
Abstract
Immunosuppressive therapy is frequently used to treat gastrointestinal diseases such as inflammatory bowel disease, autoimmune hepatitis, IgG4-related disease (autoimmune pancreatitis and sclerosing cholangitis) and in the post-transplantation setting. These drugs interfere with the immune system. The main safety concern with their use is the risk of infections. Certain infections can be prevented or their impact minimized. Physicians must adopt preventative strategies and should have a high degree of suspicion to recognize infections early and treat appropriately. This article reviews the risk factors for infections, the mechanism of action of immunosuppressive therapy and proposes preventive strategies.
Keywords
Introduction
Immunosuppressive therapy (IMT) is the cornerstone of treatment in many gastroenterological diseases, most notably inflammatory bowel disease (IBD), autoimmune hepatitis and in the post-transplantation setting, and more recently IgG4-related disease (autoimmune pancreatitis and sclerosing cholangitis) [Rahier et al. 2009; Talley et al. 2011; Rostaing et al. 2012; Manns et al. 2010; Culver and Chapman, 2011]. In this context, the most frequently used immunosuppressive drugs are corticosteroids, thiopurines (azathioprine and mercaptopurine), methotrexate, calcineurin inhibitors (tacrolimus and cyclosporine) and antitumor necrosis factor agents (infliximab and adalimumab). These drugs can increase the risk of infectious complications, an important safety concern when prescribing IMT. Prevention of infection is a key management strategy, which includes recognition of risk factors, monitoring for clinical symptoms, attention to laboratory results, vaccination where possible and patient education [Vermeire et al. 2010]. In this article, we will review measures to prevent bacterial, viral, fungal and parasitic infections associated with IMT. Our review focuses on the literature from IBD but also studies from hepatology, dermatology and rheumatology. The diagnosis and treatment of infection is beyond the scope of this article.
Infections associated with IMT
The infections associated with IMT are presented in Table 1. A clear association between certain infections and certain drugs may be linked to their mechanism of action and the immune profile (Table 2).
Infections associated with immunosuppressive therapy. (Adapted from Aberra and Lichtenstein [2005].)
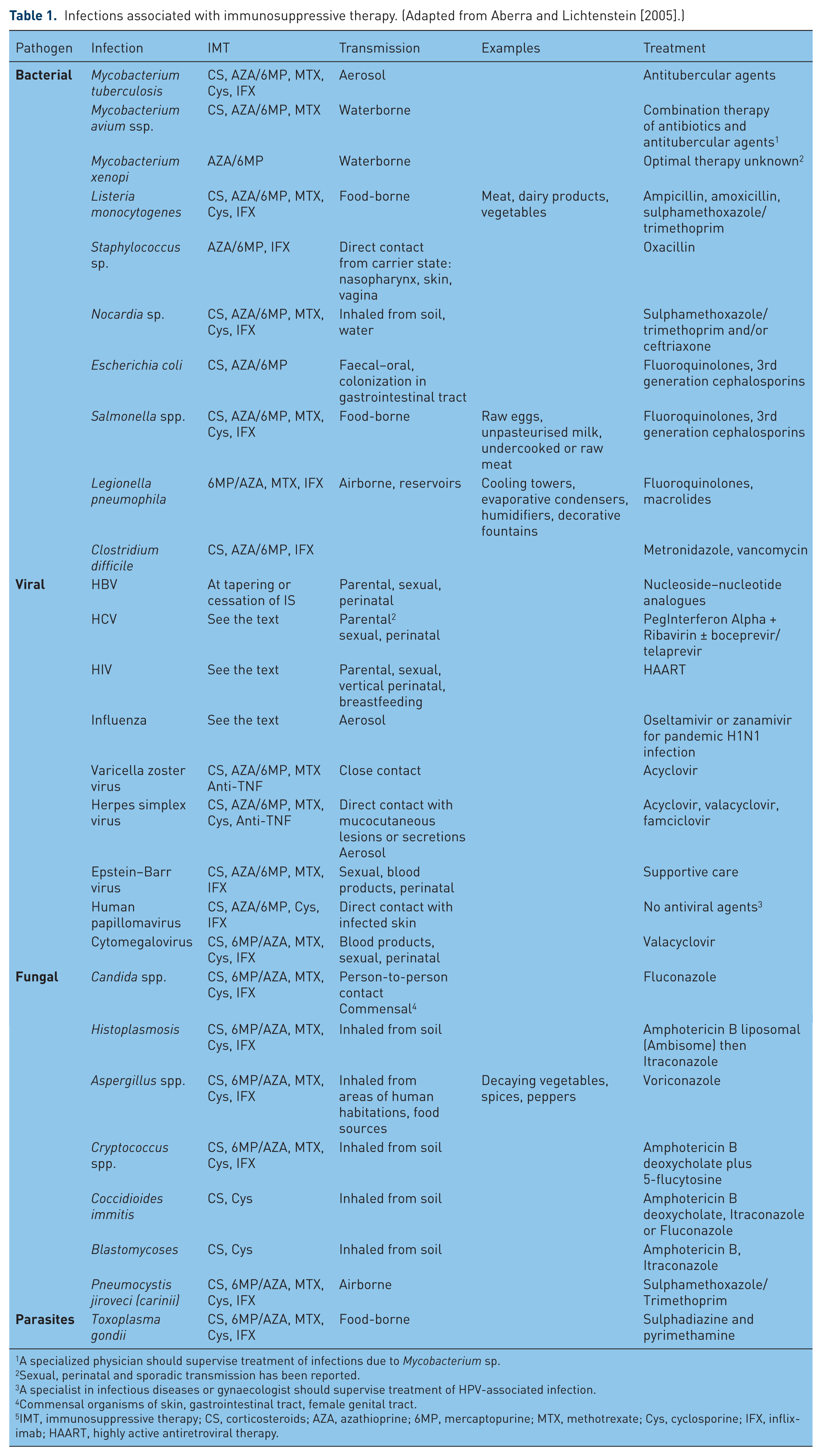
A specialized physician should supervise treatment of infections due to Mycobacterium sp.
Sexual, perinatal and sporadic transmission has been reported.
A specialist in infectious diseases or gynaecologist should supervise treatment of HPV-associated infection.
Commensal organisms of skin, gastrointestinal tract, female genital tract.
IMT, immunosuppressive therapy; CS, corticosteroids; AZA, azathioprine; 6MP, mercaptopurine; MTX, methotrexate; Cys, cyclosporine; IFX, infliximab; HAART, highly active antiretroviral therapy.
Mechanism of action of immunosuppressive agents.
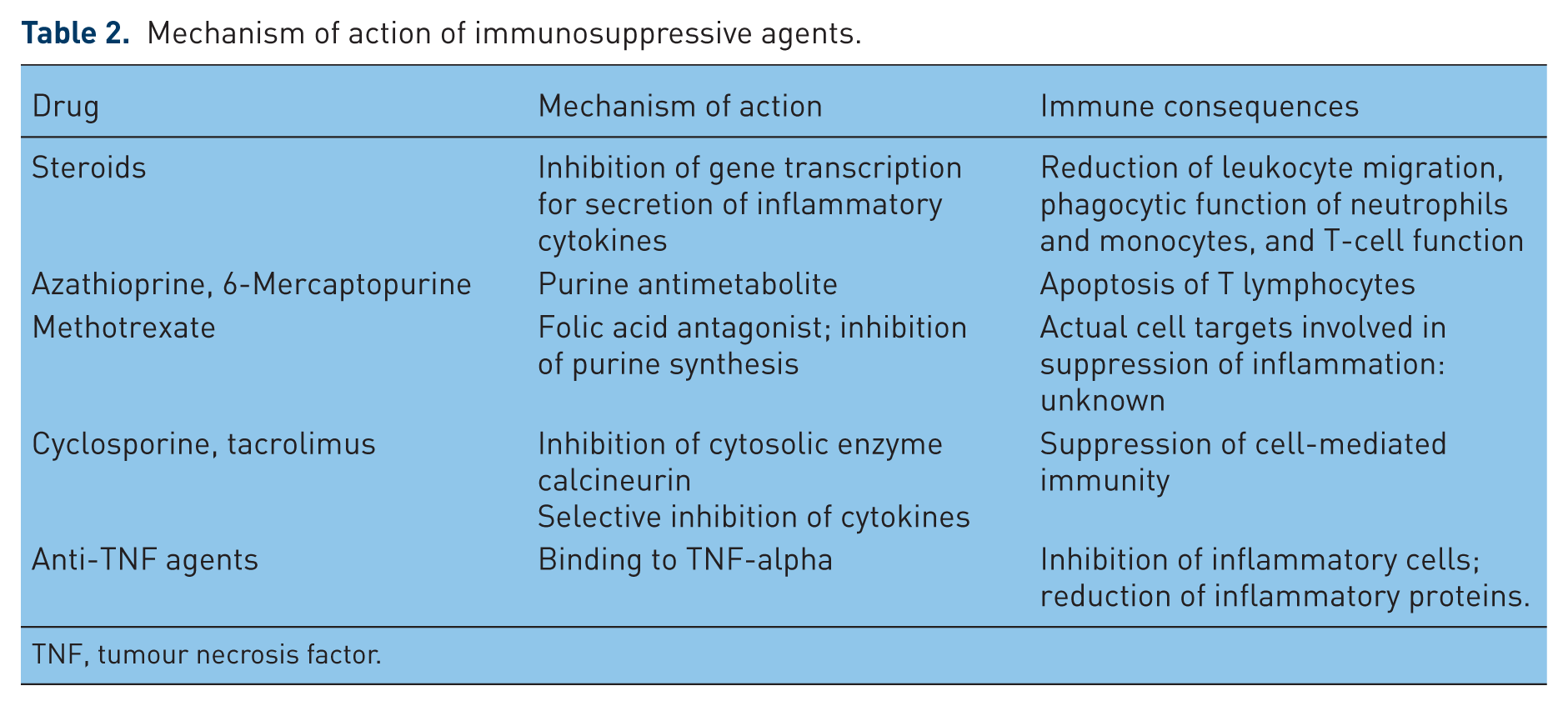
TNF, tumour necrosis factor.
Corticosteroid use is associated with a broad spectrum of infectious complications. In one of the largest meta-analyses of pooled data from 71 controlled clinical trials (4198 patients with various diseases), the overall rate of steroid-associated infectious complications was 12.7% in those randomly allocated to corticosteroids compared with 8% in those receiving placebo (relative risk [RR] 1.6, 95% confidence interval [CI] 1.3–1.9, p < 0.001) [Stuck et al. 1989]. In subgroup analysis, the risk of infection was significantly higher in those with intestinal disease (RR 1.4, p = 0.02) but not with hepatic disease (RR 1.4, p = 0.25). The risk of infection can depend upon dose, duration and route of corticosteroid administration and the hosts underlying disease state [Cutolo et al. 2008]. A decreased risk has been associated with a lower dose, shorter course and with night-time dosing of corticosteroids and in those with less comorbidity [Stuck et al. 1989]. Corticosteroids can blunt the typical clinical features of infection, so awareness is important. The combination of steroids and other immunosuppressive drugs increase the risk of serious and opportunistic infections [Aberra and Lichtenstein, 2005].
Azathioprine and mercaptopurine have been independently associated with many bacterial and viral infections, the risk with methotrexate is less clear [Aberra and Lichtenstein, 2005]. Regular monitoring of laboratory results in patients on thiopurines and methotrexate for leukopenia is imperative [Aberra and Lichtenstein, 2005; Levesque and Loftus, 2012]. Cyclosporine was associated with Gram-negative sepsis and pneumonia in controlled clinical trials in IBD [Aberra and Lichtenstein, 2005]. Tacrolimus has been independently associated with increased risk of fungal infections, but less risk of symptomatic cytomegalovirus infection compared with cyclosporine post-liver transplantation [Hoppe et al. 2006; Alessiani et al. 1991]. Anti-tumour necrosis factor (anti-TNF) therapy has been associated with upper respiratory infections, abscesses, staphylococcal sepsis, pneumonia, urinary tract infection, cutaneous Nocardiasis and Listeria monocytogenes [Aberra and Lichtenstein, 2005]. In a large cohort of patients with rheumatoid arthritis receiving anti-TNF, the long-term risk of serious infections was 23.7/1000 patient-years (95% CI 13.1–34.2) on adalimumab and 65.1/1000 patient-years (95% CI 48.4–81.8) on infliximab [Atzeni et al. 2012]. In a controlled trial of 100 patients with IBD the odds ratio (OR) for opportunistic infection with infliximab was 4.4, and increased significantly when combined with corticosteroids and azathioprine or mercaptopurine [Toruner et al. 2008]. Concomitant use of steroids and advanced age at the start of anti-TNF therapy are significant predictors of infection [Atzeni et al. 2012; Toruner et al. 2008].
Bacterial infections
Prevention of specific bacterial infections
Clostridium difficile infection
Clostridium difficile is a Gram-positive anaerobic spore-forming bacillus. It secretes two pathogenic toxins: A (enterotoxin) and B (cytotoxin). C. difficile-associated disease (CDAD) usually presents with diarrhoea, abdominal pain, fever and leukocytosis. Risk factors to acquire C. difficile and develop CDAD include antibiotics, IMT, nursing home residence and hospitalization [Martinez et al. 2012]. Corticosteroids are associated with significantly increased mortality in patients with CDAD [Das et al. 2010]. Thiopurines, methotrexate and infliximab have all been associated with an increase in CDAD in patients with IBD, especially in those taking 2 immunosuppressive agents [Badger et al. 2012]. Prevention of C. difficile centres upon good hand hygiene: handwashing with soap as mechanical friction eliminates spores. If CDAD is suspected or diagnosed, patients should be isolated to avoid transmission. Healthcare workers should wear disposable gloves and gowns and rooms should be decontaminated with hydrochlorite solutions [Martinez et al. 2012; Badger et al. 2012]. Routine screening for C. difficile is not recommended before initiating IMT nor is chemoprophylaxis [Rahier et al. 2009]. However, in patients admitted with an exacerbation of known colitis, a history of prior antibiotic use should be taken, C. difficile screening should always be performed and treatment commenced if there is a high degree of suspicion. Data is limited and conflicting in the role of probiotics in preventing CDAD, thus routine prescription cannot be recommended [Na and Kelly, 2011].
Streptococcus pneumonia
Streptococcus pneumonia is a Gram-positive facultative anaerobic coccus. Pneumonia and meningitis are the most severe manifestations of pneumococcal infections. Risk factors for infection include IMT, age over 65 years, smoking and chronic diseases [Pitsiou and Kioumis, 2011]. Pneumococcal infections can be prevented with vaccination. The most commonly used vaccines are nonconjugated polysaccharide (Pneumovax 23® and Pneumo 23®). European Crohn’s and Colitis Organisation (ECCO) guidelines recommend vaccination at least 2 weeks before initiating IMT [Rahier et al. 2009]. Antibody levels decrease over time so revaccination is recommended; one group from the United States recommend one-time revaccination after 5 years in patients with IBD [Sands et al. 2004] whereas other Spanish and Belgian groups recommend it every 3–5 years [Vermeire et al. 2010; Esteve et al. 2009]. Conjugated vaccines have recently been licensed (Prevnar®/Prevenar®, Synflorix®) [Pitsiou and Kioumis, 2011]. These are more effective in preventing pneumococcal infections in children and in the elderly, although they cover fewer serotypes than the nonconjugated vaccines. Routine administration in the adult population is yet to be determined.
Listeria and Salmonella
Listeriosis is a bacterial infection caused by a Gram-positive motile bacterium. It occurs in those who are immunocompromised, in the elderly and newborn infants. Salmonellosis is an infection with Salmonella bacteria, which can cause diarrhoea, fever, vomiting and abdominal cramps from 12 to 72 hours after infection and can persist for 4–7 days; the immunocompromised are more likely to develop severe illness [Culver and Travis, 2010]. Prevention consists of food hygiene, mainly by avoiding raw eggs, unpasteurized milk, insufficiently cooked or raw meat and raw vegetables [Rahier et al. 2009].
Legionella pneumophila
Legionella is a pathogenic Gram-negative bacterium that can cause severe infection in the immunocompromised and elderly. Regular cleaning of water systems such as humidifiers avoids Legionella pneumophila infection [Rahier et al. 2009].
Tuberculosis
Tuberculosis (TB) is caused by Mycobacterium tuberculosis and is one of the world’s most common fatal infections. It typically manifests as pulmonary TB; the majority of cases resulting from reactivation of latent infection [World Health Organization, 2011]. Risk factors for reactivation are close contact with infectious persons, radiographic evidence of untreated TB, malnutrition and smoking [Horsburgh and Rubin, 2011]. Corticosteroids (prednisolone at a dose ≥15mg/day or equivalent) and anti-TNF agents are both responsible for an increased risk of reactivation. In a national prospective observational study the event rate of TB was 144 per 100,000 patient-years for adalimumab and 136 per 100,000 patient-years for infliximab; the majority of cases were extrapulmonary (62%) [Dixon et al. 2010]. Nonwhites had a sixfold higher risk of TB compared with whites treated with anti-TNF therapy.
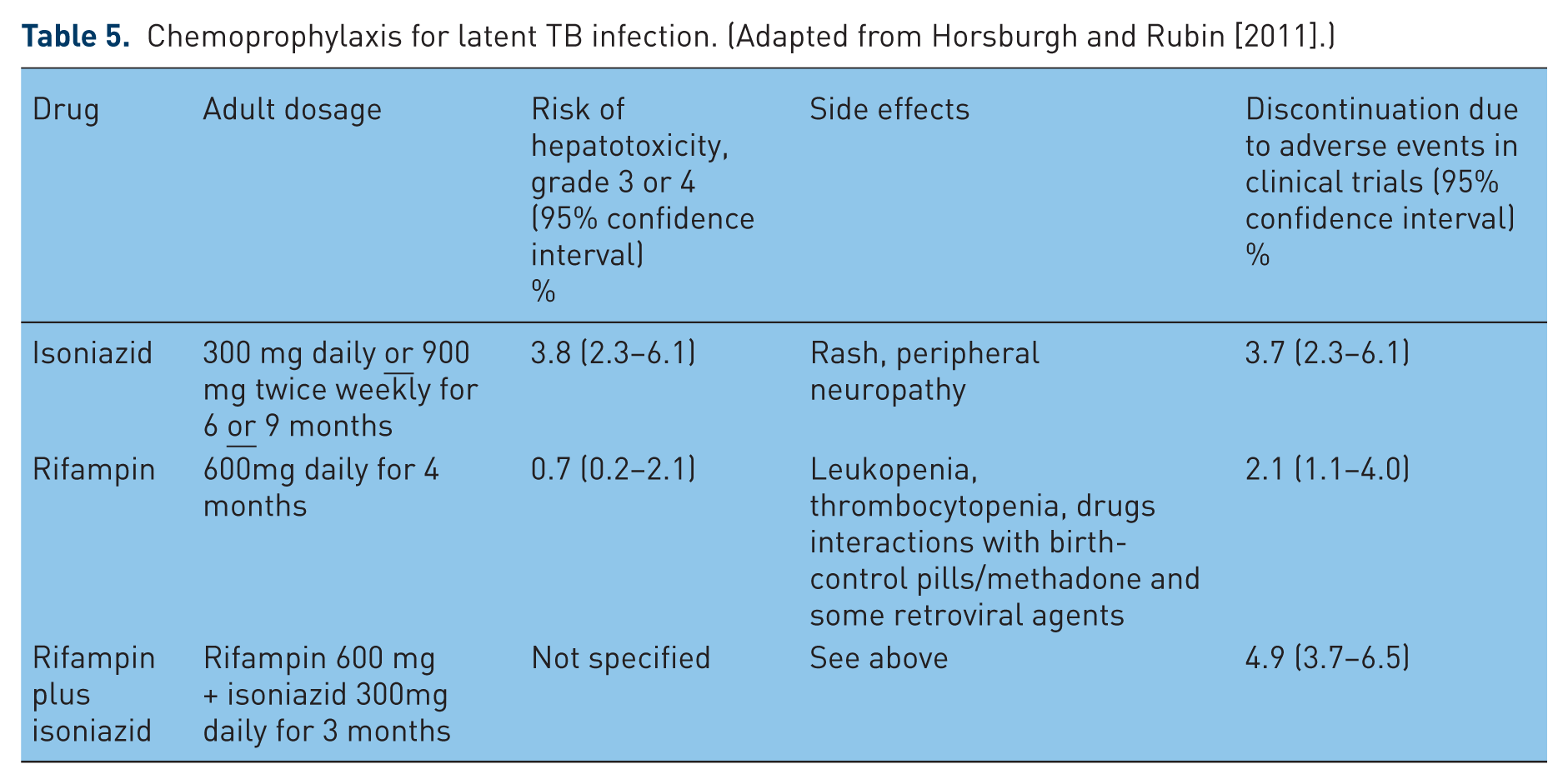
All patients should be evaluated to determine risk of latent or active TB when considering IMT (Table 3). Patients are at increased risk for developing active disease and becoming infectious if they have latent TB, despite the absence of overt symptoms [Mazurek et al. 2010]. There are local variations in the use of tuberculin skin testing (TST) or interferon-gamma-release assays (IGRAs), part of the screening protocol for TB (Table 4). Testing should be performed prior starting IMT as both rely on an intact immune response. IGRA is more specific but less sensitive than a standard TST in predicting future active disease [Horsburgh and Rubin, 2011; Mazurek et al. 2010]. A positive diagnosis of latent TB is established in those with appropriate risk factors and a positive TST or IGRA with no evidence of active TB clinically and on chest X-ray (CXR). The risk of TB needs to be balanced against the risk of adverse effects of chemoprophylaxis with isoniazid or rifampicin (Table 5). ECCO guidelines recommend that if latent TB is present, anti-TNF should be delayed for at least 3 weeks after starting chemoprophylaxis and infectious diseases specialist advice sought [Rahier et al. 2009]. One group from East Anglia have audited the impact of TB screening in areas of low TB incidence in 339 patients with rheumatoid arthritis taking anti-TNFs [Pradeep et al. 2009]. A tuberculin test was done in 81 patients (24%), 238 (92%) had a CXR and 15 (4.4%) needed specialist referrals. Six of 10 patients with suspected latent TB received chemoprophylaxis before starting IMT. None of these patients have had TB reactivation. When applying screening algorithms, 30 additional tuberculin tests, 26 CXRs and 4 specialist referrals should have been done. They concluded that adhering to guidelines may be an unnecessary practice in areas where TB prevalence is low. More studies are needed before validating this approach.
Identification of patients at increased risk of tuberculosis.

TB, tuberculosis; BCG, bacille Calmette–Guérin; TST, tuberculin skin testing; IGRA, interferon gamma-release assay.
Screening guidelines for tuberculosis (TB) from the United States, Canada and the United Kingdom. (Adapted from Horsburgh and Rubin [2011].)

For example, homelessness or injected-drug use.
VIH, persons using immunosuppressive therapy such as prednisolone or anti-TNF
The sources for the US, Canadian and UK guidelines are Centers for Disease Control and Prevention (CDC), the Public Health Agency of Canada and the UK National Institute for Health and Clinical Excellence, respectively.
TST, tuberculin testing skin; IGRA, interferon-gamma-release assays; BCG, bacille Calmette–Guérin.
Chemoprophylaxis for latent TB infection. (Adapted from Horsburgh and Rubin [2011].)
Viral infections
Certain human viral infections have a benign course, some cause chronic viral infections (e.g. hepatitis B and C) whilst others stay in a latent form after a primary infection (e.g. varicella zoster).
Specific viral infections
Hepatitis B virus infection
Hepatitis B virus (HBV) is a hepatotropic DNA virus with variable worldwide geographical distribution; prevalence is low in Western Europe, Canada and the United States [Teshale, 2012]. Reactivation of HBV replication has been reported in 20–50% of patients receiving IMT or cancer chemotherapy; it usually occurs at tapering or cessation of IMT or anti-TNFs [Lok and McMahon, 2009]. Clinical presentation varies from subclinical hepatitis to potentially fatal liver failure. Patients at risk are those with a positive HBV surface antigen (HBsAg) and those who are HbsAg-negative HBV core antibody (anti-HBc)-positive. Corticosteroids, thiopurines, methotrexate and calcineurin inhibitors result in low levels of immunosuppression and are infrequently associated with HBV reactivation [Morisco et al. 2011; Gisbert et al. 2011]. Several cases have been reported with infliximab in patients with Crohn’s disease; reactivation occurring after the first infusion and up to 2 years after commencing infliximab [Gisbert et al. 2011; Shale et al. 2010]. Most have occurred in the context of combination therapy with thiopurines or corticosteroids. A few cases have also been described with adalimumab [Abramson et al. 2012; Matsumoto et al. 2010; Verhelst et al. 2010].
Universal screening for HBV is recommended in all patients before initiating IMT (as recommended by ECCO and American Association for the Study of Liver Diseases [AASLD]) as targeted screening is difficult to implement and can miss infected patients who do not recognize or report risk factors [Rahier et al. 2009; Lok and McMahon, 2009; European Association for the Study of the Liver, 2012]. High-risk groups include persons born in high or intermediate endemic areas, persons with chronically elevated aminotransaminases, men who have sex with men, persons with multiple sexual partners or history of sexually transmitted disease, inmates of correctional institutions, intravenous drug users, HIV- or hepatitis C virus (HCV)-infected individuals and contacts (family, sexual partners) of persons infected by HBV.
Screening tests should include HBsAg, anti-HBc and HBV surface antibody (anti-HBs) to assess infection and vaccination status. ECCO and AASLD guidelines recommend vaccination to all seronegative patients [Rahier et al. 2009; Lok and McMahon, 2009]. Ideally, vaccination should occur before initiating IMT, which can reduce immunogenicity following vaccination. If patients are already on IMT, vaccination should be given and testing for serological immunity is recommended 1–2 months after administration of the vaccines last dose. Anti-HBs concentration of ≥10 mIU/ml is considered as a reliable indicator of protection against infection [Gisbert et al. 2011]. Revaccination should be considered in nonresponders to initial vaccination with an additional dose, a second three-dose course or even double the standard dose. Prophylactic antiviral therapy with nucleotide/nucleoside analogues has been proven effective in patients undergoing chemotherapy for cancers. It reduces the rate of HBV reactivation, severity of associated hepatitis flares and mortality [Lok and McMahon, 2009]. Prophylactic antiviral therapy is recommended in the guidelines produced by ECCO, AASLD and the European Association for the Study of the Liver (EASL) for patients who are HBsAg-positive and due to start on, or who are currently on, IMT (Table 6). Patients who are HBsAg-negative/anti-HBc-positive should be monitored with aminotransferase and HBV-DNA levels regardless of anti-HBs status. Antiviral therapy should be introduced when HBV-DNA levels become detectable.
Prevention guidelines of HBV in the context of immunosuppressive therapy (according to the most recent guidelines from ECCO, EASL and AASLD).

Owing to the risk of drug resistance associated with long-term lamivudine use.
Interferon-alpha may exacerbate Crohn’s disease and cause additional bone marrow suppression; could be considered in ulcerative colitis.
EASL recommends up to 12 months after cessation of IMT.
EASL recommends prophylaxis indefinitely in patient with liver grafts.
EASL recommends monitoring ALT and HBV-DNA every 1–3 months depending on the type of IMT and comorbidities.
HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; IMT, immunosuppressive therapy; ALT, alanine transaminase
HCV infection
HCV is a hepatotropic RNAvirus affecting 2–3% of the world’s population and0.2–3.5% of the European population [World Health Organization, 2010a]. No consensus has been reached for HCV screening before the introduction of IMT and therefore screening of selected patients with a history of exposure to the virus and testing those with an identifiable risk factor, as suggested by the AASLD guidelines, is generally adopted. Risk factors include intravenous drug use, blood transfusions and organ transplants pre-1992, haemophiliacs receiving blood products pre-1987, those on haemodialysis, those born to HCV-infected mothers, those with HIV, those with infected sexual partners or multiple partners and elevations of alanine aminotransferase that are unexplained [Ghany et al. 2009].
Studies reporting liver transplant recipients who had HCV infection indicate that thiopurines and methotrexate can be used without detrimental effect. Corticosteroids should be tapered slowly to limit the risk of early recurrent HCV hepatitis. Anti-TNF therapy seems to have no adverse effects [Rahier et al. 2009; Gisbert et al. 2011; Shale et al. 2010]. There are no reports of acute HCV infection occurring during anti-TNF treatment. No vaccine or chemoprophylactic therapies are available. Avoiding exposure to infection is the best prevention.
HIV infection
HIV is part of the human retrovirus family. It affects almost 0.5% of the European and Canadian population [World Health Organization, 2010b]. Highly active antiretroviral therapy (HAART) has dramatically improved the outcome of patients infected by HIV. Data is limited as for the use of IMT in HIV. Studies from renal transplantation in HIV-positive patients indicate that corticosteroids increase CD4 population and decreases HIV viral load [Natario et al. 2012]. Calcineurin inhibitors have well-documented antiretroviral effects while azathioprine is associated with increased viral replication [Natario et al. 2012]. Small clinical studies assessing the impact of anti-TNFs on the course of HIV infection report no worsening of infection with the use of infliximab [Rahier et al. 2009; Culver et al. 2010]. There are no reports of acute HIV infection whilst on conventional IMT or anti-TNF therapy.
ECCO guidelines recommend testing for HIV active infection by HIV p24 antigen and antibody, prior to immunomodulators and anti-TNF agents [Rahier et al. 2009]. However, blanket HIV testing before immunosuppression has not been widely adopted and many physicians will base HIV screening upon risk factors, such as sexual behaviour and intravenous drug use. Patient education to reduce HIV transmission should be given, such as condom use and not sharing needles. Post-exposure prophylaxis is appropriate for health professionals. If active infection is diagnosed, treatment is best discussed with a specialist in HIV but HAART should be started before IMT.
Influenza virus
Influenza infection is characterized by the onset of fever and tracheobronchitis. Immunocompromised patients are generally considered at increased risk of influenza and at higher risk of complicated infection [Beck et al. 2011]. In the event of infection, preventive measures include maintaining good respiratory hygiene, washing hands frequently and staying at home to avoid spread. Vaccination is often underutilized in immunocompromised patients. In a German cohort of IBD patients treated with immunomodulators only 19% were vaccinated against influenza, the most common reasons being lack of awareness (45%) and fear of side effects (17%) [Wilckens et al. 2011]. Numerous studies have evaluated the safety of influenza vaccines in patients taking IMT for rheumatic disease, solid organ transplantation and IBD. Heterogeneity across studies limits generalization, but most immunocompromised patients achieve protective antibody titres. Immunogenic responses vary depending on the immunosuppressive agent or regimen administered. Post-vaccination protection was the lowest with anti-TNF agents in combination with other immunosuppressive agents [Agarwal et al. 2012].
Influenza vaccine can be given in the form of injectable trivalent inactivated or intranasal live attenuated vaccine [Kelso, 2012]. The former contains killed virus or viral subunits that cannot cause influenza infection and is therefore safe in immunocompromised patients and recommended yearly in most guidelines (Table 7). The WHO declared a pandemic outbreak of human swine-origin influenza A (H1N1) virus in 2009, against which seasonal influenza vaccine does not protect. Reported cases of resistance to oseltamivir, an antiviral drug used as treatment, since emerged [Renaud et al. 2011]. Studies looking at the immunogenicity and safety of the pandemic influenza vaccine in immunocompromised suggest its safety [Manuel et al. 2011; Felldin et al. 2012]. Patients receiving IMT are advised to receive the appropriate vaccine as soon as it is available and some authors suggest giving two doses [de Lavallade et al. 2011]. Monitoring of serological response to the vaccine is not recommended.
Travel-related infections and preventive measures in patients on immunosuppressive agents. (Adapted from Esteve et al. [2011]. Information revised on the CDC website.)
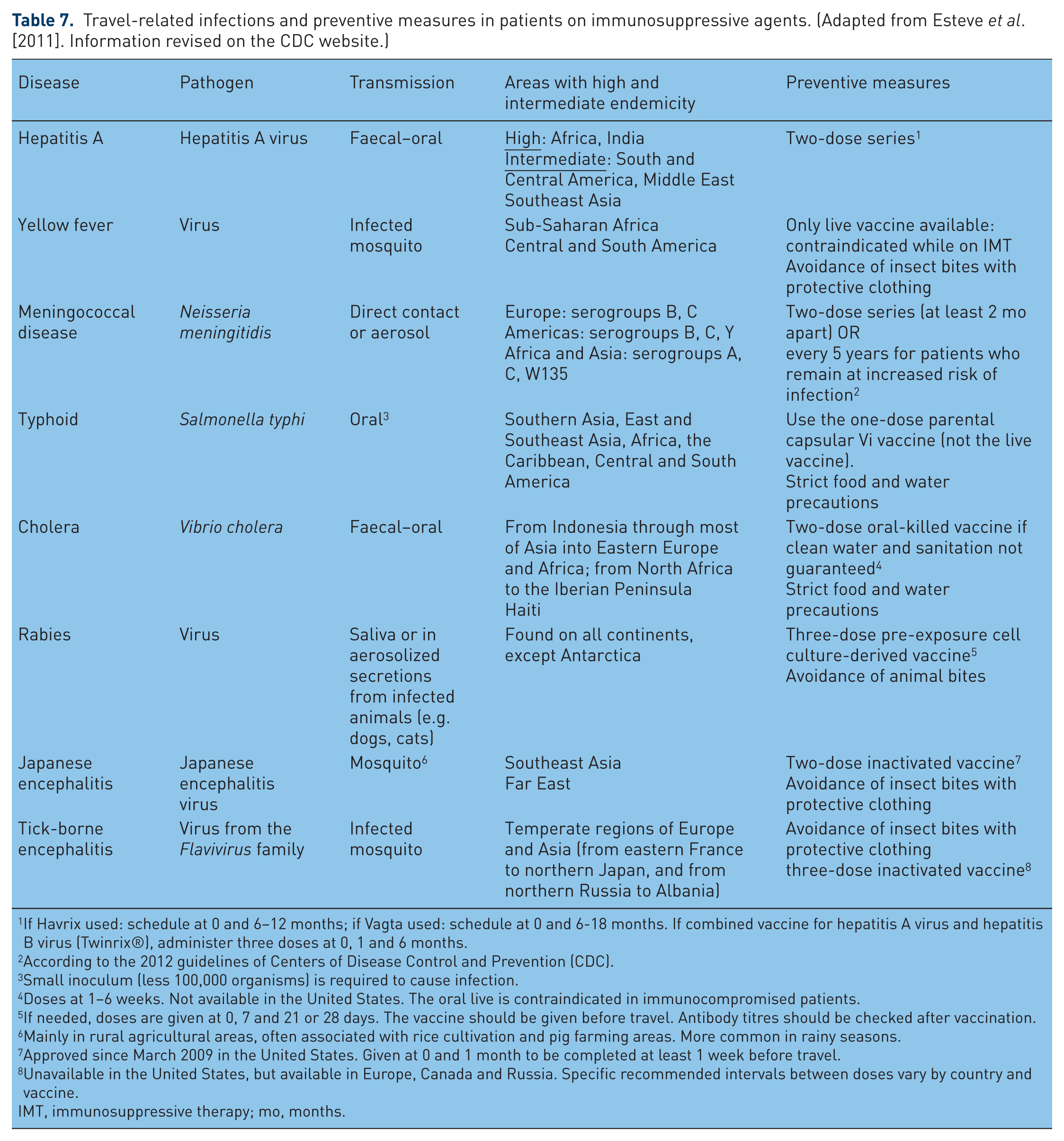
If Havrix used: schedule at 0 and 6–12 months; if Vagta used: schedule at 0 and 6-18 months. If combined vaccine for hepatitis A virus and hepatitis B virus (Twinrix®), administer three doses at 0, 1 and 6 months.
According to the 2012 guidelines of Centers of Disease Control and Prevention (CDC).
Small inoculum (less 100,000 organisms) is required to cause infection.
Doses at 1–6 weeks. Not available in the United States. The oral live is contraindicated in immunocompromised patients.
If needed, doses are given at 0, 7 and 21 or 28 days. The vaccine should be given before travel. Antibody titres should be checked after vaccination.
Mainly in rural agricultural areas, often associated with rice cultivation and pig farming areas. More common in rainy seasons.
Approved since March 2009 in the United States. Given at 0 and 1 month to be completed at least 1 week before travel.
Unavailable in the United States, but available in Europe, Canada and Russia. Specific recommended intervals between doses vary by country and vaccine.
IMT, immunosuppressive therapy; mo, months.
Varicella zoster virus infection
Primary infection with varicella zoster virus (VZV) causes chickenpox, characterized by vesicular cutaneous lesions and fever. Reactivation of latent VZV results in herpes zoster virus (HZV), producing a painful, vesicular dermatomal rash [Sampathkumar et al. 2009]. Immunocompromised patients and those over the age of 50 years old are at higher risk [Thomas and Hall, 2004]. Immunosuppression increases the risk of disseminated disease, chronic mucocutaneous infection and can lead to HZV encephalitis, pneumonia, hepatitis and death [Wauters et al. 2012]. Anti-TNF therapy is a particularly important risk factor; in a prospective cohort of patients with rheumatoid arthritis in Germany, the incidence of HZV was 11.1/1000 patient-years for anti-TNF therapy compared with 5.6 /1000 patient-years for conventional immunomodulators [Wendling et al. 2008; Strangfeld et al. 2009; García-Doval et al. 2010]. Older age and corticosteroid use were also risk factors [Strangfeld et al. 2009]. In a prospective 3-year French RATIO registry of patients receiving anti-TNFs, 18/45 (40%) reported infections were viral of which 8 were severe VZV [Salmon-Ceron et al. 2011].
Two methods are advocated to prevent complicated VZV infection: post-exposure passive antibody prophylaxis in the form of varicella zoster immunoglobulin (VZIG) and active vaccination. If an unimmunized patient has had close contact with a person with chicken pox or herpes zoster, VZIG should be given within 96 hours of exposure. The individual must be carefully observed over the next 4 weeks for evidence of clinical infection, and immediate antiviral therapy should be started with specialist advice [Rahier et al. 2009]. The vaccine uses a live attenuated form of VZV and most recent guidelines from the Centers for Disease Control and Prevention (CDC) recommends avoiding it in immunocompromised patients (Table 8) [Centers for Disease Control and Prevention, 2012]. Nevertheless, active immunization with a two-dose series of live varicella vaccine is advised by ECCO, at least 3 weeks before introducing IMT. ECCO recommend vaccination in individuals only if the medical history of chickenpox, shingles and VZV vaccination is negative [Rahier et al. 2009]. In adults with no history of VZV or prior immunization, serologic testing is not required before administration of zoster vaccine [Harpaz et al. 2008]. If IMT is discontinued, a 3-month period is needed before administrating live vaccines except for corticosteroids where 1 month is sufficient [Rahier et al. 2009, 2010].
Vaccination summary for immunocompromised patients. (Adapted from Centers for Disease Control and Prevention [2012] and Rahier et al. [2009, 2010].)

Contraindications apart from severe allergic reaction (e.g. anaphylaxis) after previous dose of any influenza vaccine or to a vaccine component.
According to the Sands et al. [2004] and the Centers for Disease Control and Prevention [2012].
According to Vermeire et al. [2010] and Culver and Travis [2010].
According to Centers for Disease Control and Prevention [2012].
Immunocompromised patients generally include patients with known severe immunodeficiency from haematological and solid tumours, receipt of chemotherapy, congenital immunodeficiency, long-term immunosuppressive therapy or patients with HIV infection who are severely immunocompromised. Significant immunosuppressive steroid dose is considered to be ≥2 weeks of daily intake of 20 mg or 2 mg/kg of prednisone or equivalent.
The Food and Drug Administration (FDA) licensed the zoster vaccine (one-dose vaccine) for adults ≥50 years of age; the Advisory Committee on Immunization Practices (ACIP) recommends that vaccination start at 60 years of age.
According to Centers for Disease Control and Prevention [2012]. The second dose can be given 1–2 months after the first dose; the third should be given 6 months after the first.
If Havrix used: schedule at 0 and 6–12 months; if Vagta used: schedule at 0 and 6–18 months. If combined vaccine for HAV and HBV (Twinrix), administer 3 doses at 0, 1 and 6 months.
IMT, immunosuppressive therapy; IC, immunocompromised; IBD, inflammatory bowel disease; HIV, human immunodeficiency virus; HBV, hepatitis B virus; HAV, hepatitis A virus.
Herpes simplex virus
Herpes simplex virus (HSV) infection affects 60–95% of human adults, causing a self-limited oral–labial (HSV type 1) or genital (HSV type 2) infection. HSV remains in a latent form in the nerve root ganglia and IMT can reactivate it. Clinical presentation ranges from recurrent oral or genital lesions to encephalitis [Fatahzadeh and Schwartz, 2007]. The rash may be atypical [Wendling et al. 2008]. Corticosteroids and azathioprine may trigger infection; in a prospective cohort of patients with IBD, azathioprine was associated with a fivefold increased risk of HSV lesions (p = 0.04) [Seksik et al. 2009]. Corticosteroids, azathioprine and cyclosporine have also been used to treat herpes-associated erythema multiforme (HAEM) [Fatahzadeh and Schwartz, 2007]. In a prospective French RATIO registry, 3 out of the 18 (17%) viral infections were due to HSV [Salmon-Ceron et al. 2011]. The number of reported cases and complications of HSV infection in the context of anti-TNFs and other agents, such as methotrexate, has increased [Sciaudone et al. 2011; Bradford et al. 2009; Justice et al. 2008; Wiland et al. 2002].
Prevention of HSV can be achieved by avoiding exposure to mucocutaneous lesions and using appropriate barrier techniques [Fatahzadeh and Schwartz, 2007]. Given that reactivation runs a benign course and severe infection remains rare, screening for latent HSV in immunocompromised patients is not recommended in the ECCO guidelines. There is no vaccine against HSV and chemoprophylaxis is unnecessary. In cases of recurrent and severe oral or genital infection, prompt oral antiviral therapy is recommended and specialist advice should be sought. Some experts suggest daily oral antiviral treatment [Rahier, 2012].
Epstein–Barr virus
Epstein–Barr (EBV) infects more than 90% of the world’s population and seropositivity increases with age. Primary infection is often asymptomatic or causes self-limiting infectious mononucleosis (glandular fever). EBV remains latent in circulating B cells thereafter. Severe complications of mononucleosis include upper-away obstruction, haemolytic anaemia and thrombocytopenia, which may be abated using corticosteroid therapy [Luzuriaga and Sullivan, 2010].
Fatal mononucleosis has been reported in IBD patients taking thiopurines; two of these patients were on dual IMT also taking corticosteroids for disease [Posthuma et al. 1995; Garrido Serrano et al. 2000; N’guyen et al. 2009]. Azathioprine has been associated with EBV hepatitis, mucocutaneous ulcers and hemophagocytic syndrome [Angelucci et al. 2011; McGinness et al. 2012; Dojcinov et al. 2010; Fitzgerald et al. 2012]. Infliximab, but not adalimumab, has been linked to severe complications of EBV infection or atypical presentations [Ueda et al. 2010; Sari et al. 2009; Colaci et al. 2011]. EBV infection been implicated in the pathogenesis of lymphoma, sarcoma and carcinoma in immunocompromised individuals [Thompson and Kurzrock, 2004]. In a Dutch national study looking at the relative risk of malignant lymphoma in IBD patients, 92% of patients with EBV-positive lymphoma (11/12 patients) used a thiopurine in contrast to only 19% with EBV-negative lymphoma [Vos et al. 2011]. The risk of lymphoma associated with the combination of anti-TNFs and thiopurines is difficult to establish.
There is no vaccine available for EBV. Screening and chemoprophylaxis is not recommended be-cause reactivation is usually asymptomatic and self-limited and the contribution of EBV in the development of lymphoma remains to be determined.
Human papilloma virus
Human papilloma virus (HPV) is a common sexually transmitted infection. The infection can be low risk, associated with anogenital warts or mild dysplasia, or high risk, associated with cervical or anal neoplasia [Munoz, 2000; Munoz et al. 2003]. Immunosuppressed post-transplant patients and those infected with HIV are considered at increased risk for developing benign and malignant anogenital tumours mediated by HPV [Gormley and Kovarik, 2012]. It is unclear whether these tumours are related to new acquisition of HPV infection or reactivation. Women with a history of exposure to IMT were more likely to have an abnormal cervical smear in one prospective controlled trial of patients with IBD [Kane et al. 2008]. Thiopurines and cyclosporine have been linked with viral warts in IBD patients and organ transplant recipients [Seksik et al. 2009; Krüger-Corcoran et al. 2010]. Cases of severe HPV infections have been described in patients treated with infliximab for IBD and dermatological diseases [Georgala et al. 2012; Antoniou et al. 2008; Somasekar and Alcolado, 2004]. In general the evidence supports that thiopurines in particular increase the risk of cervical neoplasia. One case-control study of 411 women with IBD suggested that the rate of abnormal smears did not differ between IBD patients and controls and IMT had no impact on cervical dysplasia or neoplasia [Lees et al. 2009]. The real impact of IMT remains unclear as studies are inconsistent.
Prevention of HPV transmission involves barrier techniques such as condoms, although uncovered areas can still spread infection [Gormley and Kovarik, 2012]. Women receiving IMT are high-risk according to the American college of Obstetricians and Gynecologists (ACOG), requiring more frequent gynaecological examination and cervical screening compared with the general population [American Congress of Obstetricians and Gynecologists, 2009]. The college does not specify the interval. HPV screening is not recommended in either women or men prior to starting IMT. Two prophylactic vaccines are available: bivalent vaccine (Cervarix) for HPV16-18 subtypes and quadrivalent (Gardasil) for HPV6-11-16-18 genotypes [Heard, 2011]. Both protect against the high-risk genotypes 16-18 and the latter also protects against the low-risk HPV6-11. The 2012 CDC guidelines recommend either vaccinate routinely for females aged 11–12 years and between 13 and 26 years if missed at an earlier stage, and also for males of the same age group. Only the quadrivalent vaccine has been approved for males. The impact of HPV vaccination is yet to be determined.
Cytomegalovirus
Cytomegalovirus (CMV) infection and reactivation have been described in patients taking IMT and anti-TNFs [Aberra and Lichtenstein, 2005; Piton et al. 2008]. CMV typically causes a subclinical infection, but it can lead to hepatitis, retinitis and disseminated infection. After solid organ transplantation, chemoprophylaxis is often needed [Eid and Razonable, 2010]. Screening for CMV is not indicated before starting IMT since most disease is subclinical.
Fungal and parasitic infections
Corticosteroids have been associated with invasive fungal infections, mainly Candida sp. and Pneumocystis jirovecii infections [Cutolo et al. 2008]. One study reported 22% of fungal infections and 4% of parasitic infections in patients on anti-TNFs agents [Salmon-Ceron et al. 2011]. Combination therapy seems to increase the risk of these infections. There is no indication to screen for fungal or parasitic infections with the exception of patients returning from an endemic area or with a history of infection. No vaccines exist. Patients should be advised to avoid environmental exposure. Fungi may be found in soil or farm dust and can be associated with certain animals or birds. Parasites are commonly associated with endemic areas such as the tropics and subtropics. Pretravel counselling is recommended with specialist advice for chemoprophylaxis.
Specific fungal infections
Pneumocystis jirovecii (formerly carinii)
P. jirovecii is a unicellular fungus that may cause severe pneumonia (Pneumocystis pneumonia [PCP]) with high mortality in immunocompromised patients, especially patients with HIV/AIDS. The FDA adverse event reporting system reported more than 80 cases of PCP following infliximab and concomitant immunosuppressive agents, of which 27% died from 1998 to 2003 [Kaur and Mahl, 2007]. There is no vaccine available. There is lack of consistency among specialists in offering P. jirovecii prophylaxis to patients on IMT. ECCO guidelines recommend the use of standard prophylaxis using trimethoprim/sulfamethoxazole (cotrimoxazole) for IBD patients on triple immunosuppression, including anti-TNFs and calcineurin inhibitors; this is based on expert opinion and experience with other immunocompromised patients [Rahier et al. 2009]. A Cochrane review from 2007 concluded that prophylaxis for PCP using trimethoprim/sulfamethoxazole was not only effective, but the number needed to treat was only 15 patients [Green et al. 2007]. However, a Canadian group did not recommend prophylaxis in the non-HIV/AIDS immunocompromised population [Grewal and Brassard, 2009]. Use of prophylaxis seemingly varies between specialist centres. Optimizing the patient’s nutritional state and reducing the dose, duration and number of immunosuppressive agents helps to prevent infection.
Prevention when travelling
Frequent travel to developing countries poses specific risks to patients on IMT. The location of travel and time spent in those countries need to be considered and the risk of travel-related infections must be discussed. Some countries should be avoided such as Sub-Saharan Africa where yellow fever is endemic. Pretravel consultation with specialists in tropical medicine is advised at least 4–6 weeks before the trip to allow time for the administration of vaccines and their protective effect to begin, and to start chemoprophylaxis to prevent malaria when required [Esteve et al. 2011].
IMT is a risk factor for acquiring food- and water-borne diseases and their complications, so patients must be cautious about their source. Prevention involves using commercially bottled water or filtration, and eating well-cooked food (avoiding salads, uncooked vegetables, unpasteurized milk, cheeses, raw meat, etc.). For traveller’s diarrhoea, the threshold for initiating empirical self-treatment with antibiotics should be low. Fluoroquinolones are the first choice. Azithromycin is an alternative in cases of fluoroquinolone resistance or contraindication. Given that fluoroquinolone resistance varies in countries, the physician must verify before prescribing. For insect-borne diseases, patients should avoid outdoor exposure during the period of maximum insect activity (e.g. dengue in daylight, malaria in twilight) and wear long-sleeved shirts, long pants, boots and hats outdoors. Insect repellents are advised. When accommodation is not adequately screened or air-conditioned, pretreated and long-lasting bed nets are essential to avoid insect bites. Immunization should be offered against travel-associated infections, such as hepatitis A (Table 7). Only killed or inactivated vaccines can be safely administered while patients are on IMT [Rahier et al. 2009]. Further information about travel in specific countries can be found on the CDC website (see http://wwwnc.cdc.gov/travel/destinations/list.htm).
Vaccination
Vaccines are underutilized in immunocom-promised patients despite published guidelines recommending their use. A Scandinavian study of 102 consecutive IBD patients found that 19% were vaccinated against influenza, 3% against pneumococcus pneumonia, 22% against HBV, 5% against VZV, 55% against rubella/mumps/measles, and 63% against tetanus [Wilckens et al. 2011]. Gastroenterologists seemingly lack adequate knowledge of established immunization guidelines prior to initiation of IMT. In a Canadian survey (46% of the respondents were gastroenterologists), 14% took an immunization history, 23% did not know whether live vaccines should be avoided in immunocompromised patients and 43% did not know which specific immunizations should be avoided [Yeung et al. 2012]. As a general rule, vaccination is best checked and updated prior to the introduction of IMT (Table 8). The vaccine will be more efficient in the absence of IMT and treatment will not be delayed. Live vaccines are not contraindicated in the absence of IMT but must be given 3–4 weeks before the (re)start of therapy. If IMT is discontinued, a period of 3 months is needed before administrating live vaccines, except for corticosteroids where a waiting period of 1 month is considered sufficient [Rahier et al. 2009, 2010]. Inactivated vaccines can be given safely at anytime during immunosuppression.
Suggested work-up before initiating IMT
There are no universal recommendations in the prevention of infectious complications in the context of IMT. The present summary reflects an overview from national guidelines (Table 9). Physicians must have a high index of suspicion for infections and a low threshold for investigation and seeking specialist advice. Patient education is crucial. It includes avoidance of exposure to pathogens and providing information about symptoms of infections. Contact details for advice to patients should be considered the standard of care especially if they are treated with anti-TNF therapy. Fever is a principal symptom of infection and may be the only symptom. Therefore, patients on IMT should seek medical advice to reduce the risk of severe illness or complications.
Systematic work-up before starting IMT. (Adapted from Viget et al. [2008].)

VZV, varicella zoster virus; HSV, herpes simplex virus; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; TB, tuberculosis; BCG, bacille Calmette–Guérin; ALT, alanine aminotransferase; IMT, immunosuppressive therapy.
Conclusion
Most infectious complications related to IMT are preventable. Death due to preventable illnesses should not occur. Gastroenterologists must be aware of and implement those strategies to prevent infections due to IMT.
Footnotes
Funding
Dr. EL Culver receives a Wellcome Trust Research Fellowship Grant investigating the natural history and pathogenesis of IgG4-RD.
Conflict of interest statement
There are no conflicts of interest to disclose.