
Abstract
Background:
Thrombocytopenia post hematopoietic stem-cell transplantation (HCT) usually contributes to poor outcomes with no standardized treatment. Eltrombopag and romiplostim can be feasible for post-HCT thrombocytopenia, but the use of avatrombopag has not yet been evaluated.
Objectives:
We aimed to evaluate the efficacy and safety of avatrombopag treatment in patients diagnosed with post-HCT thrombocytopenia.
Design:
In this retrospective study, we evaluated the efficacy and safety of avatrombopag treatment in a cohort of 61 patients diagnosed with thrombocytopenia post HCT in our clinical center.
Methods:
Avatrombopag was initiated at 20 mg daily, with a dosage adjustment to achieve platelet recovery to >20 × 109/l independent from transfusion for 7 consecutive days (overall response, OR) or to >50 × 109/l free from transfusion for 7 consecutive days (complete response, CR). Factors influencing OR and CR were studied in univariate and multivariate analyses, respectively. Within the follow-up, adverse events like myelofibrosis, thrombosis, and organ toxicities were monitored carefully.
Results:
The overall response rate (ORR) to avatrombopag was 68.9% and the cumulative incidence (CI) of OR was 69.1%. The complete response rate (CRR) and the CI of CR were both 39.3%. The median days from avatrombopag initiation to OR and CR were 21 and 25 days, respectively. An adequate number of megakaryocytes before the initiation of avatrombopag was an independent protective factor of avatrombopag treatment for OR (hazard ratio, HR = 4.628, 95% confidence interval 1.92–11.15, p = 0.0006) and CR (HR = 4.892, 95% confidence interval 1.58–15.18, p = 0.006). Avatrombopag was well tolerated in all patients with no severe adverse events.
Conclusion:
Our findings suggested that avatrombopag can be optional for thrombocytopenia post HCT.
Keywords
Introduction
Hematopoietic stem-cell transplantation (HCT) is a critical therapy for several hematological malignancies and non-malignant disorders. Nevertheless, HCT has several severe complications affecting its benefit, among which thrombocytopenia brings a high risk of transplantation-related mortality (TRM).1–3 The reported incidence of thrombocytopenia post HCT varies from 20% to 40%. 3 Causes of thrombocytopenia post HCT are diverse, including impaired graft function, graft-versus-host disease (GVHD), viral infection, underlying disease relapse, and drug toxicity. 4 Repeated platelet transfusion, glucocorticoids, intravenous immunoglobulin, rituximab, and recombinant human thrombopoietin (rhTPO) were documented to restore platelet counts in patients who suffer from thrombocytopenia post HCT, but still, standardization and reliability of these therapies are lacking for these patients.
Avatrombopag is a new kind of small molecule thrombopoietin receptor agonist (TPO-RA) approved for the indications of either periprocedural thrombocytopenia associated with chronic liver disease (CLD) or adult chronic immune thrombocytopenia (ITP). Avatrombopag has similar drug properties to eltrombopag, such as the same binding site of c-mannosylation of thrombopoietin receptor (c-MPL) and the potency of inducing the differentiation and maturation of megakaryocytes (MKs), finally leading to the increase of platelet production. However, two main differences between avatrombopag and eltrombopag exist. Approximately 88% of the avatrombopag is eliminated through gut, 5 indicating that it is almost free from the signal for hepatotoxicity unlike eltrombopag. The other difference is that avatrombopag does not require dietary restrictions owing to its zero- and first-order absorption property. 6 In contrast, eltrombopag is poorly absorbed in the presence of dietary fat and multivalent cations such as calcium. 7
Two prior TPO-RAs, romiplostim and eltrombopag, have been validated to be feasible for thrombocytopenia post HCT, but information regarding the use of avatrombopag is presently absent. Therefore, we reported the efficacy and safety of avatrombopag based on the data derived from 61 patients who suffered from thrombocytopenia post HCT in our clinical center. To our knowledge, it is the first retrospective study of avatrombopag as a therapy for the post-HCT thrombocytopenia.
Method
Patients
This retrospective cohort included 61 consecutive patients who developed thrombocytopenia after HCT and were treated with avatrombopag in the First Affiliated Hospital of Soochow University between September 2020 and October 2021. All patients enrolled satisfied the criteria including the achievement of complete donor cell chimerism, absence of hepatic dysfunction (serum transaminases and serum bilirubin greater than 2.5 times and twice normal levels, respectively), and absence of evidence of concurrent disease relapse. The study was approved by the ethics committee of our hospital (approval number: Sdfyy-2021-301) and informed consent forms from all patients were obtained. We de-identified all patient details in our manuscript. The inclusion procedure was shown in Figure 1.
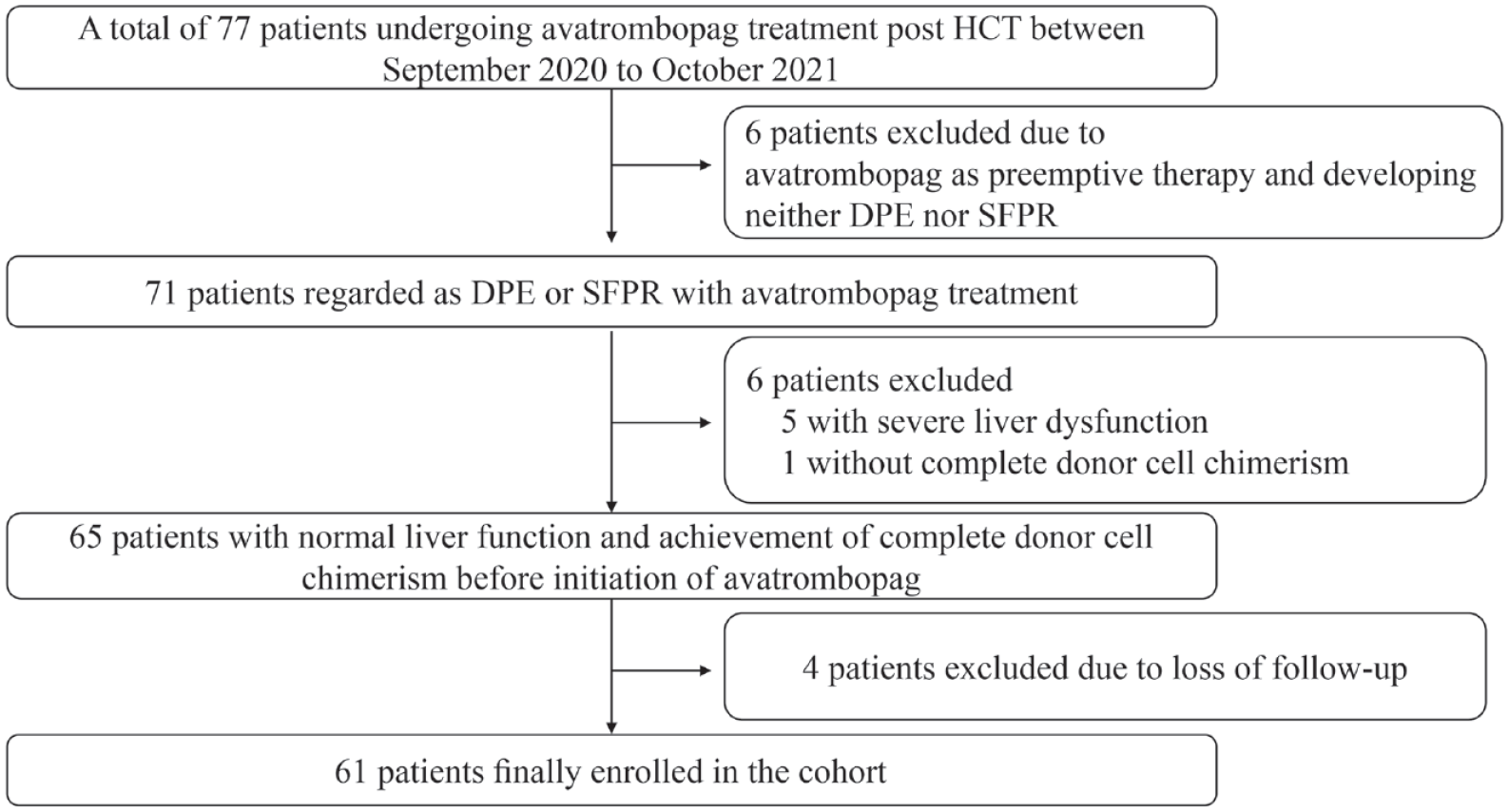
Flow chart of patient inclusion.
Conditioning regimen and prophylaxis of GVHD
The following conditioning regimens were implemented: (1) Modified BuCy: It consisted of semustine 250 mg/m2/day orally on day –10, cytarabine 2 g/m2/day intravenously on days −9 to −8, busulfan (Bu) 0.8 mg/kg intravenously every 6 h on days −7 to −5, and cyclophosphamide (Cy) 1.8 g/m2/day intravenously on days −4 to −3. (2) TBI + Cy: It was composed of semustine 250 mg/m2/day orally on day −8, total body irradiation (TBI) 400–450 cGY/day on days −7 to −6, cytarabine 2 g/m2/day intravenously on days −6 to −5, and Cy 1.8 g/m2/day intravenously on days −4 to −3. (3) Flu + Cy: This regimen contained Fludarabine (Flu) 30 mg/m2 on days −7 to −3 and Cy 50 mg/kg/day on days −4 to −3. Modified BuCy and TBI + Cy were considered myeloablative conditioning (MAC), while Flu + Cy was regarded as reduced-intensity conditioning (RIC).
GVHD prophylaxis included cyclosporine A (CsA) 3 mg/kg/day and short-course methotrexate (MTX) on day +1 (15 mg/m2), +3, +6, +11 (10 mg/m2) for human leukocyte antigen (HLA)–matched sibling transplantation. In unrelated and haploidentical transplantation, mycophenolate mofetil (MMF) 15 mg/kg orally every 12 h on days −9 to +28, and anti-thymocyte globulin (ATG, thymoglobuline) 2.5 mg/kg/day intravenously on days −5 to −2 were administrated besides CsA and a short-course MTX.
Criteria of thrombocytopenia post HCT
Thrombocytopenia post HCT was stratified into two categories in our study, delayed platelet engraftment (DPE) and secondary failure of platelet recovery (SFPR). DPE was defined as a platelet count less than 20 × 109/l or dependence of platelet transfusion for over 35 days after HCT. 8 SFPR was defined as a platelet count less than 20 × 109/l which lasted for more than 7 consecutive days or with a demand for platelet transfusions after primary platelet engraftment. 9
Myelodysplastic syndrome (MDS), aplastic anemia (AA), primary myelofibrosis (PMF), and Fanconi anemia (FA) were considered bone marrow failure syndrome (BMFS) owing to the incapability to produce adequate numbers of hematopoietic elements.10–12
Bone marrow (BM) aspiration was performed right before the initiation of avatrombopag administration. The number of MKs was measured using a 1.5 × 3.5 cm2 area of BM aspirate smear, with a normal range from 7 to 35.
Avatrombopag administration
The initial dose was 20 mg daily, which was subsequently increased by 20 mg every 2 weeks in accordance with the response and tolerance of patients, with a maximum dosage of up to 60 mg/day. Avatrombopag was tapered or stopped when the platelet count was greater than 100 × 109/l or 200 × 109/l, respectively, without any platelet transfusion. If a decline of platelets reoccurred during the tapering period, the dosage was adjusted accordingly.
Endpoints
The primary endpoint was overall response (OR), which was defined as an increase of platelet count to >20 × 109/l after the initiation of avatrombopag, independence of platelet transfusion for at least 7 consecutive days. Complete response (CR), defined as a platelet recovery to >50 × 109/l after avatrombopag treatment absent from platelet transfusion for 7 consecutive days, was one of the secondary endpoints. Other secondary endpoints included the days from avatrombopag initiation to OR and CR, adverse events related to the application of avatrombopag, and the independent factors affecting the response to avatrombopag therapy. National Cancer Institute Common Toxicity Criteria (NCI-CTC) version 5.0 was introduced to grade adverse events in our study. The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 13
Statistical analysis
Continuous data were shown as median plus inter-quartile ranges (IQRs), while categorical data were indicated as percentages. Categorical data were compared using χ2 test between groups, while the comparisons of continuous data were conducted with the Mann–Whitney U test. The factors with a p value < 0.1 and with considerable clinical significance were input into multivariate analysis. The cumulative incidence (CI) of OR and CR were calculated respectively, and Gray’s test was implemented regarding disease relapse and death before platelet response as competing risks. Data analysis was completely conducted with R software (version 4.1.3). It was considered statistically significant for p value < 0.05. The follow-up was up to 120 days after the first administration of avatrombopag.
Results
Patient characteristics
Basic clinical characteristics of included patients were summarized in Table 1. The underlying diseases of the cohort were acute myeloid leukemia (AML, n = 23), acute lymphoblastic leukemia (ALL, n = 17), MDS (n = 5), AA (n = 6), PMF (n = 4) and others, including FA (n = 1), chronic myelomonocytic leukemia (n = 2), and B cell lymphoma (n = 3). The median age of the patients was 43 years old (IQR, 29–51). Neutrophil engraftments were achieved in all patients with a median time of 12 days (IQR 11–14) after HCT. Twenty-one (34.4%) and five (8.2%) patients suffered from cytomegalovirus (CMV) and Epstein–Barr virus (EBV) infection, respectively. Fifteen (24.6%) patients experienced II to IV degree of GVHD. Nineteen (31.1%) patients had a history of rhTPO administration. The whole cohort consisted of 35 (57.6%) DPE patients and 26 (42.6%) SFPR patients.
Clinical characteristics of included patients.

AA, aplastic anemia; ALL, acute lymphoblastic leukemia; AML, acute myelocytic leukemia; BM, bone marrow; BMFS, bone marrow failure syndrome; CMV, cytomegalovirus; CR, complete response; DPE, delayed platelet engraftment; EBV, Epstein–Barr virus; FACT-G, functional assessment of cancer therapy-general; GVHD, graft-versus-host disease; HC, hemorrhagic cystitis; HCT, hematopoietic stem-cell transplantation; HLA, human leukocyte antigen; IQR, inter-quartile range; MAC, myeloablative conditioning; MDS, myelodysplastic syndrome; MNC, mononuclear cell; NR, no response; PB, peripheral blood; PMF, primary myelofibrosis; PR, partial response; rhTPO, recombinant human thrombopoietin; RIC, reduced-intensity conditioning; SFPR, secondary failure of platelet recovery.
Among patients with ALL, AML, and MDS.
Patients alive till the end of follow-up.
Efficacy of avatrombopag treatment
Avatrombopag was started at a median time of 48 days (IQR 31–66) post HCT. The maximum dosage varied from 20 to 60 mg, but only three patients received the maximum dose of 60 mg. The total efficacy of avatrombopag was shown in Table 2. In the whole cohort, 42 (68.9%) out of 61 patients responded to avatrombopag with a median time of 21 days (IQR 6–33). The CI of OR was 69.1% (Figure 2). Among the 42 responders, 25 (59.5%) were diagnosed with DPE and the rest 17 (40.5%) patients were SFPR. Twenty-four (39.3%) of the patients analyzed achieved CR with a median time of 25 days (IQR 9–40). The CI of CR was 39.3% (Figure 3). At the last follow-up, 31 (50.8%) patients withdrew avatrombopag without any platelet transfusion dependence. The platelet counts of nine (14.8%) patients maintained stable independence of transfusion with the help of avatrombopag, not meeting the criteria of tapering off or quitting. Sixteen (26.2%) patients were still in need of blood transfusion, most of whom were suffering from severe infection or III to IV degree of GVHD. Two of the 16 transfusion-dependent patients responded to avatrombopag previously, and the rest were non-responders to avatrombopag (n = 14). One (1.6%) patient died, and four (6.6%) patients relapsed during the follow-up period.
Outcomes of avatrombopag treatment.
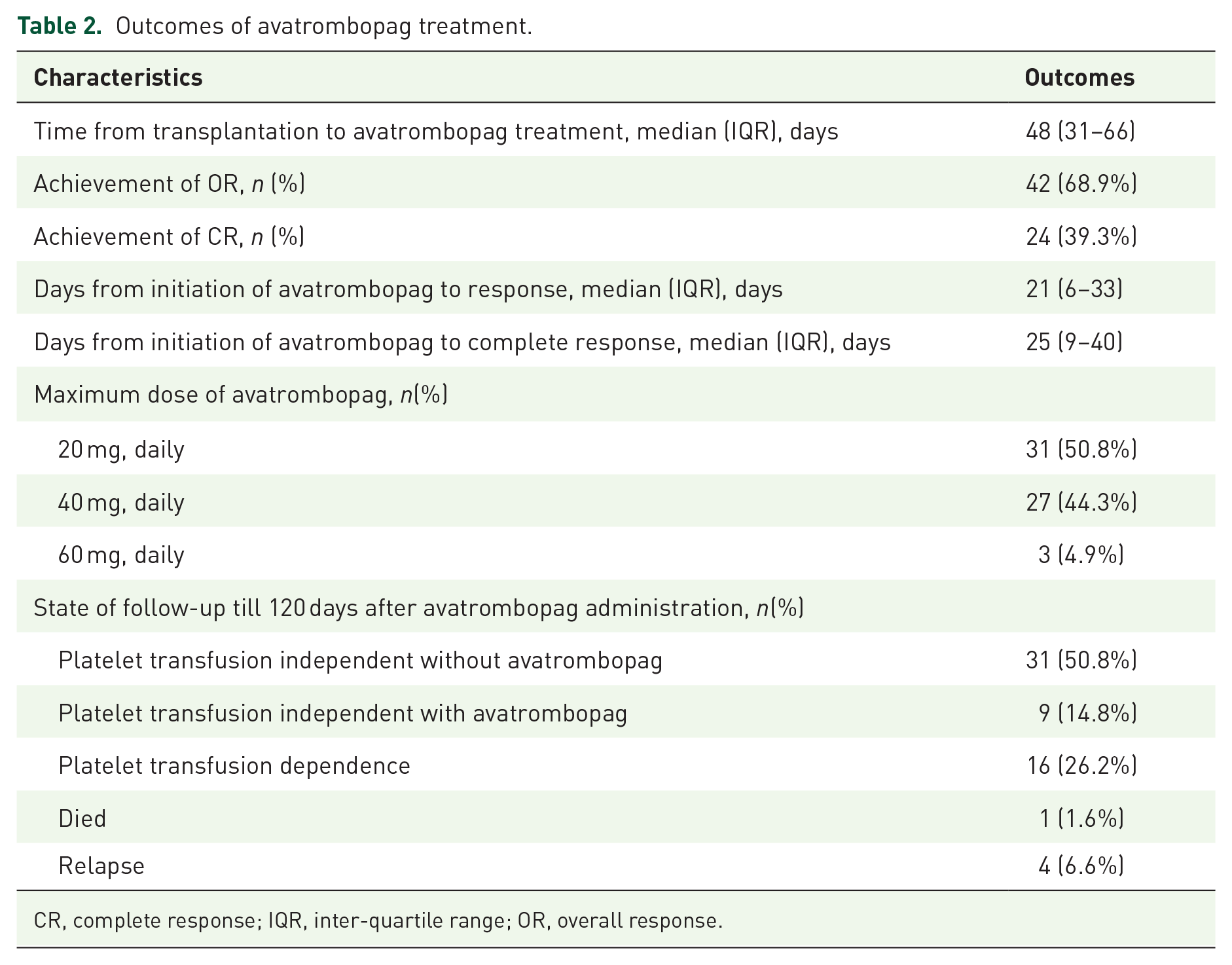
CR, complete response; IQR, inter-quartile range; OR, overall response.

The cumulative incidence of overall response (OR) (n = 61).

The cumulative incidence of complete response (CR) (n = 61).
Predictors of the efficacy of avatrombopag treatment
According to univariate analysis (Table 3), OR to avatrombopag was relevant to the adequate MKs before treatment initiation (89.7% for MK adequate patients versus 32.6% for MK inadequate patients, p < 0.0001, Figure 4(a)) and BMFS diagnosis (43.8% for BMFS patients versus 78.1% for non-BMFS patients, p = 0.02, Figure 4(b)). Clinical characteristics stratified by the endpoint, CR to avatrombopag were demonstrated in sTable 1 in the supplemental material. Univariate and multivariate analysis in regard to the factors influencing CR were shown in sTable 2 in the supplemental material. Univariate analysis revealed that a CR to avatrombopag was associated with patient age [54.8% for elderly patients (⩾43 years) versus 23.3% for young patients (<43 years), p = 0.01, Figure 4(c)], adequate MKs in the BM before avatrombopag initiation (53.9% for MK adequate patients versus 13.6% for MK inadequate patients, p = 0.004, Figure 4(d)), and BMFS (18.8% for BMFS patients versus 46.7% for non-BMFS patients, p = 0.07, Figure 4(e)). Other variables, including sex, disease types, disease status before HCT, the number of mononuclear cells or CD34 + cells, GVHD, viral infection, and type of thrombocytopenia post HCT, presented no impact on the OR and CR to avatrombopag treatment. Subsequently, multivariate analysis of OR and CR were performed and the results were listed in Table 3 and sTable 2 in the supplemental material. The only independent factor for OR and CR was the sufficiency of MKs in the BM before avatrombopag initiation (hazard ratio, HR = 4.628 for OR, 95% confidence interval, 1.92–11.15, p = 0.0006, and HR = 4.892 for CR, 95% confidence interval, 1.58–15.18, p = 0.006).
Factors influencing overall response in univariate and multivariate analysis.

BM, bone marrow; BMFS, bone marrow failure syndrome; CMV, cytomegalovirus; DPE, delayed platelet engraftment; EBV, Epstein–Barr virus; GVHD, graft-versus-host disease; HC, hemorrhagic cystitis; HCT, hematopoietic stem-cell transplantation; HLA, human leukocyte antigen; HR, hazard ratio; SFPR, secondary failure of platelet recovery; MAC, myeloablative conditioning; MK, megakaryocyte; MNC, mononuclear cell; PB, peripheral blood; RIC, reduced-intensity conditioning; rhTPO, recombinant human thrombopoietin.
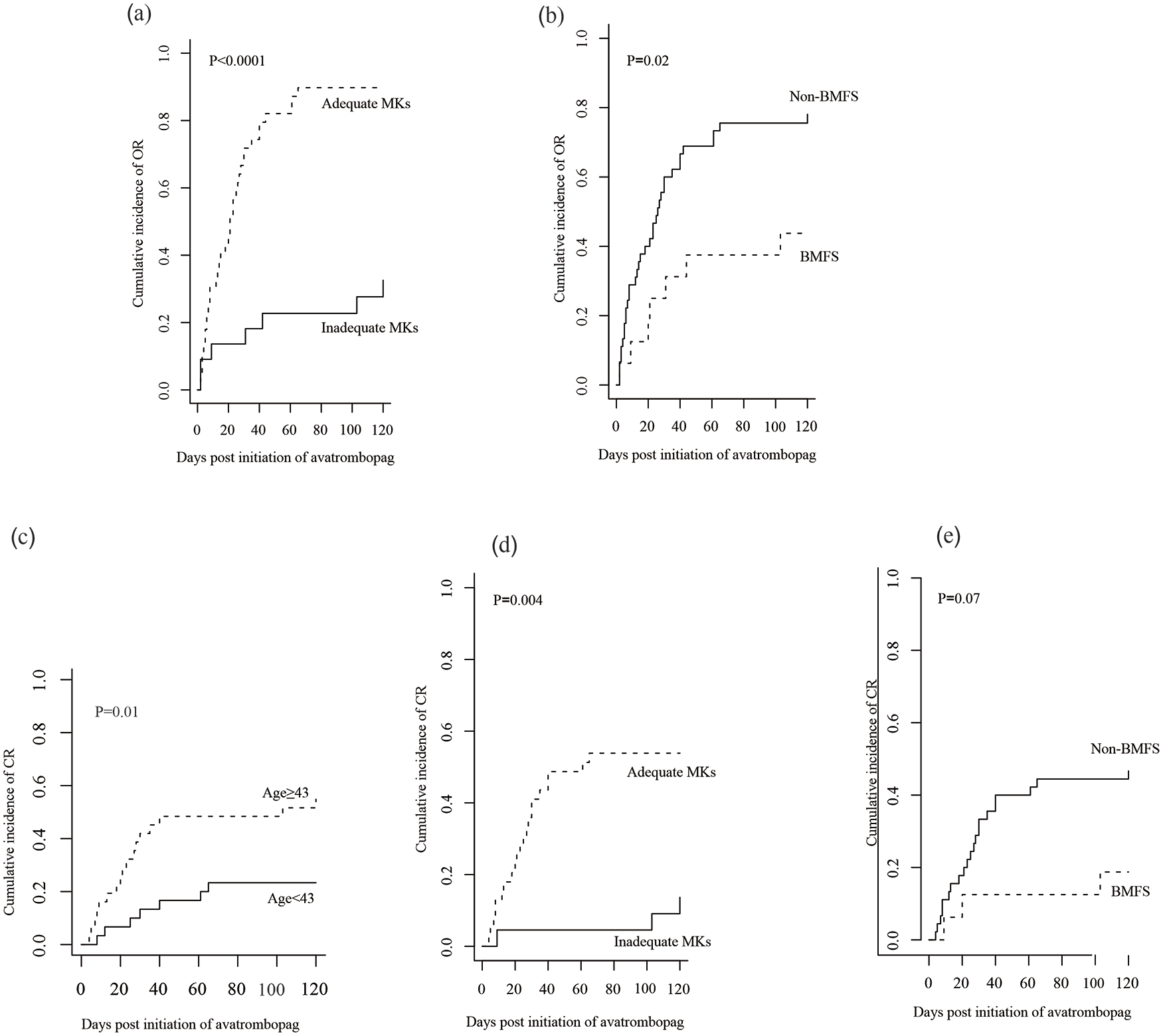
(a) The cumulative incidence of overall response (OR) between patients with adequate megakaryocytes (MKs) (n = 39) and inadequate MKs (n = 22) before starting avatrombopag. (b) The cumulative incidence of OR between bone marrow failure syndrome (BMFS) patients (n = 16) and non-BMFS patients (n = 45) before starting avatrombopag. (c) The cumulative incidence of complete response (CR) stratified according to median age (age < 43, n = 30; age ⩾ 43, n = 31). (d) The cumulative incidence of CR between patients with adequate MKs (n = 39) and inadequate MKs (n = 22) before initiation of avatrombopag. (e) The cumulative incidence of CR between BMFS patients (n = 16) and non-BMFS patients (n = 45) before initiation of avatrombopag.
Adverse events of avatrombopag treatment
Six (9.8%) patients developed hepatic dysfunction during the avatrombopag treatment. Four (66.7%) of them developed hepatic GVHD and the remaining two (33.3%) patients suffered from severe infection. Nevertheless, none of the six patients discontinued the treatment of avatrombopag. Two patients who received avatrombopag 40 and 60 mg/day, respectively, reported nausea, but treatment continued, and the symptoms disappeared with dosage adjustment. Dry tap of three patients at the initial diagnosis improved and the remaining patients presented no additional dry tap of BM aspiration. None of the patients developed fatigue, overt thrombosis, or grade III to IV degree of organ toxicities based on NCI-CTC.
Discussion
In this retrospective study, the OR rate (ORR) of avatrombopag treatment for thrombocytopenia post HCT was 68.9% and the CI of OR was 69.1%. In addition, the CR rate (CRR) and the CI of CR were both 39.3%. Avatrombopag was well tolerated among the included patients. None of them developed thrombosis, BM fibrosis, or organ toxicities. To the best of our knowledge, it was the very first time to explore the efficacy and safety of the avatrombopag treatment post HCT.
Another oral TPO-RA, eltrombopag, has been widely used in AA and adult ITP, but limited numbers of studies focused on the eltrombopag treatment within the setting of thrombocytopenia post HCT. These studies were detailed in sTable 3 in the supplemental material, but those concerning cytopenia in two or three lineages were not included. Most of the studies were retrospective and in small sample sizes. The reported ORRs (the proportion of patients whose platelet counts > 20× 109/l, free from transfusion) were similar to that of our study. However, the CRRs (the proportion of patients whose platelet count increased greater than 50 × 109/l without transfusion) varied from 33.0% to 72%,14–21 most of which were fairly higher than that of our study (39.3%), especially those earlier studies with small sample sizes. However, the outcomes of Ahmed’s study which was the latest randomized controlled trial (RCT) using eltrombopag in thrombocytopenia after HCT were not so encouraging. It revealed that CRR (platelet count > 50 × 109/l) of the eltrombopag arm was notably higher than that of the placebo arm (21% versus 0%, p = 0.046), but the difference in ORR between the two arms did not reach statistical significance after the 8-week course of treatment. 22 After an in-depth review of these studies, we found that underlying diseases in most of the patients were hematological malignancies, including AML, ALL, and MDS, whereas there was a higher ratio for non-malignancies like AA and PMF in our study. Broadly speaking, AA, PMF, FA, and MDS can be regarded as BMFS, which is characterized by the presence of ineffective hematopoiesis due to germline errors or acquired reasons, and had a certain risk of developing myeloid malignancies.23,24 In our study, the consequence of univariate analysis revealed that the BMFS was associated with poor response to avatrombopag, although the association from the multivariate analysis was not significant possibly due to the small sample size. Kong’s study suggested that the underlying disease related to impaired BM micro-environment like MDS was an independent factor for poor graft function post HCT. 25 Paradoxically, our previous work indicated that the prognosis of MDS and AA after HCT could be improved with the application of rhTPO. 26 The possible reason for the contradiction might lie in the differences in patients included. Our study only included the BMFS patients who suffered from thrombocytopenia post HCT, while Wang’s study included MDS and AA patients who underwent HCT regardless of platelet engraftment.
We also concluded that the only independent factor for OR and CR was the number of MKs in the BM before the avatrombopag initiation, which was consistent with earlier studies on eltrombopag.14,16–20 In vitro studies revealed that eltrombopag acted in multiple ways including immune regulation, 27 ferric chelation, 28 and rescue for the function of hematopoietic stem cells impaired by interferon-gamma in the inflammatory micro-environment. 29 Nonetheless, the basic pharmacological mechanism of TPO-RAs was mainly through a combination of TPO receptor c-MPL, leading to the activation of JAK-STAT, PI3K, and ERK pathways that regulated megakaryocytopoiesis. 30 In other words, an adequate number of MKs prior to initiation of TPO-RAs was the fundamental requirement for possible response to treatment. This outcome indicated that patients with sufficient MKs in the BM were more likely to benefit from avatrombopag, and for those with decreased MKs in the BM, or refractory to other therapies, low-dose DAC would be recommended.31,32
Contrary to Fu’s study, 14 our result indicated that elderly patients were more likely to achieve CR with the therapy of avatrombopag despite its lack of statistical significance from the multivariate analysis. The possible explanation might be that the elderly patients were more likely to receive RIC (25.8% of age ⩾ 43 versus 6.7% of age < 43 for receiving RIC respectively, p = 0.094). Otherwise, it was merely a bias because the patients in the competition group (relapsed or died in the follow-up) were all < 43 years old.
No severe adverse event was reported in our study, especially elevated liver enzymes, which was considered to be the main difference from other TPO-RAs administrated post HCT based on a recent meta-analysis. 33 Besides impairment of liver function, clonal evolution and progression to hematologic malignancies like MDS/AML remain major concerns of TPO-RA treatment,34,35 although a few studies demonstrated that eltrombopag did not stimulate leukemia or MDS cell growth.36,37 On the contrary, eltrombopag even presented anti-proliferation ability to some human leukemia cells. 38 Same hesitation with TPO-RAs exists under the circumstance of thrombocytopenia post HCT with underlying diseases like BMFS mentioned above. No report was found on the clonal evolution or progression of the original disease strictly attributed to the use of TPO-RAs. Similar to our study, four patients who relapsed shortly after HCT were diagnosed with AML (n = 3) and ALL (n = 1), with no direct evidence of any relationship between avatrombopag administration and relapse. However, BMFS patients including AA and MDS who underwent HCT with avatrombopag treatment should be followed up carefully for as long as possible.
There were still some limitations in our study. First, although the cohort of our study was relatively larger than that of most previous studies on eltrombopag, our study remained a retrospective one that had a low evidence level. Second, the follow-up period was shorter compared with other studies conducted with the eltrombopag treatment. Third, there was no control group in our study. To amend these deficiencies, our pilot study is in progress (NCT05143892), regarding the use of avatrombopag in the condition of thrombocytopenia post HCT, and we are looking forward to encouraging results in the near future.
Conclusion
In summary, avatrombopag provides a promising option for thrombocytopenia post HCT, but its optimal dose and administration schedule as well as the appropriate population of patients should be carefully determined based on the consequence of large RCTs.
Supplemental Material
sj-docx-1-tah-10.1177_20406207221127532 – Supplemental material for Avatrombopag for the treatment of thrombocytopenia post hematopoietic stem-cell transplantation
Supplemental material, sj-docx-1-tah-10.1177_20406207221127532 for Avatrombopag for the treatment of thrombocytopenia post hematopoietic stem-cell transplantation by Meng Zhou, Jiaqian Qi, Chengyuan Gu, Hong Wang, Ziyan Zhang, Depei Wu and Yue Han in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.