
Abstract
Interferons are cytokines with immunomodulatory properties and disease-modifying effects that have been used to treat myeloproliferative neoplasms (MPNs) for more than 35 years. The initial use of interferons was limited due to difficulties with administration and a significant toxicity profile. Many of these shortcomings were addressed by covalently binding polyethylene glycol to the interferon structure, which increases the stability, prolongs activity, and reduces immunogenicity of the molecule. In the current therapeutic landscape, pegylated interferons are recommended for use in the treatment of polycythemia vera, essential thrombocythemia, and primary myelofibrosis. We review recent efficacy, molecular response, and safety data for the two available pegylated interferons, peginterferon alfa-2a (Pegasys) and ropeginterferon alfa-2b-njft (BESREMi). The practical management of interferon-based therapies is discussed, along with our opinions on whether to and how to switch from hydroxyurea to one of these therapies. Key topics and questions related to use of interferons, such as their safety and tolerability, the significance of variant allele frequency, advantages of early treatment, and what the future of interferon therapy may look like, will be examined. Pegylated interferons represent an important therapeutic option for patients with MPNs; however, more research is still required to further refine interferon therapy.
Plain language summary
Why was this paper written? This paper was written to summarize the current clinical landscape of the use of interferons for the treatment of myeloproliferative neoplasms (MPN).
What are interferons and how are they used in MPNs? Interferons are small proteins involved in cellular signaling that have been used to treat MPNs, polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF), for more than 35 years. They can have modulatory effects on the immune system and on the fundamental causes of disease. The use of interferons as treatment was initially limited due to difficulties with their administration and the potential for significant adverse effects. Many of these shortcomings were addressed by chemically binding a biocompatible polymer, polyethylene glycol (PEG), to the structure of the interferon, which increases the stability of the protein, prolongs the time during which it is active, and reduces negative effects to the immune system. The combined chemical structure of PEG and interferon (pegylated interferon or peginterferon) is recommended for use in the treatment of PV, ET, and PMF.
What topics are discussed in this paper? In this review paper we evaluate the clinical effectiveness and safety of two available pegylated interferons, peginterferon alfa-2a (Pegasys) and ropeginterferon alfa-2b-njft (BESREMi) and discuss the practical clinical management of interferon-based therapies, along with the authors’ opinions on whether to and how to switch therapy from hydroxyurea. Key topics and questions related to the use of interferons, such as their safety and tolerability, the significance of their effects on mutated cells, advantages of early treatment, and what the future of interferon therapy may look like, will be examined.
What do the findings mean? Pegylated interferons represent an important therapeutic option for patients with MPNs; however, more research is still required to further refine interferon therapy.
Keywords
Myeloproliferative neoplasms
Myeloproliferative neoplasms (MPNs) are clonal disorders that originate from the acquisition of somatic mutations in hematopoietic stem cells (HSCs).1–4 The International Statistical Classification of Diseases and Related Health Problems (ICD) of the World Health Organization (WHO) offers the most widely used categorization of MPNs and was updated in 2022 (ICD-11) to incorporate the most recent clinical, prognostic, morphologic, immunophenotypic, and genetic data.2,5 In the WHO category of MPNs, the BCR:ABL1-negative subtypes include polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF).1,2,5,6 In the United States, incidence rates of PV, ET, and PMF reported from 2001 to 2012 are 11, 10, and 3 per 1 million person-years, respectively. 7
General information about interferons
Interferons are cytokines with immunomodulatory properties and disease-modifying effects. 8 Interferons are classified into three groups according to their structural and functional properties: IFN-type I, IFN-type II, and IFN-type III.9–11 Within IFN-type I, there are 13 IFNα subtypes (α-1, α-2, α-4, α-5, α-6, α-7, α-8, α-10, α-13, α-14, α-16, α-17, and α-21), IFNβ, IFNε, IFNκ, IFNω, IFNδ, and IFNτ.12–14 Within IFN-type II, there is only IFNγ.13,15 In addition, IFNα generally induces an apoptotic effect in several cell types and has been shown to exert an apoptotic effect on Janus associated kinase 2 (JAK2) V617F+ progenitor cells in patients with MPNs.8,16,17 However, the exact mechanism of action (MOA) in mutated HSCs is not fully elucidated. In both mouse models and in cells from patients with MPNs, IFNα induces cell cycle entry of mutated HSCs, leading to their exhaustion.16,18 In mouse models, treatment with IFNα induced monosomal karyotype/myeloid biased HSCs and reduced JAK2 V617F+ HSCs with long-term reconstitution capacities. 19 In patients with JAK2 V617F+ MPN subtypes, IFNα was found to induce both quiescence of homozygous JAK2 V617F+ HSCs and apoptosis of heterozygous JAK2 V617F+ HSCs. 20
Characteristics of interferons in clinical use
There are several interferon products currently in clinical use for the treatment of MPNs; these recombinant forms of INFα-2 include; IFN alfa-2a (Roferon-A), pegylated interferon alfa-2a (Pegasys), interferon alfa-2b (Intron-A), pegylated interferon alfa-2b (Peg-Intron), and a modified pegylated interferon alfa-2b (ropeginterferon alfa-2b-njft; BESREMi).9,21 The molecular structure of the two recombinant IFNα-2 described above (IFNα-2a and IFNα-2b) differ from one another by a single amino acid at position 23. 9 Ropeginterferon alfa-2b-njft is currently the only interferon approved for use in MPNs (i.e. PV). 21
Pharmacokinetics
Historically, clinical use of interferons has been limited due to a short half-life (requiring frequent administration) and a poor adverse effect profile.8,22,23 However, the pegylation of interferons increases their half-life, allowing for once- or biweekly administration of pegylated IFNα compared to three times weekly for IFNα.9,24,25 PegIFNα-2b (Peg-Intron) has a half-life of 54 h, PegIFNα-2α (Pegasys) has a half-life of 65 h, and ropeginterferon alfa-2b-njft (BESREMi) has a half-life of 168 h.9,21 Interferons can be administered intravenously, intramuscularly, or subcutaneously, although the majority of currently available therapies are given subcutaneously.9,21
Pharmacology
Pegylation of interferons is achieved by covalently binding polyethylene glycol to the IFNα structure.25–27 As discussed, pegylation can increase stability and solubility, prolong activity, increase half-life, and reduce immunogenicity. 9 These structural changes also result in a more tolerable toxicity profile.25,26 The random pegylation reactions used to bind polyethylene glycol to most interferons results in complex mixtures of different isoforms, each having its own activity and stability properties. 28 Ropeginterferon alfa-2b-njft has been engineered to contain two additional amino acids, including a proline at the N-terminus that allows for site-specific monopegylation. 21 This unique structure allows ropeginterferon alfa-2b-njft to exist primarily as a single isoform, which can allow for an extended dosing interval, potentially improve the safety profile, and result in fewer fluctuations in uptake or elimination.27–29 Compared to other pegylated interferons that lack this monopegylated feature, ropeginterferon alfa-2b-njft is dosed less frequently and has a similar safety profile.27–29
Pharmacodynamics
In general, interferons bind to their receptor, causing the receptors to dimerize.30–33 Receptor dimerization brings two Janus kinases into close proximity, where they can phosphorylate each other.30–35 Phosphorylated JAKs in turn phosphorylate signal transducers and activators of transcription (STATs), leading to their dimerization, translocation to the nucleus, and activation of their transcription factor activity.30–35 The binding of the STAT complex to DNA enhances the transcription of specific genes, whose protein products mediate the observed cellular responses to interferon binding.30–35 Although the exact MOA of interferons in MPNs is not fully understood, one potential mechanism is the induction of apoptosis in hematopoietic progenitors of MPN, with a preference for the mutated clone.17,36 Another proposed mechanism is through activation of the cell cycle and promotion of JAK2 VF-driven erythroid-lineage differentiation by preferentially depleting JAK2 VF MPN-propagating stem cells. 16 An overview of the potential MOA of interferons in MPNs can be found in a publication in 2020 by How and Hobbs. 37
Interferons in the current therapeutic landscape
Interferons have been used as a treatment for MPNs for over 35 years, but use of non-pegylated interferons has been limited mainly because of their significant toxicity profiles.38–41 Pegylated interferons, however, offer a more favorable toxicity profile and allow for less frequent administration.25,26 The National Comprehensive Cancer Network (NCCN) Guidelines for MPNs (Version 1.2023) recommend pegylated interferons to treat PV, ET, and PMF. 42 For PV, both peginterferon alfa-2a and ropeginterferon alfa-2b-njft are recommended as cytoreductive therapies (selected low-risk PV patients with indications for cytoreductive therapy and all high-risk PV patients with indications for cytoreductive therapy). 42 In high-risk ET and low-risk PMF, peginterferon alfa-2a is recommended as a cytoreductive therapy option. 42
Efficacy/safety of interferons in clinical trials
Interferons have been extensively studied in clinical trials of patients with MPNs. Older studies were limited by small cohorts of patients, used different interferon types and doses, had varied response criteria and short follow-up times, and therefore, diverse durability of responses. 39 Key trials are discussed here, and additional select clinical trials are summarized in Tables 1 and 2.
Summary of selected studies of pegylated interferons: efficacy and safety.

CR was defined as correction of the platelet count to <400 × 109/L, HCT to <45% without phlebotomy (for PV patients only), and WBC to <10 × 109/L; resolution of splenomegaly; and resolution of disease-related symptoms (defined as microvascular disturbances, headache, and pruritus).
CHR was defined as normalization of blood counts (essential thrombocythemia: platelets ⩽440 × 109/L; PV: hemoglobin <15.0 g/L without phlebotomy) with complete resolution of palpable splenomegaly/symptoms in the absence of a thrombotic event. A partial PR required at least a 50% reduction in the platelet count for essential thrombocythemia, or a 50% reduction in the rate of phlebotomies, or 50% reduction in spleen size by palpation for polycythemia vera.
Clinicohematologic response assessment was performed by central review according to the modified 2009 European LeukemiaNet (ET, PV, and pre-MF) and the 2005 European Myelofibrosis Network criteria (PMF).
Risk events: disease progression, death, and thromboembolic events.
Response defined as: HCT < 45% and no need for additional cytoreductive treatment.
AE, adverse event; BAT, best available therapy; CHR, complete hematological response; CMR, complete molecular response; CR, complete response; D/C, discontinuation; ET, essential thrombocythemia; HCT, hematocrit; HU, hydroxyurea; IFN, interferon; JAK, Janus kinase; PMF, primary myelofibrosis; PR, partial response; pre-MF, pre-myelofibrosis; PRV-1, polycythemia rubra vera 1 gene; PV, polycythemia vera; ropeg, ropeginterferon alfa-2b-njft; VAF, variant allele frequency; WBC, white blood cell; WHO, World Health Organization.
Summary of ongoing and future studies of pegylated interferons: efficacy and safety.
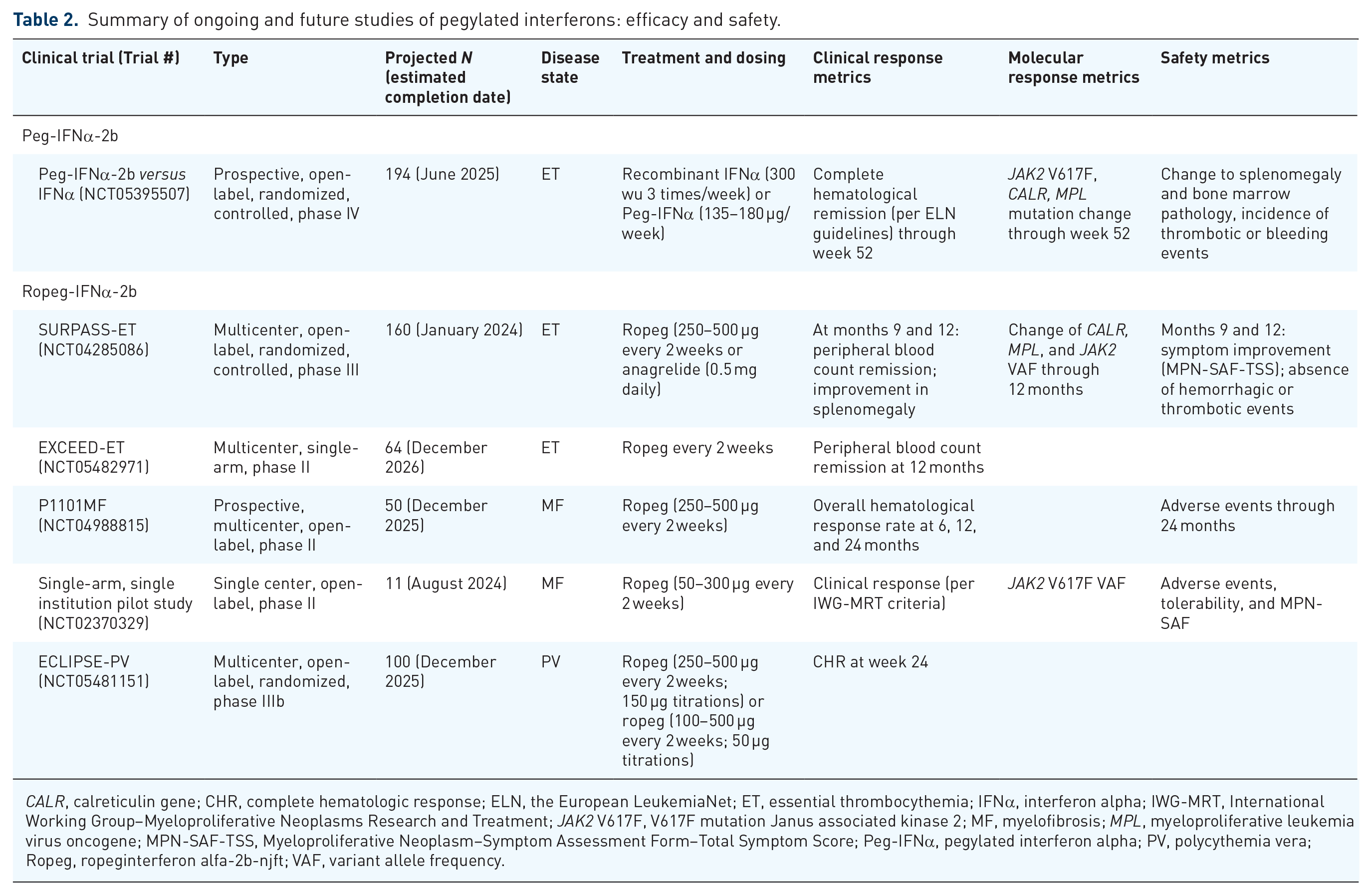
CALR, calreticulin gene; CHR, complete hematologic response; ELN, the European LeukemiaNet; ET, essential thrombocythemia; IFNα, interferon alpha; IWG-MRT, International Working Group–Myeloproliferative Neoplasms Research and Treatment; JAK2 V617F, V617F mutation Janus associated kinase 2; MF, myelofibrosis; MPL, myeloproliferative leukemia virus oncogene; MPN-SAF-TSS, Myeloproliferative Neoplasm–Symptom Assessment Form–Total Symptom Score; Peg-IFNα, pegylated interferon alpha; PV, polycythemia vera; Ropeg, ropeginterferon alfa-2b-njft; VAF, variant allele frequency.
Peginterferon alfa-2a and Peginterferon alfa-2b
In a phase II, multicenter, open-label trial (MPD-RC 111; NCT01259817), peginterferon alfa-2a was evaluated in patients (N = 115) with PV or ET who were resistant to or intolerant of hydroxyurea (HU).
43
Peginterferon alfa-2a was initially administered subcutaneously at a dose of 45 µg/week, then titrated monthly in 45 µg increments up to a maximum dose of 180 µg/week (median weekly dose 128.7 µg for patients with PV and 102.7 µg for patients with ET).
43
Complete response [CR; defined as a platelet count
In a randomized phase III study (MPD-RC 112; NCT01259856), HU (n = 80) versus peginterferon alfa-2a (n = 82) was evaluated in patients with PV or ET.
44
Peginterferon alfa-2a was initially administered subcutaneously at a dose of 45 µg/week, then titrated monthly in 45 µg increments up to a maximum dose of 180 µg/week (median weekly dose 89.4 µg).
44
HU was initiated at 500 mg twice daily.
44
After 1 year of treatment, CR (defined as a platelet count
The phase III DALIAH Study (NCT01387763) was an open-label, randomized, controlled, parallel-design trial in patients with ET, PV, pre-myelofibrosis, or PMF.47,53 Patients aged
A single center, retrospective study of patients with PV (N = 470) evaluated myelofibrosis-free survival (MFFS) and overall survival (OS).
56
Patients were treated with either recombinant interferon alpha therapy (rIFNα; recombinant interferon alpha-2a, recombinant interferon alpha-2b, or pegylated interferon alpha-2a), HU or other cytoreductive therapy (ruxolitinib, anagrelide, imatinib, dasatinib, busulfan, or combinations thereof), or received no cytoreductive treatment.
56
For low-risk patients, 20-year MFFS was 84%, 65%, and 55% in the rIFNα, HU, and no cytoreductive treatment groups, respectively (p
The phase I/II RUXOPEG Study (NCT02742324) was a multicenter, adaptive trial in patients with MF (intermediate- or high-risk) that evaluated the combination of ruxolitinib and pegylated interferon alpha-2a.
57
During phase I of the study, patients (N = 18) received one of nine possible combinations of ruxolitinib and pegylated interferon (10, 15, and 20 mg BID; and 45, 90, and 135 µg/week, respectively).
57
No dose-limiting toxicities occurred during phase I; therefore interferon 135 µg/week + ruxolitinib 15 or 20 mg BID were chosen for further evaluation in patients (N = 19) during phase II.
57
Overall, a
Ropeginterferon alfa-2b-njft
Ropeginterferon alfa-2b-njft was approved by the US Food and Drug Administration (FDA) in 2021 to treat PV, and is currently the only interferon approved to treat MPNs.21,58,59
The phase II/III PEGINVERA Study (NCT01193699), an open-label, prospective, multicenter, dose-escalation trial, was undertaken to determine the maximum tolerated dose and assess the efficacy and safety of ropeginterferon alfa-2b-njft in patients with PV.23,48 The study enrolled 51 patients with PV who received either a low dose (<300 µg) or high dose (⩾300 µg) of ropeginterferon alfa-2b-njft administered subcutaneously every 2 weeks.23,48 Median exposure to ropeginterferon alfa-2b-njft was 5.1 years; patients required a median of 34 weeks of treatment to achieve CR [defined as hematocrit <45% (without phlebotomy in the previous 2 months), platelet count ⩽400 × 109/L, WBC count ⩽10 × 109/L, normal spleen size (measured via ultrasound), and absence of thromboembolic events] and a median of 10 weeks to achieve a PR [defined as either hematocrit <45% without phlebotomy but with persistent splenomegaly or elevated (>400 × 109/L) platelet counts, or reduction in requirement of phlebotomy by at least 50%].23,48 The best observed hematological response in the efficacy set was CR in 27/42 (64.3%) of patients and PR in 14/42 (33.3%). 48 The best observed individual molecular response was complete molecular response (CMR; defined as reduction of JAK2 allelic burden to undetectable levels) in 12/42 (28.6%) of patients and partial molecular response (PMR; defined as reduction ⩾50% in patients with <50% mutant allele burden at entry, or a reduction ⩾25% in patients with >50% mutant allele burden) in 19/42 (45.2%) of patients.23,48 A median of 82 weeks of treatment was required to achieve a CMR, and a median of 34 weeks was needed to achieve a PMR. 48 At least one AE was reported in 48/51 (94.1%) of patients; the majority (97.3%) of AEs were mild or moderate in severity. 48 The most frequently reported AEs (>20%) were arthralgia, influenza-like illness, and fatigue. 48
The PROUD-PV Study (EudraCT 2012-005259-18) and its long-term extension study CONTINUATION-PV (EudraCT 2014-001357-17) were phase III, randomized, controlled, open-label trials in patients with PV,49,60,61 that evaluated the safety and efficacy of ropeginterferon alfa-2b-njft versus HU or best available therapy (BAT) over 6 years.49,61 Patients in the ropeginterferon alfa-2b-njft group received a starting dose of 50–100 µg every 2 weeks subcutaneously, and patients in the HU group received 500 mg/day orally. After 1 year in the PROUD-PV Study (N = 254), 21% of patients receiving ropeginterferon alfa-2b and 28% of patients receiving HU (response difference: 95% CI: −17.23 to 4.09; p = 0.23) achieved complete hematological response (CHR; defined as hematocrit
The phase II, multicenter P1101MF Study (NCT04988815) evaluating ropeginterferon alfa-2b in patients with early/pre-fibrotic primary myelofibrosis (pre-PMF) and a Dynamic International Prognostic Scoring System (DIPSS) score of low/intermediate-1 risk of MF is ongoing.64,65 Participants receive ropeginterferon alfa-2b at a starting dose of 250 µg, followed by 350 µg at week 2, 500 µg at week 4, and 500 µg every 2 weeks thereafter.
64
As of the 27 February 2023 data cut-off, 62 patients had enrolled; 71% (44/62) had pre-PMF, 9.7% (6/62) had overt PMF, 8.1% (5/62) had post-PV MF, and 11.3% (7/62) had post-ET MF.
65
Clinicohematologic CR in patients at 12 weeks (n = 46) and 24 weeks (n = 30) was 74% and 67%, respectively.
64
Responses in hemoglobin (defined as 10 g/dL to upper limit of normal), WBC (defined as WBC
The Low-PV Study (NCT03003325) was a phase II, multicenter, open-label, randomized trial that assessed the efficacy of phlebotomy + aspirin (standard treatment) with or without ropeginterferon alfa-2b-njft in patients with PV at low risk of thrombosis.50,51 Patients received 100 µg of ropeginterferon alfa-2b-njft subcutaneously in addition to standard therapy every 2 weeks.50,51 After 1 year of treatment, 52/64 (81%) of patients in the ropeginterferon alfa-2b-njft group had achieved response (hematocrit
Clinical considerations of interferon therapy
Safety and tolerability of interferons
Safety data from completed trials are summarized in Table 1. Although no head-to-head comparisons exist, rates of discontinuation with interferons due to AEs are highly variable and, among other factors, can be influenced by the specific formulation and dosing regimen being used.9,66 A systematic review and meta-analysis of the use of interferons in the treatment of PV and ET included 23 studies of patients with PV (N = 629) and 30 studies including patients with ET (N = 730). 67 Due to the limitations of AE data among these studies, a formal meta-analysis of AEs could not be performed. 67 However, the authors noted that qualitatively, flu-like symptoms were highly prevalent, especially with the use of non-pegylated interferons. 67 The combined discontinuation rates of interferon therapy in patients with PV or ET were 6.5% and 8.8%, respectively. 67 Results from a meta-regression analysis that compared discontinuation rates between pegylated and non-pegylated interferons were not statistically significant (p = 0.23). 67 In phase II and III studies of pegylated interferon alfa-2a (interferon dose: 45–180 µg weekly), rates of discontinuation due to AEs were 13.9% and 15%, respectively in the interferon arms.43,44 A phase II study of pegylated interferon alfa-2b (interferon dose: 0.5–1.0 µg/kg weekly) reported discontinuation rates due to AEs of 38% in the treatment arm. 46 Another exploratory study of pegylated interferon alfa-2b (interferon dose: 180 µg weekly) found the discontinuation rate due to AEs was 9.1%. 68 In a phase I/II study to determine the maximum tolerated dose of ropeginterferon alfa-2b-njft (interferon dose: 50–540 µg every 2 weeks), the discontinuation rate due to AEs was 20%. 23 A phase III study investigating ropeginterferon alfa-2b-njft (interferon dose: 50–500 µg every 2 weeks) observed discontinuation rates due to AEs of 11%. 69 In the PROUD-PV and CONTINUATION-PV Studies, 32% and 2% of patients receiving ropeginterferon alfa-2b-njft reported grade 3 or grade 4 toxicities, respectively, after 3 years. 61 In the MPD-RC-112 Study, 46% of patients receiving peginterferon alfa-2a reported grade 3 or 4 toxicities. 44
Thrombosis risk
One of the most common complications of both PV and ET is thrombosis, and prior history of thrombosis is a key risk stratification factor in both PV and ET.42,70,71 Due to the chronic nature of MPNs and the constraints of clinical trial follow-up, data is limited with regard to thrombotic events in patients receiving interferon therapy.23,43,44,72 In a recent study, time on interferon was shown to be associated with lower all-cause mortality independent of history of thrombosis. 56 Over the 6 years of treatment in the CONTINUATION-PV Study, the probability of event-free survival (risk events: disease progression, thromboembolic events, and death) was found to be significantly higher among patients receiving ropeginterferon alfa-2b-njft compared with the control group (p = 0.04).49,69
Significance of changes in VAF measurements
A 2010 study estimated that in the first 12 years of disease, VAF increases by 1.4% and 1.5% per year in male and female patients with MPNs, respectively.
73
These data were corroborated in the 5-year analysis of the PROUD-PV and CONTINUATION-PV Studies in patients with PV, which also showed in an increase in the VAF of 1.3% per year in the control arm.73,74 Although the full significance of decreasing VAF in patients with MPNs is still under investigation, studies have shown positive correlations among lower JAK2 V617F VAF and clinical outcomes.75–77 In patients with MPNs, a JAK2 V617F VAF of ⩾50% was associated with a higher risk of venous thrombosis, but not arterial thrombosis.75,77 Allele burden may also influence disease progression. In a 2014 study, the incidence rate of MF was significantly higher in patients with high or unsteady JAK2 V617F VAF compared with those patients having low VAF (2.8 versus 0.1 cases of MF/100 person-years; p
Practical management of interferon-based therapies
How to initiate treatment with interferons
Whether initiating interferons or switching from HU, clinical and laboratory monitoring are essential to ensuring safe and effective therapy. One should consider switching therapies if a patient experiences unacceptable levels of toxicity associated with HU, a lack or loss of hematologic response, the occurrence of a vascular event or progressive disease state, due to patient preference, physician preference, or pregnancy. Laboratory and clinical monitoring are essential to ensure a safe and effective transition of therapy. Blood counts, chemistry profile with liver function tests, and thyroid function should be monitored at least every 2–4 weeks during the initial 3 months of interferon therapy. Importantly, the approach to the transition of therapy in a patient with MPN should be individualized to account for baseline blood counts and comorbid conditions. Patients should consider undergoing eye examinations before and during interferon therapy and those who develop new or worsening eye disorders that cannot be attributed to alternative causes should discontinue treatment. Interferon should also be discontinued in patients experiencing moderate-to-severe hepatotoxicity and endocrine toxicities that cannot easily be managed medically, or in those with other autoimmune or organ toxicities. Peginterferon alfa-2a has been given to pregnant and lactating women but few data for use of ropeginterferon alfa-2b-njft in these same groups are currently available; the prescribing information for ropeginterferon alfa-2b-njft does not indicate its use in pregnant or lactating women and cites potential risks and insufficient data in these populations. 21
When switching a patient from HU to interferon therapy, HU is continued at the current dose with the interferon being initiated concurrently at a low level (Figure 1).

Considerations when switching to interferons. (a) Dosing regimen for ropeginterferon alfa-2b-njft (every 2 weeks) and peginterferon alfa-2a (every week). Peginterferon alfa-2a should be administered 45–90 μg subcutaneously weekly and titrated monthly in 45 μg increments to a maximum of 180 μg weekly. (Note that if there are concerns about sensitivity, even lower dosing can be considered.) The recommended starting dose of ropeginterferon alfa-2b-njft is 100 μg subcutaneously every 2 weeks (50 μg if receiving HU) with up-titration by 50 μg every 2 weeks to a maximum of 500 μg. After 1 year of treatment with ropeginterferon alfa-2b-njft and with hematological stability, dosing can be reduced to every 4 weeks. After 5 years, or even earlier, dosing of peginterferon alfa-2a can be adjusted to every 2 weeks. (b) Representative schematic of the titration regimens when switching a patient from HU to interferon, showing the concurrent titration up of interferon while titrating HU down. For those on HU prior to initiating ropeginterferon alfa-2b-njft, taper the HU off by reducing the total biweekly HU dose by 20–40% every 2 weeks during weeks 3–12 with complete discontinuation of HU by week 13. Interferon dose should be titrated up to the dose at which adequate hematologic results are obtained (maximum doses, peginterferon alfa-2a: 180 µg subcutaneously every week; ropeginterferon alfa-2b-njft: 500 µg subcutaneously every other week).
Peginterferon alfa-2a should be administered subcutaneously at 45 or 90 μg weekly and titrated monthly in 45 μg increments to a maximum of 180 μg weekly. The recommended starting dose of ropeginterferon alfa-2b-njft is 100 μg by subcutaneous injection every 2 weeks (50 μg if receiving HU). The dose should be increased by 50 μg every 2 weeks (up to a maximum of 500 μg) until hematological parameters are stabilized. Once the optimal dose is identified, visits can occur less frequently (every 3–4 months). If switching a patient from interferon to next-line therapy, there is no need to taper the interferon dose. No data exist to support a switch from one interferon therapy to another in the event of lack of efficacy or development of a concerning toxicity. Interim data from a multicenter study in Korea and a phase II study in China suggest that an accelerated design regimen could be used, and the ECLIPSE-PV and EXCEED-ET Studies are also investigating an optimized dosing regimen (ClinicalTrials.gov Identifier: NCT05481151 and NCT05482971).52,83 Blood counts are monitored every 2 weeks, and HU is tapered down on an individualized basis while the interferon dose is increased. For those on HU prior to initiating ropeginterferon alfa-2b-njft, taper the HU off by reducing the total biweekly HU dose by 20–40% every 2 weeks during weeks 3–12 with complete discontinuation of HU by week 13. 21 In patients who demonstrate normalized blood counts after 1 year, interferon dose can be tapered down to ensure ongoing tolerance. Common AEs associated with interferon therapy and general recommendations for treatment are summarized in Table 3.

Specific dose modifications for peginterferon alfa-2a and other interferon products are not available. However, similar principles should be applied.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyltransferase; NYHA, New York Heart Association; ULN, upper limit of normal; WBC, white blood cell.
Advantages of early treatment
Early treatment of MPNs can result in better outcomes for patients in terms of lowering the risk of thrombotic events and delaying disease progression.56,84 Research has shown that JAK2 V617F+ cells can be present decades before the development of MPNs as a result of a single mutated HSC growing exponentially and competitively over years.3,53,85 In addition to addressing cell counts of patients with MPNs, interferons can have positive effects on the driver mutation-bearing stem and progenitor cell pool, thus effectively reducing VAF.44,47,49,50 Higher JAK2 V617F VAF correlates with negative clinical outcomes and a higher incidence rate of MF. 76 It is important to note that although the early reduction of JAK2 V617F may result in better clinical outcomes, it is not currently part of treatment guidelines.53,84
Contraindications for the use of interferons
Peginterferon alfa-2a and -2b are not approved by either the FDA or European Medicines Agency (EMA) for use in MPNs. Ropeginterferon alfa-2b-njft is approved by the FDA and EMA for use in patients with PV. Peginterferon alfa-2a and -2b, and ropeginterferon alfa-2b-njft are contraindicated in patients with autoimmune diseases, hepatic impairment, and hypersensitivity to interferon or to any component to therapy.21,58,59 Ropeginterferon alfa-2b-njft is also contraindicated in patients with existing or a history of severe psychiatric disorders, and in immunosuppressed transplant recipients. 21 It should also be noted that the use of interferons should be delayed for at least 6 weeks in patients who have had a stroke, and that psychiatric disorders should be considered when managing patients receiving peginterferon alfa-2a and -2b.
Discussion
In a recent survey, 35% of patients with ET agreed that prevention of vascular/thrombotic events was the most important goal of treatment, compared with 57% of physicians. 86 For patients with MF or PV, the slowing or delaying of progression was noted as being the most important goal of treatment, whereas physicians reported improvement of symptoms and prevention of vascular/thrombotic events as being most important for those patients. 86 The use of interferons in patients with MPNs is of particular interest as these therapies may allow for a combination of thrombosis reduction and disease course modification, supported by the driver mutation VAF reduction observed in prospective studies.43,44,47–50
Clinical use of interferons
Considering the efficacy and safety profiles of pegylated interferons, why are they not used more often? In a chart review analysis of approximately 1400 patients with PV (median age 72.2 years), the use of cytoreductive therapy in high-risk patients was highly varied across 42 centers (10.1–100%). 87 One reason cited for not initiating pegylated interferons as cytoreductive therapy was patients’ objections because of potential AEs. 87 Overall, for patients undergoing cytoreductive therapy, 72.3% of those received HU, 22.4% received ruxolitinib, and 2.0% received pegylated interferons. 87 MPNs are becoming increasingly more recognized in adolescents and young adults, and where cytoreductive therapy is required, pegylated interferons are often the preferred first-line therapy, given their lack of genotoxicity and carcinogenenicity. 88
Limitations of interferon use
Due to the chronic and progressive nature of MPNs, treatment is often needed for long periods of time to control disease symptoms and progression.56,89,90 Interferons may be associated with significant side effects in some patients, and prolonged use can result in discontinuation due to AEs.9,23,43,44,46,56,66,68,74 A 7-year (median) follow-up of a phase II study in patients with PV and ET who received peginterferon alfa-2a (90–450 µg/week subcutaneously) showed that, although rates of AEs decreased over time, they did not disappear entirely. 45 The most common late AEs were fatigue (all years), anemia (highest in the third and sixth year), neutropenia (highest in third and sixth year), and depression (highest in fourth through sixth years). 45 Two or more years from the start of interferon therapy, new grade 3 and 4 toxicities unrelated to dose occurred in 10–17% of patients per year. 45 Improvement in symptom burden with interferon treatment can vary based on hematological response and symptom burden at baseline, among other factors. 91 In the MPN-RC 111 and MPN-RC 112 Studies, 20.8% of patients with high baseline symptom burden and 16.7% of patients with low baseline symptom burden experienced improvement in total symptom score from baseline to 1 year. 91 It should also be noted that the clinical effectiveness of interferon therapies can vary among patients and disease characteristics. Until ropeginterferon alfa-2b-njft was approved for use in PV, no interferon was approved for use in MPNs. This made accessing interferon therapies challenging.21,90
Biomarkers of response and resistance
Increasing use of myeloid gene panels allows the possibility of using mutational information in guiding treatment selections and expectations. For interferons, there is data that suggests that co-existing mutations could serve as a predictive biomarker and provide insights into resistance mechanisms. In one study, patients failing to achieve CMR had a higher frequency (56% versus 30%) of mutations outside the JAK/STAT pathway and are more likely to acquire new mutations during therapy. 92 Further, those with both JAK2 V617F and TET2 mutations at therapy onset had a higher JAK2 V617F allele burden and a less significant reduction in JAK2 V617F allele burden. 92 The resistance of TET2 mutation eradication was previously noted in another study as well. 93 Analysis from the DALIAH study showed that treatment-emergent mutations in DNMT3A were observed more commonly in patients treated with IFNα compared with HU (p = 0.04) and that these were significantly enriched in IFNα-treated patients not attaining CHR (p = 0.02). 53 Further, in patients treated with IFNα, those with CHR had a greater reduction in the JAK2 VAF as compared to those not achieving CHR. 53 In contrast, the CALR VAF did not significantly decline in those achieving CHR as compared to those not achieving CHR. 53 Germline polymorphism data from the PROUD-PV/CONTINUATION-PV studies showed that interferon lambda 4 (IFNL4) diplotype status may serve as a biomarker for molecular response. 94 Overall, though, these findings are limited to few studies. The impact of co-existing mutations, mutational burden, clonal complexity, and treatment-emergent mutations will need further elucidation and confirmation.
Combination therapy
Due to the wide range of etiologies, pathologies, and disease progression profiles among MPNs, there are currently many interferon-containing combination therapies under investigation to address the diseases more comprehensively by combining the complementary therapeutic effects of different treatments.57,95,96 As discussed, the phase I/II RUXOPEG Study showed positive hematologic and molecular effects in patients with MF. 57 The COMBI-I Study investigated the combination of interferon-alpha-2a and ruxolitinib in patients with PV and showed positive effects on hematological response, need for phlebotomy, and JAK2 V617F VAF. 96 This therapeutic approach is worthy of prospective randomized trials with single-agent ruxolitinib as the control arm.
Discontinuation of therapy
The use of pegylated interferons, either alone or in combination with other therapies, could potentially lead to long-term hematological remission and eventual minimal residual disease (MRD) status.90,97 MRD status refers to the reduction of VAF in peripheral blood to low or undetectable levels.90,97 The ability of interferons to affect MPN hematopoietic progenitors and preferentially deplete JAK2 V617F mutated stem cells may allow patients to achieve MRD status and discontinue therapy for periods of time as a therapeutic holiday.16,17,36,90,96,97
Conclusion
Pegylation of interferons can increase stability, prolong activity, and reduce immunogenicity of the molecule, resulting in a formulation that is more tolerable for patients. Although their exact MOA is not fully understood, interferons have been shown to target and deplete JAK2 V617F stem and progenitor cells. The potential disease-modifying aspect of interferons sets them apart from other therapies for MPN. In recent years, numerous clinical trials have been undertaken to investigate the use of pegylated interferons in patients with MPNs, and there are more underway to evaluate accelerated dosing regimens and combination therapies. More research is still needed to determine the ideal timing of interferon treatment and whether discontinuation of therapy is possible if MRD status is achieved. Pegylated interferons represent an important therapeutic option, and future work will further refine therapeutic approaches with a goal of achieving true disease modification for patients with MPNs.
Footnotes
Acknowledgements
Medical writing and editorial assistance were provided by Matt Brown, PhD, and Linda Ritter, PhD, of Symbiotix, LLC, and were funded by PharmaEssentia USA Corporation. The authors received no honorarium/fee or other form of financial support related to the development of this article. The authors retained full editorial control and provided final approval on all content.