
Abstract
The treatment of immune thrombocytopenia (ITP) in adults has evolved rapidly over the past decade. The second-generation thrombopoietin receptor agonists (TPO-RAs), romiplostim, eltrombopag, and avatrombopag are approved for the treatment of chronic ITP in adults. However, their use in pregnancy is labeled as category C by the United States Food and Drug Administration (FDA) due to the lack of clinical data on human subjects. ITP is a common cause of thrombocytopenia in the first and second trimester of pregnancy, which not only affects the mother but can also lead to thrombocytopenia in the neonatal thrombocytopenia secondary to maternal immune thrombocytopenia (NMITP). Corticosteroids, intravenous immunoglobulins (IVIGs) are commonly used for treating acute ITP in pregnant patients. Drugs such as rituximab, anti-D, and azathioprine that are used to treat ITP in adults, are labeled category C and seldom used in pregnant patients. Cytotoxic chemotherapy (vincristine, cyclophosphamide), danazol, and mycophenolate are contraindicated in pregnant women. In such a scenario, TPO-RAs present an attractive option to treat ITP in pregnant patients. Current evidence on the use of TPO-RAs in pregnant women with ITP is limited. In this narrative review, we will examine the preclinical and the clinical literature regarding the use of TPO-RAs in the management of ITP in pregnancy and their effect on neonates with NMITP.
Keywords
Introduction
Thrombocytopenia, defined as a platelet count less than 150,000/µL, can occur in up to 7–11% of pregnancies due to multiple reasons (Table 1).1–5 Immune thrombocytopenia (ITP), defined as a platelet count less than 100,000/µL, is a common cause of thrombocytopenia in the first and second trimester of pregnancy and accounts for 1–4% of all causes of pregnancy-associated thrombocytopenia.2,3,6–8 Despite significant advances made in the treatment options for adult ITP, the management of pregnant patients presenting with acute ITP remains a challenge. Although all pregnant patients with ITP may not require treatment, when needed, corticosteroids and intravenous immunoglobulins (IVIGs) are the most widely used medications for treating such patients.3,6,9 Steroids take 3–7 days to achieve a response and nearly 2–3 weeks to achieve the maximum effect. 10 In pregnant women, prednisone is preferred over dexamethasone due to a lower risk of transfer via the placenta. Also, dexamethasone confers a higher risk of oligohydramnios and facial deformities in the fetus.1,11 IVIG achieves a rapid and effective response in ~80% of patients. However, the response is brief and is lost within a few weeks in most patients. 12 Splenectomy is safe during pregnancy; however, it is a more radical option and is rarely pursued.13,14 Intravenous anti-D in Rh(D)-positive women with intact spleen has demonstrated benefit in small pilot studies; however, its use is associated with the risk of maternal and fetal hemolysis. 15 Rituximab is labeled as category C by the United States (US) Food and Drug Administration (FDA) for use during pregnancy and is recommended only for very severe cases. 14 Likewise, azathioprine is another drug that can be used for ITP during pregnancy; however, it is also labelled category C by the US FDA. 14 Vinca alkaloids, mycophenolate, and danazol are teratogenic and are contraindicated in pregnancy. 14
Etiology of thrombocytopenia dependent upon the trimester of presentation.
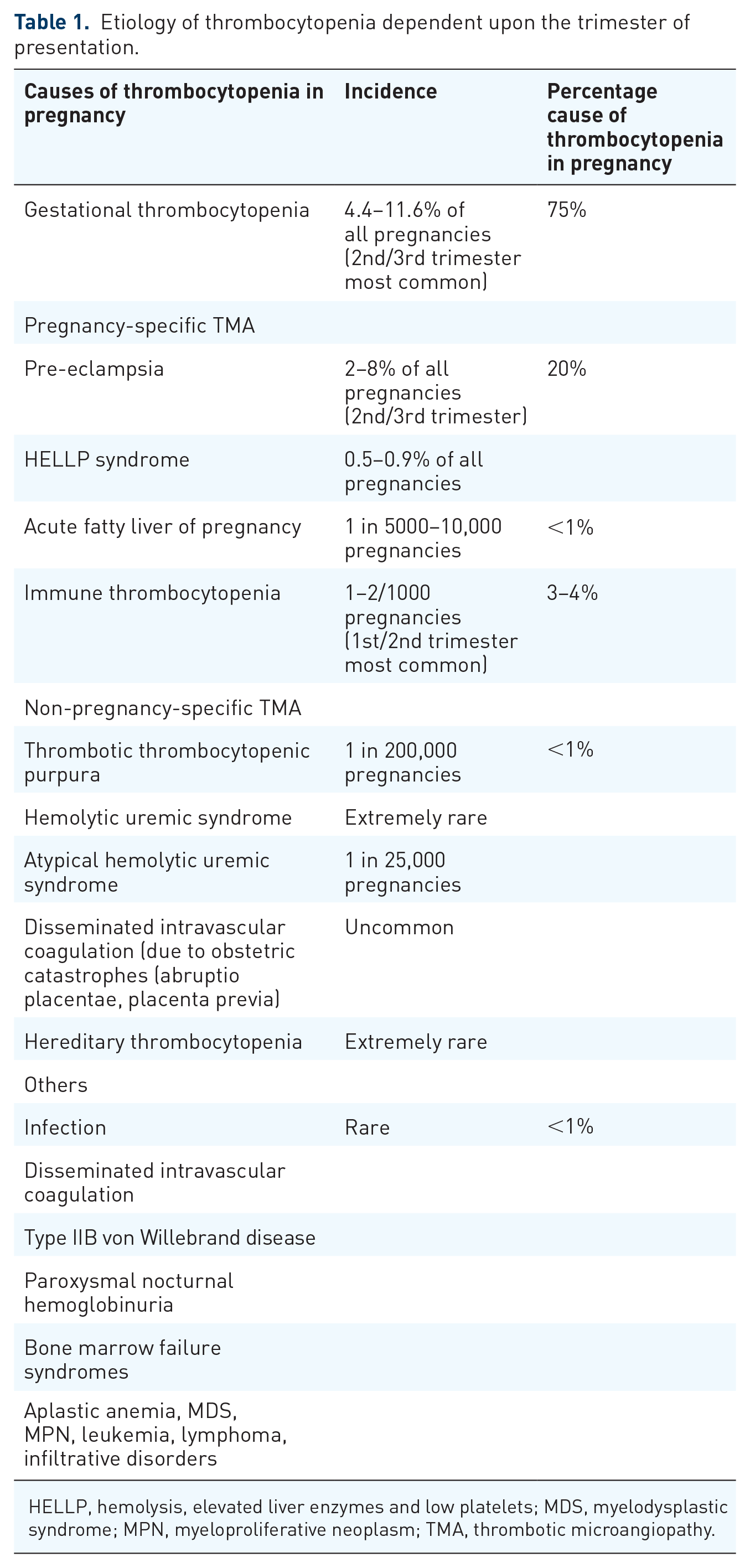
HELLP, hemolysis, elevated liver enzymes and low platelets; MDS, myelodysplastic syndrome; MPN, myeloproliferative neoplasm; TMA, thrombotic microangiopathy.
Thrombopoietin receptor agonists (TPO-RAs) act as thrombopoietin (TPO) mimetics to stimulate megakaryopoiesis in the bone marrow and yield an overall response rate of ~80%.16,17 TPO is a cytokine that regulates megakaryocyte and platelet production via the receptor called myeloproliferative leukemia protein (MPL) or CD110. 18 Thrombopoietin receptor (TPO-R) is a 635 amino acid long protein with an extracellular, transmembrane, and an intracellular or cytoplasmic domain that is expressed on the surface of megakaryocytes, platelets, hemangioblasts, and hematopoietic stem cells (HSCs).18–20 TPO is produced mainly in the hepatocyte either via the stimulation of the Ashwell–Morell receptor by old de-sialylated platelets; 21 or via direct stimulation by interleukin (IL) 6. 22 Unlike erythropoietin, hepatocytes keep producing TPO with no regulation of gene expression. 23 TPO-R plays a critical role in balancing the levels of TPO by binding, internalizing, and then degrading the excess TPO in circulation.24,25 Platelets and megakaryocytes express the bulk of TPO-R. Their large numbers degrade excessive TPO, hence maintain a negative feedback loop to prevent its action on progenitor stem cells.24,26 In patients with thrombocytopenia, high levels of TPO are noted due to insufficient platelet mass. 27 On the contrary, in patients with ITP, the TPO levels remain inappropriately normal or slightly elevated.28–31 Although decreased production of TPO, increased degradation, immune interference with TPO, or increased clearance along with antibody-bearing platelets, or megakaryocytes have been described in the literature, the mechanism for low to normal TPO levels in patients with ITP remains. 32
TPO-RA is labeled as ‘category C’ by the US FDA, which means that animal studies have shown adverse effects on the fetus, but no adequate or well-controlled studies are present in humans. As a result, none of the trials exploring the use of TPO-RAs in adult patients with ITP include pregnant patients or lactating mothers. The recent guidelines from the American Society of Hematology and International Working Group also do not promote the use of TPO-RAs in pregnant patients.13,14 The current literature demonstrating the use of TPO-RAs in pregnancy is limited to off-label use in case reports and case series.33–42 Eltrombopag (Promacta), Avatrombopag (Doptelet), and Romiplostim (Nplate) are approved by the US FDA for adult patients with ITP.43,44 Studies of TPO-agonist antibodies [Minibodies (VB22B sc(Fv)2) and domain subclass-converted TPO agonist antibodies (MA01G4G344)] have not been reported as of yet. In this narrative review, we will review the preclinical and clinical literature associated with the use of TPO-RA in pregnancy and its impact on neonatal thrombocytopenia secondary to maternal immune thrombocytopenia (NMITP). A literature search was conducted using the PubMed electronic database from 1950 to 2018. The MeSH heading and/or text words ‘Romiplostim’, ‘Eltrombopag’, ‘Avatrombopag’, ‘Purpura’, ‘thrombocytopenia’, ‘idiopathic’, ‘thrombopoietin receptor agonists,’ ‘Pregnancy’, and ‘Pregnant’ were used. We also searched the Google Scholar database for any additional reports not listed in the PubMed database. In addition to this, the US FDA website and individual drug websites (Nplate, Promacta, Doptelet) were also searched for references. Finally, the bibliographies of all retrieved articles were examined for additional relevant citations.
TPO-RAs: preclinical data in pregnancy
Eltrombopag
Eltrombopag, developed under the name SB497115, is a non-peptide TPO mimetic belonging to the bioarylhydrazone class of compounds with an empiric formula of C25H22N4O4 and molecular weight of 445.2 D. 45 It has a metal chelation group in the center that binds to the TPO receptor causing phosphorylation and activation of the Janus kinase-2 (JAK-2), signal transducer and activator of transcription 5 (STAT5), mitogen-activated protein kinase (MAPK), and phosphoinositide-3 kinase (PI3K) pathway. 45 It is administered orally at a dose of 50–75 mg per day, achieves a peak concentration in 2–6 h, and has a half-life of 26–35 h in patients with ITP. It is excreted primarily in the feces, followed by urine. In clinical trials, eltrombopag showed a dose-dependent increase in platelet count by day 8–10 in healthy subjects. 45 Eltrombopag shows species specificity and is active only in humans and chimps. 46 Fetal toxicity in animals was seen only at doses whose equivalent doses would be toxic for human beings (Table 2). 47 However, no significant maternal–fetal toxicity was noted at doses that were equivalent to doses currently recommended in humans.47–49 Lactation studies in rats showed the continued presence of the drug in the F1 pup even after 22 h of commencing lactation, indicating that it was secreted in the milk. 47 A registry study in humans to observe the effects of eltrombopag in lactating mothers was launched but failed to recruit any patients in 5 years and was subsequently withdrawn (NCT01055600). 50 Eltrombopag did not affect male fertility in rats even at three times the human equivalent doses. 50 In addition to this, eltrombopag did not compete with TPO and hence had additive effects in combination with the native TPO. 46 Off-target toxicity in the form of cataracts was noted in young rodents when exposed to a dose that was four times the average human exposure. 51 Similar toxicity was also noted in human clinical trials; however, the patients in whom cataracts developed also had numerous other risk factors that predisposed them to develop cataracts (such as prior chronic treatments or use of steroids).48,51
Preclinical data from embryo-fetal developmental studies and lactation studies for eltrombopag, romiplostim, avatrombopag and fostamatinib.

ITP, immune thrombocytopenia; NOAEL, no observed adverse effect level; PND, postnatal day.
Romiplostim
Romiplostim, developed under the name of AMG531, is a 60-kDa recombinant protein called ‘peptibody’ with a molecular formula of C1317H2043N361O395S9.45,52 The molecule consists of a ‘peptide domain’ and an ‘Fc domain’. 45 The Fc portion of the molecule contains IgG1 heavy chains and kappa light chain constant regions bound by disulfide chains. 45 Two identical TPO-peptide sequences are linked to each arm of the Fcγ heavy chain by polyglycine linkers at the C-terminus. 45 In the initial stages of development, the 14-amino-acid long TPO peptide had a very short half-life and would have needed frequent administration to have meaningful clinical use. However, when linked with the IgG1-Fc fragment, the half-life of the drug extended dramatically (120–140 h). 45 It is administered as a subcutaneous injection at a dose of 1–10 µg/kg once every week. In patients with ITP, romiplostim achieves a peak concentration within 7–50 h (median 14 h).45,53 As with other TPO-RAs, romiplostim also showed maternal and fetal toxicity only at doses that were toxic to both humans and maternal test dams (Table 2). 53 However, more severe fetal adverse events such as stillbirth, fetal death, and significant malformations were noted at the toxic doses compared to eltrombopag. Romiplostim binds to the Fc receptor and is expected to be excreted in the milk of lactating mothers. 54 Within the western hemisphere, romiplostim (approved by the US FDA for ITP in 2008) has the longest safety record for the management of patients with ITP. In some case, it has been used for more than a decade. Although TPIAO (a TPO drug developed by 3SBio, a Chinese company), was launched in China in 2006 for chemotherapy-induced thrombocytopenia, it was not approved for ITP until 2011. Nearly 80% of patients on treatment with romiplostim either reduced or discontinued treatment and nearly a quarter permanently discontinued treatment.12,17 This finding correlated well with increased function of Tregs and Bregs; and also increased circulation of tumor growth factor-β, which suggested that TPO-RAs may play a key role in restoring immune homeostasis.12,55 Whether it is a direct effect of TPO-RAs or an immunogenic effect of increased platelet turnover is a matter of further debate.12,55–58
Avatrombopag
Avatrombopag, developed under the name of E5501 (formerly called YM477 and AKR 501), is a small molecule TPO-RA with a chemical formula of C29H34Cl2N6O3S2 and a molecular weight of 649.65 g/mol.59,60 Like eltrombopag, it is another non-peptide TPO mimetic with both in vitro and in vivo activity to increase the platelet count. 61 It is administered orally, with a dose-dependent response in platelets. It reaches peak concentration in the blood within 5–6 h and has a half-life of approximately 19 h. Like eltrombopag, it is also active only in humans and chimpanzees. 61 The clinical review committee approving avatrombopag observed that fetal toxicity was not independent of maternal toxicity and was possibly driven by it. 60 In the prenatal and post-natal studies, in which the drug was administered throughout organogenesis, a 15 mg/kg dose in rats appeared to be safe for both the pup and the dam (Table 2). As avatrombopag was not considered for chronic use at the time of clinical review, the committee labeled it as ‘may cause fetal harm’. In a toxico-kinetic study, a radiolabeled dose of avatrombopag did cross over to the fetus by gestational day 18 and was present in the lactation milk by day 10. 60
Drugs targeting Fc-FcγR interaction and spleen tyrosine kinase pathway
The Major Histocompatibility Complex (MHC)class I-like Fc receptor, neonatal Fc receptor (FcRn), is involved in a pH-dependent salvage pathway that recycles and subsequently prolongs the half-life of IgG. 62 This interaction helps to maintain humoral immunity in humans. However, in patients with autoimmune disorders, this interaction also maintains an abundant quantity of pathogenic IgG, which leads to humoral autoimmunity. 62 Drugs that block the interaction of FcRn and IgG are expected to enhance the degradation of the IgG and are being explored as a potential therapy for ITP. Many molecules, like ARGX-113 (efgartigimod), UCB7665 (rozanolixizumab), etc., are currently in clinical trials for adult patients with ITP. Fostamatinib (R788) is an oral spleen tyrosine kinase (syk) inhibitor that converts to its active metabolite R406 (by intestinal alkaline phosphatase) and blocks the downstream effect of Fc receptor activation in the mast cells and B cells. 63 It is approved as a second-line treatment for adult patients with ITP based on positive results from two randomized controlled trials. 64 Their use in pregnancy is contraindicated based on preclinical data in developmental studies, which show severe urogenital abnormalities in gravid rats and rabbits. 65 The US FDA recommends strict contraception before starting the medication, throughout treatment, and for more than one month after stopping the medication.
Current evidence on the use of TPO-RAs in pregnancy
Since all trials of TPO-RAs in adult patients with ITP have excluded pregnant women and lactating mothers, the current literature is restricted to ‘off-label’ use in pregnant women. Till recently, a ‘Nplate Pregnancy Exposure Registry’ (NCT02090088) was open, which was terminated on 6 January 2015, and the results were never published in a journal. 66 Four patients, who had romiplostim exposure any time during the pregnancy, were registered during the trial period between March 2014 and January 2015, and all of the pregnancies resulted in live births. Adverse events such as preterm delivery, adrenal insufficiency, phimosis, decreased platelet count, and intraventricular hemorrhage were reported in the registry. As the results were never published formally, it is not possible to draw any conclusions regarding a causal effect between romiplostim and these adverse events. Eltrombopag and avatrombopag are pharmacologically active only in humans and chimpanzees. Hence the preclinical data from rats and rabbits cannot be interpreted conclusively for humans.46,49,60 A registry for eltrombopag use in pregnancy, named ‘Promacta Pregnancy Registry’ (NCT01064336 – February 2010–July 2016), listed only one patient and never reported any results.
Kong et al. 67 reported a phase I, prospective study using a novel recombinant thrombopoietin (rhTPO) in pregnant patients with ITP. This was a full length, glycosylated TPO produced by Chinese hamster ovary cells that was almost identical to the endogenous TPO. 67 A total of 31 pregnant patients with ITP who were refractory to IVIG and steroids were enrolled in the trial. The patients enrolled in the trial either had a history of bleeding complications due to thrombocytopenia from ITP or had presented with a platelet count of less than 30 × 109/L. Patients in the first trimester of pregnancy were excluded from the trial. A loading dose of 300 U/kg/day was given for 14 days, followed by sequential maintenance. The rhTPO was discontinued if the platelet count was more than 100 × 109/L. After delivery, the dose of rhTPO was changed to 300 U/kg/week from a daily dose. All patients were followed for 24 weeks, and all 31 neonates were followed for 53 weeks after delivery. Three-quarters of all patients had ITP diagnosed before the start of pregnancy. All patients had some bleeding manifestation, out of whom 10% had a severe bleeding manifestation. A complete response (defined as a platelet count more than 100 × 109/L) was observed in 33% (n = 10), and partial response was observed in 44% (n = 13) of subjects by day 14. In 80% of the patients, bleeding events were resolved by day 14. Although, four patients were deemed non-responders, the authors report improvement in bleeding events in these patients as well. No thromboembolic events or any other significant adverse events were noted in the mothers. Serum anti-TPO antibodies were measured at 4 weeks after starting the treatment, at the end of the treatment, and 6 months after stopping the treatment with rhTPO. Although the authors report that none of the mothers developed anti-TPO antibodies, they also acknowledge that the sample size is too small to derive definite conclusions. 67
Michel et al. 68 reported an international retrospective study of 15 patients (17 pregnancies) who received either eltrombopag (10 pregnancies) or romiplostim (seven pregnancies) for ITP in pregnancy. Eleven patients were diagnosed with ITP prior to the start of pregnancy. Thirteen pregnancies (12 patients) received TPO-RA in the third trimester of pregnancy primarily to prepare for the process of delivery (median 34 weeks of gestation, interquartile range (IQR) 27–39 weeks). Eleven of these 13 pregnancies had minor bleeding manifestations (skin and/or mucosal bleeding). Only one patient had severe gastrointestinal bleeding. The median exposure in these patients was 3 weeks (IQR 1–10 weeks). Three patients receiving eltrombopag for chronic ITP had unexpected pregnancies while on the medication and were exposed to TPO-RAs during the first trimester. Interestingly, it seems from the presented data that these three patients did not receive eltrombopag throughout the pregnancy (median exposure 12 weeks, IQR 9–12 weeks). Two of the three patients received additional treatment with IVIG and corticosteroids, while one patient who was refractory to seven previous lines of treatment did not receive any other treatment. One patient who received romiplostim during the first pregnancy was switched to eltrombopag after delivery of the first neonate and went on to have her second pregnancy while she was on eltrombopag. This was the only patient to receive TPO-RAs throughout the pregnancy (39 weeks). Eight pregnancies reported complete response, six reported partial response, and three pregnancies reported no response. Eleven pregnancies received additional treatment in the form of steroids and IVIG (five reported complete response, four with partial response, and two with no response). No adverse events or thromboembolic events were reported in the mother; however, the data are limited due to the retrospective nature of this study.
Several case reports and small series have reported off-label use of TPO-RAs in pregnant women, which present more granular data regarding the use and adverse events related to TPO-RAs in pregnancy (Table 3). The majority of these patients had ITP (n = 12), and one patient had MYH9 disorder. Except for three patients who started TPO-RA before getting pregnant and chose to stay on it for the entire pregnancy, the medication was started around a median of 30 weeks of gestation (16–36 weeks) and was administered for a median time of 5 weeks (1–24 weeks). All patients who responded to TPO-RA did so within 2–3 weeks of administering the medication. The one patient who was deemed as a non-responder received only a single dose of romiplostim among numerous other agents, including chemotherapy. 40 This patient also developed postpartum hemorrhage (PPH) due to persistent thrombocytopenia. 40 None of the other patients developed PPH due to low platelet counts. Three patients who started TPO-RA before getting pregnant and chose to continue it throughout the pregnancy developed hypertensive crises and placental infarcts. None of the patients on TPO-RA had an abortion or premature delivery. The decision to continue the medication after delivery was made based on platelet counts, in which a few patients were taken off due to high platelet counts. None of the patients experienced hepatic toxicity, signs of marrow failure, or major vessel thrombosis on either eltrombopag or romiplostim. Currently, lactating mothers are advised either to discontinue breastfeeding or the TPO-RA. However, the fact that oral TPO-RA should not be taken within 4–6 h of consuming food (to prevent chelation) raises the possibility that the high calcium content of breast milk would possibly chelate the TPO-RA as well.49,59,69 As there are no overall data on safety for breastfeeding with the use of TPO-RA, lactating mothers are discouraged to breastfeed if using TPO-RA.
Profile of patients and adverse effects associated with the use of thrombopoietin receptor agonists in pregnant patients.
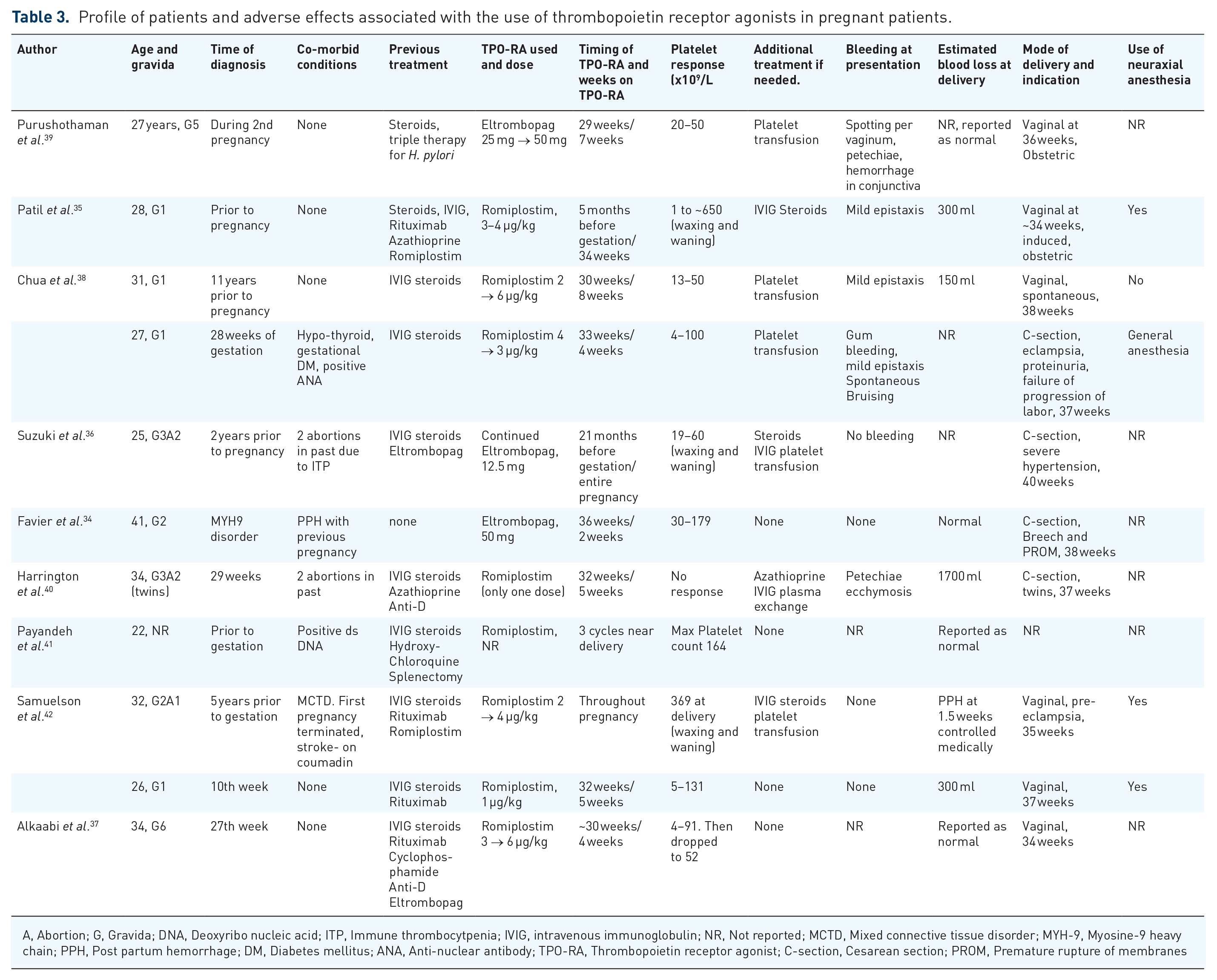
A, Abortion; G, Gravida; DNA, Deoxyribo nucleic acid; ITP, Immune thrombocytpenia; IVIG, intravenous immunoglobulin; NR, Not reported; MCTD, Mixed connective tissue disorder; MYH-9, Myosine-9 heavy chain; PPH, Post partum hemorrhage; DM, Diabetes mellitus; ANA, Anti-nuclear antibody; TPO-RA, Thrombopoietin receptor agonist; C-section, Cesarean section; PROM, Premature rupture of membranes
Neonatal thrombocytopenia associated with maternal ITP
ITP in the mother can lead to neonatal thrombocytopenia and related complications. Up to 25–50% of neonates born to mothers with ITP develop thrombocytopenia.70–72 Out of these, 5–15% are born with platelet counts less than 50 × 109/L, and 1–5% are born with severe thrombocytopenia (platelet count less than 20 × 109/L).1,71–73 A maternal history of splenectomy (done for treating ITP) or a previous pregnancy with ITP that led to thrombocytopenia in the neonate are some recognized risk factors associated with NMITP.1,72–78 The timing of the diagnosis of ITP in the mother (whether diagnosed before or after pregnancy starts) as a risk factor for NMITP remains controversial.79,80 Passive transfer of maternal antibodies across the placenta is the most widely accepted mechanism behind NMITP. However, it must be noted that up to 40% of neonates will test negative for antiplatelet antibodies.72,81 Although breastfeeding is safe for mothers with ITP, prolonged thrombocytopenia (more than 3 months long) in the neonate has been observed in such cases. The reasons remain anecdotal and are attributed to the passive transfer of antibodies in breast milk. 82 A case–control study evaluating prolonged thrombocytopenia in neonates born to mothers with ITP demonstrated the presence of IgA antibodies targeting αIIbβ3 integrin. 83 In neonates born to mothers with ITP, a cord blood sample should be drawn to determine the platelet count.1,10 If the cord blood shows thrombocytopenia, then this should be confirmed with a venous blood sample.10,72 The platelet count usually reaches a nadir by postpartum day 1–5.1,2,10,72 IVIG is the drug of choice and is used when the platelet count drops below 30 × 09/L.1,2 Donor platelets are often transfused along with IVIG to raise the platelet counts quickly.1,10,72,80 Steroids are not frequently used in NMITP to prevent neonatal sepsis. However, if used then they are administered in low doses. 84 Intracranial hemorrhage (ICH) occurs in less than 1% of neonatres with NMITP.1,85,86 All neonates with NMITP exhibiting neurological manifestations indicative of ICH must be evaluated with a head ultrasound. 1 Concurrent NMITP and fetal-neonatal alloimmune thrombocytopenia (FNAIT) must be considered in the differential if a neonate develops ICH and in those born with a platelet count less than 10 × 109/L. 1 A full review of FNAIT is done elsewhere. 87
Current evidence for the use of TPO-RAs in neonates
Kong et al. 67 followed the 31 neonates born during the study period for a median period of 53 weeks (range 39–68 weeks) after delivery. They did not report any difference in the cord blood TPO levels of healthy mothers and mothers with ITP. 67 They also did not report any adverse events such as ICH, severe bleeding, or a platelet count less than 10 × 109/L in the neonates after birth or in the follow-up period. 67 The incidence of low birth weight and premature labor was similar to those treated with conventional treatment in previous studies. 67 It is worth noting that nine out of 31 neonates born to mothers with ITP had a platelet count between 50 and 100 × 109/L, and none was born with a platelet count below 50 × 109/L.67,88 In the retrospective review reported by Michel et al., 68 18 neonates were born from 17 pregnancies (one pregnancy resulted in twins). NMITP was found in six neonates, including the twins from a single mother (median count 14 × 109/L, IQR 4–34 × 109/L). IVIG and platelet transfusions were used for treatment in five out of six neonates with NMITP. One neonate who had thrombocytosis at the time of birth (558 × 109/L) was born to a mother who received a higher than the recommended dose of eltrombopag for 4 weeks (the patient received 100 mg/day; the maximum recommended dose is 75 mg/day). Preterm delivery occurred in five out of 17 pregnancies, and a cesarean section was done in six pregnancies. All the events were attributed to obstetric causes, and none were attributed to TPO-RA exposure in utero. None of the four pregnancies that received TPO-RA during the first trimester reported any adverse outcomes. One death due to genetic malformation (trisomy 8) and one neonate born with pulmonary stenosis had only 1 week’s worth of TPO-RA exposure in utero, that too at the end of the third trimester. On review of all case reports (Table 4), five out of 13 neonates developed thrombocytopenia, and two out of five developed bleeding complications such as intraventricular hemorrhage (IVH) and purpura.35,38 The administration of TPO-RA to the mother did not seem to have any bearing on the prevention of NMITP. IVIG and steroids were used as first-line therapy for NMITP. No babies were reported to have low birth weight, and fetal malformation was reported only in one nenate. The mother of this neonate had a long history of ITP treated with multiple medications (azathioprine, rituximab, steroids, vincristine) and had received romiplostim through her entire pregnancy. 35
Data pertaining to the effects seen in neonates whose mothers were treated with thrombopoietin receptor agonists during pregnancy.

TPO-RA, Thrombopoietin receptor agonist; NMITP, Neonatal-maternal alloimmune thrombocytopenia; IVIG, Intravenous immunoglobulin; IVH, Intraventricular hemorrhage; NR, Not reported
Controversies in the effect of TPO-RA on the fetus and the newborn
The effect of TPO-RA on organogenesis in the human fetus is not clear from the current literature. TPO is known as a critical physiological regulator of hemangioblasts, which eventually differentiate into endothelial and hematopoietic cells.89,90 Excessive TPO exposure has long been speculated as a cause of limb defects in patients with hereditary thrombocythemia, an autosomal dominant disease that occurs either due to the mutation in the TPO gene or the TPO receptor (c-MPL) gene. 91 The germline mutation in the TPO gene results in the removal of ‘inhibitory’ signals, which leads to uninhibited translation of the TPO-mRNA and an increase in TPO production. 91 Although extremely rare, congenital limb defects have been observed in families with hereditary thrombocythemia.91–94 Graziano et al. 91 analyzed the TPO gene of one such patient with hereditary thrombocythemia and congenital unilateral limb defect (proband) and found similar limb defects in his first and third offspring. In 2012, the same group reported another family with hereditary thrombocythemia and limb defects. 92 Due to limb defects being rare among families with hereditary thrombocythemia, genetic background is suspected to be at play in addition to the excessive TPO. On the contrary, in patients with congenital thrombocytopenia due to mutations in homeobox genes (such as HOXA11), limb defects (radio-ulnar synostosis syndrome) have been observed, which raises doubts about the relationship between excessive TPO and limb defects.95,96 In addition to this, no limb defects have ever been reported in families with hereditary thrombocythemia, in which the c-MPL gene was mutated, which again does not support the theory of excessive TPO being the cause of limb defects. 92 From a clinical aspect, it is a well-established fact that all of the approved TPO-RAs cross the placenta in utero to reach the fetal marrow. 88 The current preclinical data suggest fetal harm at doses that were toxic to the maternal dam as well, raising the possibility that the fetal harm may be driven by maternal toxicity rather than the medication itself.49,53 In their phase I study, Kong et al. 67 excluded patients in their first trimester of pregnancy hence preventing exposure of rhTPO during organogenesis. In the data from the case reports compiled for this review, one patient who was administered romiplostim throughout the pregnancy delivered a fetus with malformations. 35 However, it seems that those patients who received TPO-RA after completion of the first trimester did not have an adverse neonatal outcome.
The management of thrombocytopenia in the neonate aims to prevent catastrophic bleeding, particularly ICH. Platelet transfusion is optimal in the setting of acute bleeding secondary to NMITP. However, several studies have noted that ‘liberal’ transfusion of platelets prophylactically is associated with increased morbidity and mortality in neonates.97–100 In the recently concluded PlaNet-2 trial, a higher mortality and bleeding rate was observed in neonates who received platelet transfusion at a platelet count of 50 × 109/L compared to those who received it at a threshold of 25 × 109/L. 101 It is not clear whether the increased mortality is due to the higher platelet counts themselves or transfusion-related issues. Currently, there are no clinical data to support the use of TPO-RA in neonates with thrombocytopenia. In theory, the use of TPO-RA as an alternative to platelet transfusion in neonatal thrombocytopenia seems an attractive option.100,102 However, it usually takes 4–6 days of continuous administration of TPO-RA for the platelets to respond and at least 10–14 days to achieve the maximum response.45,103 Since nearly 80% of severe thrombocytopenia in the neonatal intensive care unit resolve within 14 days,104,105 the use of TPO-RA would be restricted to a minority of neonates who present with ‘persistent thrombocytopenia’ (thrombocytopenia for more than 14 days).100,102 Mahat et al. 106 recently published the first report of using romiplostim in a full-term NMITP. Starting on the 34th day of life, the neonate received escalating doses of romiplostim (1–3 µg/kg/week), which led to normalization of platelets by day 69. 106 Until further evidence evolves, the use of TPO-RA in neonates should be avoided.
Strengths and limitations
The strength of this paper lies in the comprehensive review of literature pertaining to the use of TPO-RA in pregnant patients with ITP. The preclinical evidence presented here has never been explored in any manuscript and shows that although fetal toxicity was demonstrated in animal models, that is either not applicable to humans (as in the case of eltrombopag and avatrombopag) or does not lead to toxicity at human equivalent doses. However, the lack of prospective data and scarcity of information in the retrospective data is the major limitation of this review.
Conclusion
The treatment options for managing thrombocytopenia in pregnant patients with ITP are limited due to concerns for fetal toxicity. Steroids and IVIG are the most widely used drugs in the treatment of pregnant patients with ITP. Our review of the literature suggests that TPO-RAs can help raise the platelet count within 2–3 weeks in pregnant patients with ITP. In light of the existing literature, it seems that the use of TPO-RAs is safe in the second and third trimesters. However, their use during the first trimester when organogenesis is at its peak must be avoided till further evidence demonstrating fetal and maternal safety becomes available. The current literature does not suggest any untoward effect of using TPO-RAs in late pregnancy on the fetus or the neonate. However, there is no clinical evidence to suggest whether it helps in preventing thrombocytopenia in neonates with NMITP or not. There is a pressing need to conduct a prospective clinical trial or a registry study evaluating the use of TPO-RAs in pregnant patients with ITP.
Footnotes
Author contributions
NA: conception of the idea, data collection, data analysis, and interpretation, wrote the manuscript.
AM: Project leader, critical revision of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
No financial support was received for this research, authorship, and/or publication of this article.
Availability of data and materials
The dataset supporting the conclusions of this article are included in the article.