anti-inflammatory drugs (NSAIDs) (Table 1) [Dougados et al. 2002]. Traditional NSAIDs or selective COX-2 inhibitors (COXIBs) improve spinal pain and stiffness in the axial subset, although radiographic progression ankylosis may occur. Nevertheless, considering the activity of the intestinal disease in IBD patients, the use of traditional NSAIDs should be avoided in the treatment of axial symptoms, due to the probability of exacerbation of bowel inflammation, particularly in UC patients [Kaufman et al. 1996]. Likewise, therapy with COXIBs is not recommended because there are no data about their use in active IBD. Theoretically, COXIBs could have deleterious effects on the bowel in patients with IBD [O’Brien, 2000], but some studies have shown that COXIBs improve the severity of experimental colitis and the endoscopic relapse compared with placebo [Smale et al. 2001; Sandborn et al. 2006]. Despite the worry of a potential worsening of bowel inflammation with NSAIDs or COXIBs, rheumatologists have used these drugs successfully in patients with IBD. However, if symptoms and/or signs of bowel inflammation develop or worsen during the use of NSAIDs or COXIBs treatment it is prudent to discontinue their use [Voulgari, 2011]. As a consequence, in order to manage joint symptoms, these drugs are recommended for patients with mild exacerbations but their use should be limited to the lowest effective dose and only for short periods of time.
Therapy of arthritis associated with inflammatory bowel disease (IBD).
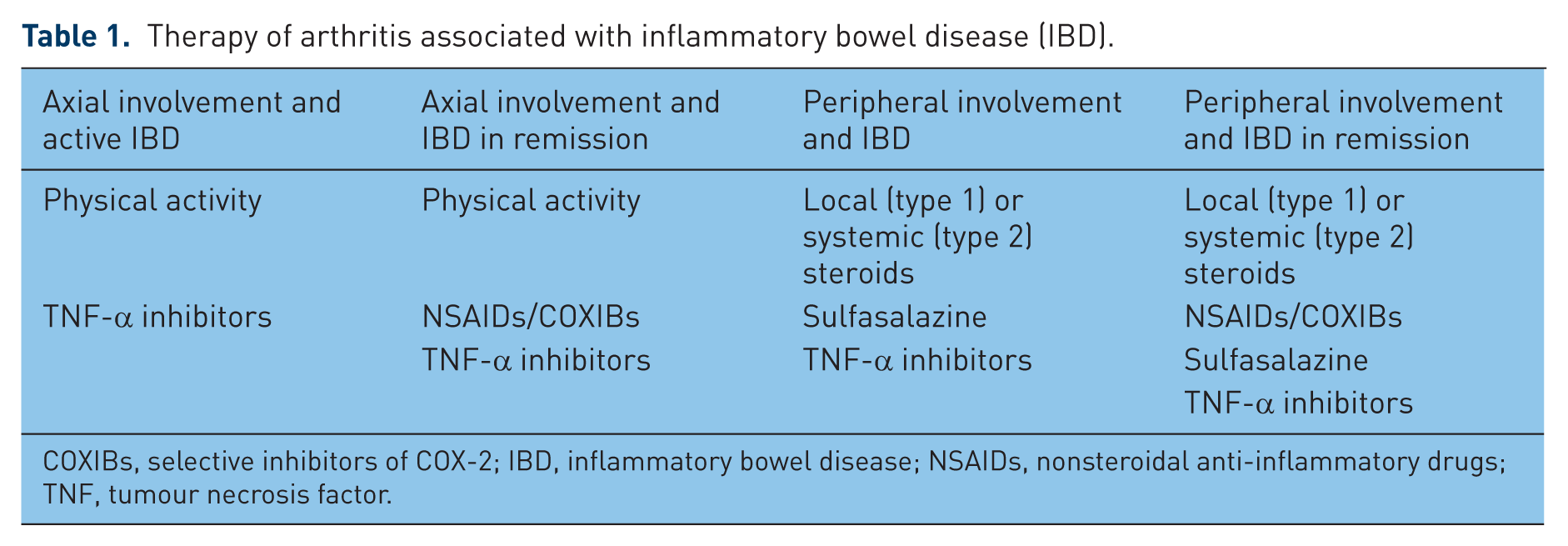
COXIBs, selective inhibitors of COX-2; IBD, inflammatory bowel disease; NSAIDs, nonsteroidal anti-inflammatory drugs; TNF, tumour necrosis factor.
Rest and physical therapy have been indicated as important additional treatments in the therapy of spondylitis in IBD patients. Physical therapy is important to improve the spinal mobility and to prevent deformities of the spine with subsequent respiratory compromise and disability. Breathing exercises, spinal exercises and swimming should be preferred. However, a recent systematic review showed that there is limited evidence to indicate that controlled physical therapy may be better than individualized home programs [Dagfinrud et al. 2005].
Corticosteroids are used in short-term treatment or intermittent pulsing therapy at large doses in moderate-to-severe nonresponsive cases of IBD [Dignass et al. 2010], but they are often ineffective in controlling axial symptoms of spondylitis [Braun et al. 2011].
Sulfasalazine has been shown to be useful both in the chronic management treatment of bowel disease and in flare-ups of UC, but the effectiveness on Crohn’s disease (CD) is not well proven [Nikfar et al. 2009]. Sulfasalazine has no effect on the evolution of joint damage to severe forms of arthritis and its usefulness in the axial subset is marginal. In fact, in a combined analysis of patients with SpA, sulfasalazine produced better treatment response rates, compared with placebo, in patients with peripheral arthritis than in those with exclusively axial disease [Clegg et al. 1999]. Finally, sulfasalazine does not seem to prevent the possible onset of intestinal inflammation in patients with SpA [Ferraz et al. 1990]. An earlier report indicated that the sulfapyridine component of sulfasalazine is responsible for the drug’s toxicity such as cyanosis, transient reticulocytosis, frank hemolysis and vomiting [Das et al. 1973]. Regarding serious blood disorders, there has been an earlier report of neutropenia due to sulfasalazine [Hopkinson et al. 1989]. In addition, sulfasalazine-associated thrombocytopenia has been reported in arthritis patients [Farr et al. 1989; McKenna and Burrows, 1994]. Finally, Ransford and colleagues reported that interstitial nephritis and pancreatitis constituted only the 3% of reports for sulfasalazine [Ransford and Langman, 2002].
Methotrexate, the second most commonly used immunosuppressive agent for IBD, has been used as an effective treatment in CD [van Dieren et al. 2006], but the evidence is less robust in UC, for which results of supplementary studies are pending (METEOR in Europe and MERIT in the United States of America) [Carbonnel, 2011]. With regard to axial involvement, efficacy is not well recognized. Responses to methotrexate in spondylitis have shown a modest efficacy in peripheral subsets, with little improvement noted in axial involvement [Ostendorf et al. 1998]. Recently, in a study conducted on AS patients who received oral methotrexate at a dose of 10 mg weekly or placebo for 24 weeks, methotrexate did not result in any significant improvement in the disease activity scores or spinal metrology scores compared with patients receiving placebo [Roychowdhury et al. 2002]. A potential new indication of methotrexate in EA could be combination therapy with tumor necrosis factor (TNF) α inhibitors, but data in the literature are lacking and further studies are needed. Interestingly, several gastroenterologists prefer subcutaneous administration for the potential erratic oral bioavailability in CD; however, there is very little on specific methotrexate bioavailability data in CD. Finally, methotrexate is thought to be safe and tolerable. Nausea can occur in 15% of patients, but can typically be prevented by co-administration of folate. Leukopenia, hepatotoxicity, hypersensitivity pneumonitis and opportunistic infections have been reported but are uncommon. Methotrexate is teratogenic and should never be used in pregnant women or those contemplating pregnancy [Regueiro, 2000; Feagan and Alfadhli, 2004]. The incidence of hepatotoxicity of methotrexate in patients with IBD is thought to be significantly lower than that in patients with other SpA. Although methotrexate-induced hepatotoxicity can occur in patients with IBD, this risk is likely low in properly selected patients (not obese, regular alcohol users, having fatty liver or other pre-existing liver disease).
With regard to other immunomodulators, azathioprine, 6-mercaptopurine, cyclosporine and leflunomide have been efficacious in patients with peripheral arthritis and other extra-intestinal manifestations [De Keyser et al. 2000; Haibel et al. 2005], but they are not effective for the treatment of axial symptoms of spondylitis. However, these results should be interpreted with caution because there are not controlled studies that have confirmed their efficacy; these data belong to uncontrolled studies or case reports. Moreover, dose-independent or hypersensitivity reactions have been described with use of these drugs. In particular, hepatitis, pneumonitis, arthritis and fever have been reported in IBD patients treated with azathioprine and 6-mercaptopurine. Perhaps the most serious dose-independent reaction is pancreatitis, occurring in 4% of patients [Chaparro et al. 2013]. This side effect generally occurs early in the course of therapy and typically resolves with discontinuation of the drug. Minor side effects such as nausea, vomiting and flu-like illness are possible and typically well tolerated in most IBD patients [Cummings et al. 2008]. Serious opportunistic infections are possible, as with any immunosuppressant agents, but are uncommon [Katz, 2005; Khan et al. 2011]. With regard to the development of cancer, and in particular of lymphoma, following the use of these therapies, a recent meta-analysis [Kandiel et al. 2005] concluded that IBD-patients have a four-fold increased risk of lymphoma, but whether this increase was due to the medication or to the underlying disease could not be established.
Cyclosporine is generally considered to be less safe than other IBD therapies because of the risk of serious side effects such as anaphylaxis, seizure, pneumocystis carinii pneumonia and permanent nephrotoxicity [Katz, 2005]. Moreover, potential easy use is limited by the need for close monitoring of drug serum levels because there is a narrow gap between the therapeutic and the toxic ranges [Cohen et al. 1999]. Therefore, cyclosporine is typically reserved as a rescue agent for severe, refractory disease.
TNF-α inhibitors have been proven to be highly effective in the treatment of IBD patients who are steroid-dependent or refractory to conventional therapy, and in patients with associated articular manifestations. Therefore, in active but not complicated CD associated with axial involvement, therapy with TNF-α inhibitors is recommended, excluding etanercept, which has been reported to be ineffective in CD [Sandborn et al. 2001]. Moreover, etanercept is a possible triggering factor for new onset of CD [Haraoui and Krelenbaum, 2009]. Indeed, a recent meta-analysis showed that, compared with infliximab, etanercept is rarely, although more frequently, associated with IBD activity in patients affected by AS [Braun et al. 2007]. However, etanercept has been demonstrated to be effective in the treatment of joint symptoms in IBD patients [Marzo-Ortega et al. 2003].
Infliximab is the best studied among TNF-α inhibitors in IBD; it is strongly effective in moderate-to-severe CD and UC, promoting fistula closure, mucosal healing and sparing use of steroids [Present et al. 1999; Hanauer et al. 2002; Sandborn et al. 2009]. There is also evidence that infliximab is effective for axial involvement in EA [van den Bosch et al. 2000; Herfarth et al. 2002; Generini et al. 2004]. Induction and maintenance doses for infliximab should be those that are effective for both diseases: 5 mg/kg at weeks 0, 2 and 6, and then every 8 weeks [Dignass et al. 2010; Orlando et al. 2011].
Adalimumab is also efficacious in inducing and maintaining remission in moderate-to-severe CD [Devlin and Panaccione, 2008] and in treatment of spondylitis [van der Heijde et al. 2006; Lichtiger et al. 2010]. Adalimumab was described to be useful against the short- and long-term effects on disease signs and symptoms in AS. Moreover, in patients with axial involvement, a reduction of signs and symptoms of sacroiliitis is also described with its use. The efficacy of adalimumab in AS is mainly sustained by the results of a recent multicenter study that showed that the response for most patients treated with adalimumab was better than that observed in patients treated with placebo [Lichtiger et al. 2010]. No published studies have addressed yet the effect of switching from infliximab to adalimumab in EA [Atzeni et al. 2009]. Induction and maintenance doses should be effective for both diseases: 160 mg at week 0, 80 mg at week 2 and then 40 mg every 2 weeks [Dignass et al. 2010; Orlando et al. 2011].
Golimumab has been demonstrated to be effective in the improvement of sign and symptoms in patients with AS [Inman et al. 2008] and in maintaining clinical response in patients with moderate-to-severe active UC [Sandborn et al. 2014]. Its safety profile was consistent with that reported for other TNF-α inhibitors. Moreover, AS patients treated with golimumab, with no syndesmophytes and less systemic inflammation at baseline, had considerably less radiographic progression [Braun et al. 2014].
Patients with axial involvement, in a persistent and stable remission, have a high probability of relapse of articular disease; in these patients TNF-α inhibitors should be continued [Braun et al. 2011; van der Heijde et al. 2011]. The possibility of reducing TNF-α inhibitors doses according to SpA treatment recommendations [Braun et al. 2011; van der Heijde et al. 2011] may be considered in CD patients with prolonged and stable clinical, radiological, endoscopic and biochemical remission [Olivieri et al. 2014]. Moreover, TNF-α inhibitors should be started when NSAIDs are insufficient to control axial symptoms. The choice of a specific TNF-α inhibitor should be influenced by the possible effect on underlying IBD [Olivieri et al. 2014].
While there are several studies on novel biologics in the treatment of other SpA, data for the use of these agents in EA are lacking. Although certolizumab is approved for the treatment and the maintenance of response in moderate-to-severe CD with an inadequate response to conventional therapy in the US, there are no data on its utility in the therapy of EA. The recommended dosing for induction is 400 mg subcutaneously at weeks 0, 2 and 4, and then every 4 weeks for maintenance of response. Studies evaluating the efficacy of infliximab, adalimumab and certolizumab have usually shown similar results but no studies have directly compared these agents. Preliminary data suggest that certolizumab can be effective in patients who respond to infliximab and then become nonresponders or intolerant to it [Hanauer et al. 2010; Sandborn et al. 2010].
Ustekinumab has been demonstrated to have clinical efficacy in CD and may be useful in patients refractory to infliximab [Sandborn et al. 2008]. Abatacept was in theory useful in IBD, but a preliminary study evaluating this drug in CD patients was stopped because of a lack of efficacy [Mozaffari et al. 2014]. Rituximab has demonstrated to be useful in the treatment of RA patients and it is theorized to be effective in IBD. Nevertheless, there are some case reports where worsening or development of IBD during rituximab treatment has been reported [Goetz et al. 2007; Ardelean et al. 2010]. Tocilizumab has been demonstrated to have clinical efficacy in RA patients who do not respond to TNF-α inhibitors [Genovese et al. 2008]. Although interleukin-6 (IL-6) may be important for healing mucosal lesions in the gut [Tebbutt et al. 2002], tocilizumab is associated with intestinal ulcers and perforation [Nishimoto et al. 2010] and therefore cannot be recommended as an ideal choice for treatment of EA. Natalizumab and vedolizumab were effective in the treatment of moderate-to-severe active CD and UC [McLean et al. 2012; Sakuraba et al. 2013], but have not been studied in SpA.
The use of biologics is generally considered to be safe and tolerable. However, a risk–benefit analysis should be undertaken when considering their potential for serious complications [Peluso et al. 2013a]. The immunosuppressive effect of currently used biologic agents leads to an increased risk of specific infections during therapy. Most commonly, these infections arise from the upper respiratory tract and the urinary tract. In a recent study on CD patients treated with biologics, an infectious adverse event occurred in about 40% of patients. Less than 3% of patients showed a serious infectious adverse event [Colombel et al. 2007]; severe infections during TNF-α inhibitor therapy include the reactivation of latent tuberculosis [Sanduzzi et al. 2012]. These patients should be treated with chemoprophylaxis (e.g. isoniazid for 6 months, during which TNF-α inhibitors can be introduced). Moreover, the development of antibodies to infliximab or to adalimumab is frequently observed in patients treated with biologics. It was associated with a shorter duration of response to therapy and a higher rate of infusion reactions [Baert et al. 2003]. The overall percentage of infusion reactions with TNF-α inhibitors was 6.1% and included a burning sensation, itching, erythema and pain, while injection site reactions, attributed to local irritation, were observed in about 4% [Colombel et al. 2007; Sandborn et al. 2007].
TNF-α plays a role in apoptosis and tumor suppression; it is believed that interference with these pathways can potentially lead to an increased risk of malignancies. The odds ratio for all types of cancer was 3.3 in a pooled analysis of both CD and RA patients receiving TNF-α inhibitors [Bongartz et al. 2006]. Neurological disorders following treatment with TNF-α inhibitors have been described. In a review of the Adverse Events Reporting System of the United States of America Food and Drug Administration (FDA), 90 cases of demyelinating events were reported following administration of TNF-α inhibitors [Mohan et al. 2001]. Abnormal liver function, such as cholestatic disease and hepatitis-like syndromes, are associated with TNF-α inhibitor treatment [Menghini and Arora, 2001; Moum et al. 2007]. Mildly elevated liver enzymes do occur and stopping TNF-α inhibitor treatment is recommended when these increases exceed three times the upper limit of normal in the case of alanine aminotransferase. Abnormal liver function tests generally return to normal after discontinuation of TNF-α inhibitor therapy. Moreover, this therapy can lead to an increase in the rate of heart failure with an increased risk of death. Therefore, its use is contraindicated in patients with class III–IV New York Heart Association congestive heart failure.
Management of peripheral involvement
The treatment of peripheral oligo-articular involvement (type 1) and/or enthesitis and/or dactylitis is based on local steroid injections, while sulfasalazine and/or low doses of systemic steroids may be useful in cases of inadequate response to intra-articular steroids (Table 1) [Ritchlin et al. 2009; Gossec et al. 2012]. Moreover, as oligo-articular involvement can parallel the course of bowel disease, treatment of IBD may resolve the arthritis. In fact, in UC patients, colectomy may be an effective treatment for IBD and may be efficacious also for articular involvement, in particular for type 1 peripheral arthritis. Nevertheless, there are case reports of arthritis developing de novo after proctocolectomy for UC, particularly with ileo-pouch anal anastomosis, in the setting of pouchitis [Balbir-Gurman et al. 2001; Abi Karam et al. 2003].
NSAIDs and COXIBs, with a short-term course (no more than 2 weeks), are usually prescribed to control peripheral arthritis (type 1 and 2) in quiescent IBD, but their use should be avoided in case of active bowel disease. Moreover, low doses of both systemic steroids and COXIBs may be considered as a ‘bridge therapy’ to oral sulfasalazine [Olivieri et al. 2014]. It is important to remember that steroids are not indicated to maintain remission from IBD. Additionally, intra-articular steroid injection into the affected joints provides rapid but only temporary relief.
The choice of disease-modifying antirheumatic drugs (DMARDs) depends on the activity of IBD and their efficacy in the management of articular manifestations should be considered.
Sulfasalazine induces only a little improvement in peripheral arthritis (type 1 and 2). It is better when used in patients with active bowel disease and if they are employed in UC rather than CD. Consequently, sulfasalazine (2–3 g/day) is indicated in the case of mild-to-moderate IBD with peripheral articular involvement and early disease (<5 years) in cases of failure of local injections of steroids [Olivieri et al. 2014]. Aminosalicylates were found to be of little benefit for peripheral arthritis and enthesitis [Thomson et al. 1994]. Moreover, sulfasalazine or mesalazine should be continued regardless of other systemic treatments used, considering their efficacy in maintaining clinical remission [Sutherland and Macdonald, 2006] and their possible chemopreventive effect on colorectal cancer [Velayos et al. 2006].
Immunomodulators such as methotrexate, azathioprine, cyclosporine and leflunomide show their efficacy in some patients with peripheral arthritis (type 1 and 2) and other extra-intestinal components [De Keyser et al. 2000; Padovan et al. 2006; Peluso et al. 2013b]. Methotrexate has greater utility in CD than in UC for gut inflammation; further evaluation is ongoing in two randomized multicenter trials (METEOR in Europe and MERIT in the United States of America) [Carbonnel, 2011]. Methotrexate, which has longstanding use in RA, may be beneficial for arthropathy in IBD as well as for IBD itself. Recently, our research group has been studying the efficacy and the tolerability of methotrexate at a dose of 20 mg/week in patients with peripheral arthritis under UC. We have shown a rapid and effective reduction of joint symptoms with significant improvement in laboratory parameters and in rates of disease activity [Peluso et al. 2009].
Many rheumatologists use methotrexate in patients with IBD and peripheral arthritis. Moreover, methotrexate can be preferred to azathioprine, but this is an empirical approach not based on trial evidence [Williams et al. 2008]. Orally administered methotrexate is adequately absorbed, even in patients with active IBD. Subcutaneous injection of the drug can reduce gastrointestinal side effects.
TNF-α inhibitors have been found to be highly effective for IBD patients who are steroid dependent or refractory to conventional treatments, particularly for CD, and they are useful in patients with associated articular involvement [van den Bosch et al. 2000; Generini et al. 2004; Rispo et al. 2005].
Infliximab, an important progress in the treatment of IBD with or without concomitant arthropathy [Barrie and Regueiro, 2007], rapidly improves peripheral arthritis in IBD patients. At the beginning of the 2000s some authors reported, in open-label studies, an improvement in peripheral arthritis in IBD patients treated with infliximab at 5 mg/kg; these patients had previously been refractory to steroids, 6-mercaptopurine, azathioprine or methotrexate [Ellman et al. 2001; Herfarth et al. 2002; Kaufman et al. 2005].
In the following years, Generini and colleagues confirmed that infliximab has been proven to be highly effective on the inflammation of the entheses and of periarticular structures in patients with CD, contemporarily inducing and maintaining the remission of bowel disease. Consequently, infliximab has a good efficacy on all the articular manifestations of the disease, in addition to the well-known positive effect on IBD [Generini et al. 2004]. Recently, a randomized controlled study confirmed infliximab as an effective therapy for bowel manifestations in UC patients with moderate–severe intestinal disease. There are no data about its efficacy on articular manifestations in course of UC [Jarnerot et al. 2005]. Therefore, on the basis of available data, it seems that most IBD patients with active intestinal inflammation and concurrent peripheral arthritis are likely to experience an improvement in their joint symptoms after receiving infliximab.
The efficacy of adalimumab in the treatment of inflammatory rheumatic disease such as RA, SpA and AS is well known, but no published studies have yet addressed the effect of switching from infliximab to adalimumab in patients with CD and associated arthritis. Recently, in a study on CD patients having associated arthritis who discontinued infliximab (because of intolerance or loss of efficacy) the clinical response to adalimumab was evaluated: it successfully controlled both articular and intestinal disease activity [Jarnerot et al. 2005].
Etanercept can control the arthritis associated with CD, but it has no effect on bowel disease itself [Marzo-Ortega et al. 2003]. There are no data on the efficacy of golimumab and other novel biologic agents in the treatment of peripheral arthropathy associated to IBD.
In conclusion, TNF-αinhibitors should be considered the first-line therapeutic approach when moderate-to-severe luminal CD or UC are associated with polyarthritis (Table 2). The choice of a specific TNF-α inhibitor should be influenced by the possible effect on underlying bowel disease. In cases of severe activity of UC, the patients should be hospitalized and treated with systemic intravenous steroids and infliximab as rescue therapy [Monterubbianesi et al. 2014] in association with a daily consultation with a surgeon [Olivieri et al. 2014]. Moreover, in cases of prolonged and stable remission for patients with both peripheral and intestinal manifestations, given the high probability of articular involvement relapse, TNF-α inhibitors should be continued [Olivieri et al. 2014]. The possibility of reducing TNF-α inhibitor doses according to SpA treatment recommendations [Braun et al. 2011; van der Heijde et al. 2011] may be taken into account in CD or UC patients with prolonged and stable clinical, radiological, endoscopic and biochemical remissions [Olivieri et al. 2014].
When to start treatment with TNF-α inhibitors.

BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C-reactive protein; DMARDs, disease-modifying antirheumatic drugs; ESR, erythrocyte sedimentation rate; MRI, magnetic resonance imaging; NSAIDS, nonsteroidal anti-inflammatory drug; TNF, tumour necrosis factor.
Conclusion
Although arthropathy is a common feature in patients with IBD, there are few studies specifically examining the treatment of arthritis in IBD. Therefore, the management of patients with SpA requires active cooperation between gastroenterologist and rheumatologist. The use of corticosteroids and/or DMARDs and/or of TNF-α inhibitors, helpful to contain intestinal inflammation, usually also leads to the reduction of peripheral type 1 arthritis symptoms, which also respond well to rest, to physical therapy and to local steroid injections. On the contrary, the management of types 2 and 3 is more complex and they may persist despite the reduction of IBD. Our experience suggests that the majority of patients respond promptly to anti-inflammatory drugs, useful to control joint and entheses inflammation [Peluso et al. 2013b]. However, they do not stop the development of joint damage and, at the same time, they may also be responsible for important side effects on the bowel, such as the exacerbation of IBD. As a consequence, in order to manage joint symptoms, these drugs are recommended for patients with mild exacerbations but their use should be limited to the lowest effective dose and only for short periods of time. Sulfasalazine is often used for the treatment of IBD and its effectiveness is also confirmed for the management of mild peripheral arthritis, particularly in patients with UC [Dissanayake and Truelove, 1973]. Its effectiveness in CD has not yet been well proven. These drugs have no effect on the evolution of joint damage to severe forms of arthritis and their usefulness in the axial subset is marginal; they do not seem to prevent the possible onset of bowel inflammation in patients with SpA [Ferraz et al. 1990]. Immunomodulators such as methotrexate, azathioprine, cyclosporine and leflunomide show their efficacy in some patients with peripheral arthritis and other extra-intestinal components [De Keyser et al. 2000; Padovan et al. 2006; Peluso et al. 2013b]. TNF-α inhibitors are highly effective in the treatment of SpA [Atteno et al. 2010; Baraliakos and Braun, 2012; Bruner et al. 2014]. In IBD patients, they have been shown to be successful in moderate-active disease, not only against IBD but also for the SpA component (axial and peripheral), and particularly in patients with CD, although these drugs show several side effects [Peluso et al. 2013a]. Finally, advances in the understanding of the molecular basis of CD and UC have led to the development of promising new biologic therapies, which will likely be studied further both as monotherapeutic agents, and for use in combination with immunomodulators.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.