
Abstract
Primary mediastinal large B-cell lymphoma (PMBCL) is a subtype of diffuse large B-cell lymphoma (DLBCL). PMBCL comprises approximately 10% of DLBCLs, thus making it a rare variant of DLBCL. Cure rates for PMBCL with upfront regimens like DA-REPOCH exceed 90%. However, if there is a poor response to this first-line therapy, relapsed/refractory PMBCL (rrPMBCL) has limited treatment options. The historic trend is to treat rrPMBCL with salvage regimens commonly used for DLBCL followed by high-dose therapy and autologous stem cell transplant (HDT-ASCT); however, response rates to salvage therapy remain low and few patients are able to proceed to transplant. An interesting feature of PMBCL is that even though it is classified as a subtype of DLBCL, PMBCL actually shares many clinical, pathologic, and genetic features with classical Hodgkin lymphoma (cHL). For example, both frequently express program death ligand 1 and 2 (PD-L1/2), which is not seen in other mature B-cell lymphomas. The expression of PD-L1/2 in PMBCL makes PDL1 inhibitors, such as pembrolizumab, an attractive therapeutic target. Pembrolizumab is an effective and well-tolerated therapy now approved for a number of cancer types from advanced melanoma to relapsed/refractory cHL. There are now multi-institutional trials underway assessing the role of pembrolizumab in the treatment of rrPMBCL.
Introduction
Primary mediastinal B-cell lymphoma (PMBCL) is a newly recognized B-cell lymphoma currently classified as a subtype of diffuse large B-cell lymphoma (DLBCL). While no standard treatment of PMBCL has been established, with the use of therapy like DA-REPOCH, the 5-year event-free survival (EFS) and overall survival (OS) exceed 90%. However, for those who either do not respond to frontline therapy or relapse, prognosis is dismal with OS at 2 years of 15%. 1 Historically, the approach to relapsed/refractory PMBCL (rrPMBCL) has been similar to that of relapsed/refractory DLBCL with treatment regimens such as DHAP (dexamethasone, cytarabine, cisplatin), ESHAP (etoposide, methylprednisolone, cytarabine, platinum agent), GDP (gemcitabine, dexamethasone, cisplatin), and mini-beam (carmustine, etoposide, cytarabine, melphalan), but with unacceptably low response rates of 0–25%.1,2 PMBCL shares many features with classical Hodgkin lymphoma (cHL) including expression of program death ligands 1 and 2 (PD-L1/2). The binding of PD-L1/2 to its receptor on T-cells, program cell death 1 (PD-1), negatively regulates T-cell-mediated immune events and provides a method for tumor cells to evade the antigen-specific T-cell immunologic response. Pembrolizumab, a PD-1 inhibitor, binds PD-1 and blocks the activation of PD-1 and PD-L1/2 signaling. It is approved for the treatment or relapsed/refractory cHL. Given the expression of PD-L1/2 on PMBCL cells and its known efficacy in cHL, pembrolizumab is now being assessed in patients with rrPMBCL with promising results and good tolerability. In this article we review the current understanding of PMBCL and the emerging role of pembrolizumab as an effective therapy for rrPMBCL.
Background
PMBCL was first described in the 1980s as a mediastinal large cell lymphoma affecting young women with characteristic fibrosis and a propensity to invade surrounding structures such as the pleura, pericardium, and superior vena cava.3–7 In 1994, it was recognized as its own entity by the revised European-American classification of lymphoid neoplasms. 8 In 2008, it was included in the World Health Organization classification of lymphoid neoplasms under mature B-cell lymphomas. 9 However, although it is classified as a subtype of mature B-cell lymphomas, it has unique clinical, pathologic, and genetic features that make it a unique entity of its own.
PMBCL comprises approximately 2–4% of non-Hodgkin lymphomas and 10% of DLBCLs. 10 Unlike DLBCL, it is more common in women in their 30–40s.11,12 It is thought to be derived from medullary thymic B-cells. 13 By histology it is characterized by a diffuse proliferation of medium to large B-cells with surrounding sclerosis. 14 Clinically, it presents as a bulky mediastinal mass with tumors greater than 10 cm found in 70–80% of patients at presentation. 15 Pleural or pericardial effusions are not uncommon and up to one-half of patients show signs or symptoms of superior vena cava syndrome.4–6,15 Bone marrow infiltration and extranodal sites of involvement are rare at presentation. 11 However, at the time of recurrence, extranodal sites of disease are common and include areas such as the kidneys, adrenal glands, liver, ovaries, and central nervous system (CNS). 16
PMBCL is molecularly different from DLBCL. It expresses pan B-cell antigens CD19, CD20, CD22, and CD79α and B-cell transcription factors BOB1, OCT2, PAX5. 17 However, it usually does not express surface immunoglobulins like other DLBCLs.7,17 Additionally, CD30 expression is seen in over 80% of PMBCL, but CD15 is usually absent. 18 It has variable expression of bcl2 and bcl6, and in contrast with other subtypes of DLBCL, bcl2, bcl6, and myc rearrangements are usually absent. 19 The differential diagnosis includes cHL and mediastinal grey zone lymphoma.
Although it is classified as a variant of DLBCL, it shares many common features with the cHL subtype, nodular sclerosing Hodgkin lymphoma (nsHL).20–22 Both commonly present as a mediastinal mass in young adults. By histology both have variable numbers of malignant cells within an inflammatory infiltrate suggesting immune evasion by the tumor cells. The large B-cells in PMBCL may have round or lobulated nuclei with an abundant cytoplasm, which can sometimes resemble Hodgkin/Reed–Sternberg cells. 17 Surface immunoglobulin expression is usually absent in both types of lymphomas. Additionally, as mentioned previously, PMBCL commonly expresses CD30, although weaker and more heterogeneously than cHL.18,21 In fact, gene expression profiling looking at signature genes expressed by HL and PMBCL showed that PMBCL shares one-third of its genes with nsHL. 21 These signature genes were not expressed by other subtypes of DLBCL. 21 A highly expressed gene that was common to both PMBCL and HL was PDL2. 21
Frontline treatment of PMBCL
Initially, the treatment of PMBCL consisted of anthracycline-based high intensity chemotherapy with consolidative radiation with overall response (OR) rates of greater than 60% after chemotherapy, which increased to greater than 80% after administration of consolidative radiation.23,24 However, concern for the long-term effects of radiation emerged. The increased risk of coronary artery disease and breast cancer in women have been well established in patients treated with radiation for HL and prompted the development of regimens such as DA-REPOCH (dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) administered without radiation.25–27 In the phase II, prospective study of 51 patients with newly diagnosed PMBCL given DA-REPOCH without routine consolidative radiation, the 5-year EFS and OS rates were 93% and 97% respectively. After follow up ranging from 10 months to 14 years, only 2 of the 51 patients (4%) had residual focal disease on positron emission tomography(PET)-computed tomography (CT). These two patients received radiation and were also subsequently disease-free. Similar results were seen in a retrospective study of 16 patients with PMBCL treated at Stanford with DA-REPOCH alone with a complete response (CR) rate of 100% at a median follow up of 37 months. 27 Given that only two patients required radiation from both trials, it suggests that the use of DA-REPOCH may decrease the need for radiotherapy. 27 Future trials incorporating PET may help delineate when radiation will be beneficial or whether lower doses of consolidative radiation may help improve EFS in PMBCL.
Treatment for relapsed/refractory PMBCL
It is believed that patients with PMBCL who do not relapse after 18 months of initial treatment are likely cured, as relapse usually occurs within the first 12–18 months.2,23,28 Optimal therapy for relapsed/refractory disease has not been well defined. For localized relapse confined to mediastinum, local radiation can be curative. 27 For nonlocalized relapse, second-line strategies have been similar to those used in DLBCL and include re-induction with noncross-resistant agents (such as rituximab, ifosfamide, carboplatin, etoposide (RICE), DHAP, or others) followed by consolidation high-dose therapy (HDT) and autologous stem cell transplant (ASCT).2,29,30 However, response rates to salvage therapies are unacceptably low. In a study of 99 patients with newly diagnosed PMBCL treated with doxorubicin-containing chemotherapy, 35% relapsed or had refractory disease. Of the 35%, none of the patients with primary refractory disease and only 22% of those with relapsed disease responded to salvage chemotherapy. 2
There are only a few small retrospective studies looking at ASCT in rrPMBCL. A study looked at 35 patients treated with high-dose cyclophosphamide, carmustine,etoposide (CBV) followed by ASCT. A total of 23 of the 35 patients had rrPMBCL (11 had relapsed disease and 12 had primary refractory disease). At the time of ASCT, 4 of the 11 patients with relapsed disease were chemotherapy-responsive. For the patients with refractory disease, 8 of the 12 patients remained refractory, 2 achieved a CR, and 2 achieved a partial response (PR). The 5-year progression free survival (PFS) for those with relapsed disease and refractory disease was 27% and 58% respectively. The strongest predictor of PFS was chemotherapy responsiveness immediately prior to transplantation. Patients with chemo-responsive disease had a 5-year PFS of 75% compared with 33% with chemo-resistant disease. 30 A small retrospective study conducted in Japan included 44 patients with rrPMBCL treated with HDT followed by ASCT. In this study, the OR rate was 77% with 64% achieving a CR. The median follow up was 54 months. The 4-year OS and PFS were 70% and 61% respectively. 31 For patients with relapsed disease compared with primary refractory disease, OS at 4 years was 73% and 65% respectively. Additionally, the 4-year OS and PFS was 80% and 69% respectively for those with chemo-sensitive disease compared with 50% and 45% respectively for those with chemorefractory disease. 31
Studies suggest that in comparison with DLBCL, fewer patients with rrPMBCL than DLBCL respond to salvage chemotherapy, but for those who do respond, the outcomes of ASCT in the relapsed setting may be similar. A retrospective study compared outcomes of salvage chemotherapy followed by ASCT in 37 patients with rrPMBCL with a control group of 143 patients with rrDLBCL. The OR rate to salvage chemotherapy (DHAP, ESHAP, GDP, and mini-Beam) was 25% for those with PMBCL and 48% for those with DLBCL. A total of 65% of patients with PMBCL and 34% of patients with DLBCL received a second line of salvage chemotherapy. However, although only 22% of patients with PMBCL and 50% of those with DLBCL were able to proceed to ASCT, there was no significant difference in the 2-year post-ASCT OS or PFS rates (67% and 53%, and 57% and 36% respectively). 28
Regardless of this, response rates of rrPMBCL patients to current salvage chemotherapy are unacceptably low and new therapeutic strategies are needed.
Programmed cell death ligand expression in PMBCL
As mentioned previously, cHL and PMBCL share many common characteristics. Both cHL and PMBCL have a similar gene expression profile and both harbor genetic alterations of chromosome 9p.21,32–34 Specifically, 9p24.1 has been shown to be amplified in 53–70% of PMBCL cases and 30–40% of cHL cases, but rarely in DLBCL.35–38 This region contains the genes for PD-1 ligands, PD-L1 and PDL-2, separated by 42 kilobases. 35 In both PMBCL and cHL, amplification of 9p24.1 has been shown to be associated with both increased PD-L1/2 transcripts and cell-surface protein expression.35,36 Expression of PD-L1 is found in 30–80% of PMBCL cases.37,39 PD-L2 protein expression has been shown to be particularly increased in PMBCL.21,35,36,40 In comparison, 70–87% of cHL and 31–57% of DLBCL express PD-L1.36,39,41 Additionally, the 9p24.1 chromosome has been found to be rearranged in 20% of PMBCL cases. 38 In another pathology study by Shi and colleagues, 72% of PMBCL cases expressed PD-L2 but only 3% of other DLBCL cases. 36 PD-L1 and PD-L2 transcripts have been shown to be elevated in PMBCL regardless of whether the locus was rearranged or amplified suggesting alternative mechanisms of regulation.36,38 In normal cells, PD-1 ligand activation is induced by cytokine-mediated signaling activated by the Janus kinase 2/signal transducer and activator of transcription (JAK2/STAT) pathway. 35 The JAK2/STAT pathway regulates the transcription of genes that influence both cell proliferation and apoptosis and has been implicated in the pathogenesis of a number of hematologic malignancies. 42 JAK2 is also found within the 9p24.1 band, 322 kilobases upstream from the PD-L1 gene. 35 It has been shown to also be co-amplified with the PD-L1/2 loci in both PMBCL and cHL cell lines.35,43 Amplification of JAK2 has been shown to be associated with increases JAK2 protein expression and activated (phosphorylated) JAK2 protein. Activated JAK2 protein further activates PD-L1/2 expression in PMBCL and cHL. 35 JAK2 inhibition has been shown to specifically decrease PMBCL growth in vitro and in vivo suggesting another possible therapeutic target. 44
Pembrolizumab background
PD-1 was first recognized in the early 1990s after it was found to be expressed by a T-cell hybridoma upon induction of apoptosis.45,46 The binding of PD-1 to its receptor, PD-L1, on dendritic cells and macrophages negatively regulates T-cell-mediated immune events.47–50 It was found that various tumor types express PD-L1, and that activation of PD-1/PD-L1 signaling serves as a method for tumor cells to evade the antigen-specific T-cell immunologic response.51,52 Thus, it was reasoned that the blocking of PD-1/PD-L1 signaling could be an effective cancer therapy. The results of several phase I studies looking at humanized monoclonal immunoglobulin (Ig)G4 antibodies to PD-1 and PD-L1 in solid tumors inspired the development of the first PD-1 inhibitors, nivolumab and pembrolizumab.53–55 Pembrolizumab is a humanized monoclonal IgG4 antibody to PD-1, which blocks binding to its ligands PD-L1 and PDL2. It was first approved for the treatment of advanced or metastatic melanoma in September 2014 based on the findings from the KEYNOTE-001 study. 56 Since then, PD-1 and PD-L1 inhibitors have been approved for the treatment of a wide variety of malignancies from malignant melanoma to HL.56,57
As previously discussed, classical Hodgkin Reed–Sternberg cells have been shown to express varying levels of PD-L1, while both the tumor-infiltrating T-cells and peripheral T-cell express high levels of PD-1.39,41,58 Nivolumab was the first PD-1 inhibitor to be approved for hematologic malignancies based on the findings from the CheckMate039 and CheckMate205 studies showing response rates of 87% and 66% respectively.59,60 Shortly thereafter, pembrolizumab was approved for the treatment of relapsed/refractory cHL in March 2017 based on the KEYNOTE-087 trial showing an OR rate of 69%. 60
Pembrolizumab in relapsed/refractory PMBCL
The finding that PMBCL, like cHL, also express PD-1 ligands prompted an initial multicenter, international phase Ib study of pembrolizumab in patients with rrPMBCL (Keynote-013), which is currently ongoing. 61 Eligible patients were those with relapsed/refractory PMBCL who had either relapsed after, or were ineligible for, ASCT. The first 11 of 19 patients enrolled in the trial received pembrolizumab at a dose of 10 mg per kg every 2 weeks. Subsequent pharmacokinetic and pharmacodynamics studies showed equivalence of pembrolizumab drug exposure with either weight-based or fixed dosing. 62 Consequently, the subsequent eight patients received a fixed dose of pembrolizumab 200 mg every 3 weeks. Treatment was continued for up to 2 years, or until unacceptable toxicity or confirmed disease progression. Treatment response was assessed by PET CT at 6 and 12 weeks, and then every 9 weeks thereafter. Primary endpoints were safety and OR rate by investigator assessment. Secondary end points included CR, duration of response, and time to subsequent lymphoma therapy.
Of the 19 patients enrolled, 17 patients were included in the efficacy analysis population (1 patient withdrew prior to receiving any doses and 1 patient did not receive the primary response assessment by time of data cutoff). The median age of patients was 30 years. A total of 72% were women. Patients were heavily pretreated with 61% having had received three or more prior lines of therapy and 33% having had prior ASCT. Overall, 41% (7/17) of patients responded. There were two patients that achieved a CR, five patients achieved a PR, and six patients had stable disease (SD). A total of 81% of patients had an overall decrease in their target lesions. At a median follow up of 11 months, the median duration of response was not reached, and six of the seven responses were ongoing. None of the responders received an ASCT. Overall, 10 patients discontinued treatment (5 due to the progression of disease based on imaging, 4 due to clinical progression, and 1 due to physician decision). The two patients who responded reached the maximum 2 years of treatment before data cutoff and remained in remission. All patients with an objective response were alive at the time of data cutoff (Table 1).
Relapsed/refractory PMBCL treated with salvage regimen.

ASCT, autologous stem cell transplant; CR, complete response; ORR, overall response rate; PMBCL, primary mediastinal large B-cell lymphoma; PR, partial response; RT, radiotherapy; SD, stable disease.
Pembrolizumab was well tolerated. A total of 61% had treatment-related adverse events (TRAEs) that were mostly grade 1–2. Overall, six patients had serious adverse events, but none discontinued treatment due to adverse events. The most common TRAEs were hypothyroidism, diarrhea, nausea, fatigue, pyrexia, and decreased appetite. The only grade 3 adverse event was neutropenia, and the only grade 4 adverse event was veno-occlusive liver disease after allogeneic stem cell transplant (SCT), at which time the pembrolizumab had been discontinued. The only potential immune events were 1 grade 2 diarrhea and 1 grade 2 radiation pneumonitis. The positive results from this study prompted a global, multicenter, phase II trial (KEYNOTE-170) evaluating the efficacy of single-agent pembrolizumab in heavily pretreated rrPMBCL patients.
The KEYNOTE-170 trial is an ongoing, multicenter, phase II trial of patients with rrPMBCL. In this trial, patients must have either failed ASCT or have failed two or more prior lines of therapy and were ineligible for ASCT.63,64 Patients were treated with pembrolizumab 200 mg intravenously (IV) every 3 weeks. Treatment was continued until either unacceptable toxicity or documented disease progression. For those without toxicity or disease progression, it was continued for up to 2 years. The primary endpoint was the OR rate assessed by a blinded independent central review. Secondary endpoints included the OR rate by investigator review and adverse events.
A total of 49 patients were evaluable in the interim results with a median age of 33 years. Patients were heavily pretreated and had received a median of three prior lines of therapy. Overall, 70% of patients had chemorefractory disease and were thus not eligible for ASCT. Similar to the phase I study, the OR rate was 41% by blinded independent central review (38% by investigator assessment). At the time of data analysis, 14% achieved a CR, 28% achieved PR, and 10% had SD assessed by independent review. A total of 28% had progression of disease and 21% were not assessable for response evaluation. The median time to response was 2.9 months. At an average follow up of 6.6 months, median duration of response and OS were not reached. At 1 year, 62% were still alive. Of all patients, 59% were positive for PD-L1 (4% were negative and 37% were unknown). Of those who responded, 76% were positive for PD-L1 (3% were negative and 21% were unknown).
Pembrolizumab was well tolerated with 1 year OS of ~60%.63,64 Approximately 40% of patients had a response to pembrolizumab.63,64 There were adverse events with 25% serious and over 50% were treatment-related.63,64 Overall 35% experienced serious adverse events and 53% experienced TRAEs. Based on the positive results of this trial, in June 2018, pembrolizumab was granted accelerated approval by the United States Food and Drug Administration (US FDA) for use in rrPMBCL patients who have progressed after two or more lines of prior therapy. 64
These studies both show OR rates of 41% with pembrolizumab salvage therapy. This is higher than the prior retrospective studies using regimens traditionally used for DLBCL (DHAP, ESHAP, GDP, and mini-beam), which have shown OR rates ranging from 0 to 25% in rrPMBCL patients.2,28,30 Although the PFS rates for rrPMBCL patients following ASCT can be as high as 67–80%, this has only been shown for those with chemotherapy-sensitive disease.28,30,31 The strongest predictor of PFS for ASCT was chemotherapy responsiveness immediately prior to transplantation. 30 For those who do not respond to chemotherapy prior to ASCT, long-term disease-free survival rates range from 33% to 45%.30,31 Novel therapies for rrPMBCL are desperately needed as response rates to salvage regimens traditionally used in patients with DLBCL are unacceptably low.
Combination therapy with immune checkpoint inhibitors
Preclinical and clinical studies in both solid tumors and hematologic malignancies have suggested that combination immune checkpoint inhibitors and immune checkpoint inhibitors combined with other therapeutic agents may have synergistic effects.65–72 In relapsed or refractory HL (rrHL), the combination of nivolumab with brentuximab vedotin (BV) has shown an OR rate of 82–89% and a CR rate of 50–61%.71,72 The OR and CR rates using the combination therapy were higher than with either nivolumab or BV alone.60,73 In a cohort of the previously mentioned CheckMate039 study, patients with relapsed or refractory hematologic malignancies were treated with nivolumab and ipilimumab. For the patients with rrHL, the OR rate was 74% with a CR of 19%. 74 Given the success of these combination therapies, as well as the similarities between cHL and PMBCL, several studies utilizing combination therapies in patients with PMBCL are underway. Additionally, given the high response rates in the relapsed or refractory setting, there are efforts to improve clinical outcomes by moving immune checkpoint inhibitors to the frontline setting.
Numerous clinical trials assessing combination therapies with pembrolizumab in B-cell lymphomas, including PMBCL, are underway. In one trial, patients with untreated DLBCL or grade 3b follicular lymphoma are being treated with frontline pembrolizumab and combination chemotherapy (ClinicalTrials.gov identifier: NCT02541565). In the relapsed/refractory setting, pembrolizumab is being given in combination with therapies such as tisagenlecleucel, vorinostat, ibrutinib, dendritic cell therapy and cryosurgery, and rituximab (Table 2). Several studies utilizing nivolumab combination therapies are also currently underway in both the frontline and relapsed or refractory settings (Table 3). Other studies targeting pathways unique to rrPMBCL, have been completed or are ongoing, including therapies targeting CD30 and the JAK/STAT pathway.76–78
Ongoing clinical trials utilizing pembrolizumab in PMBCL.
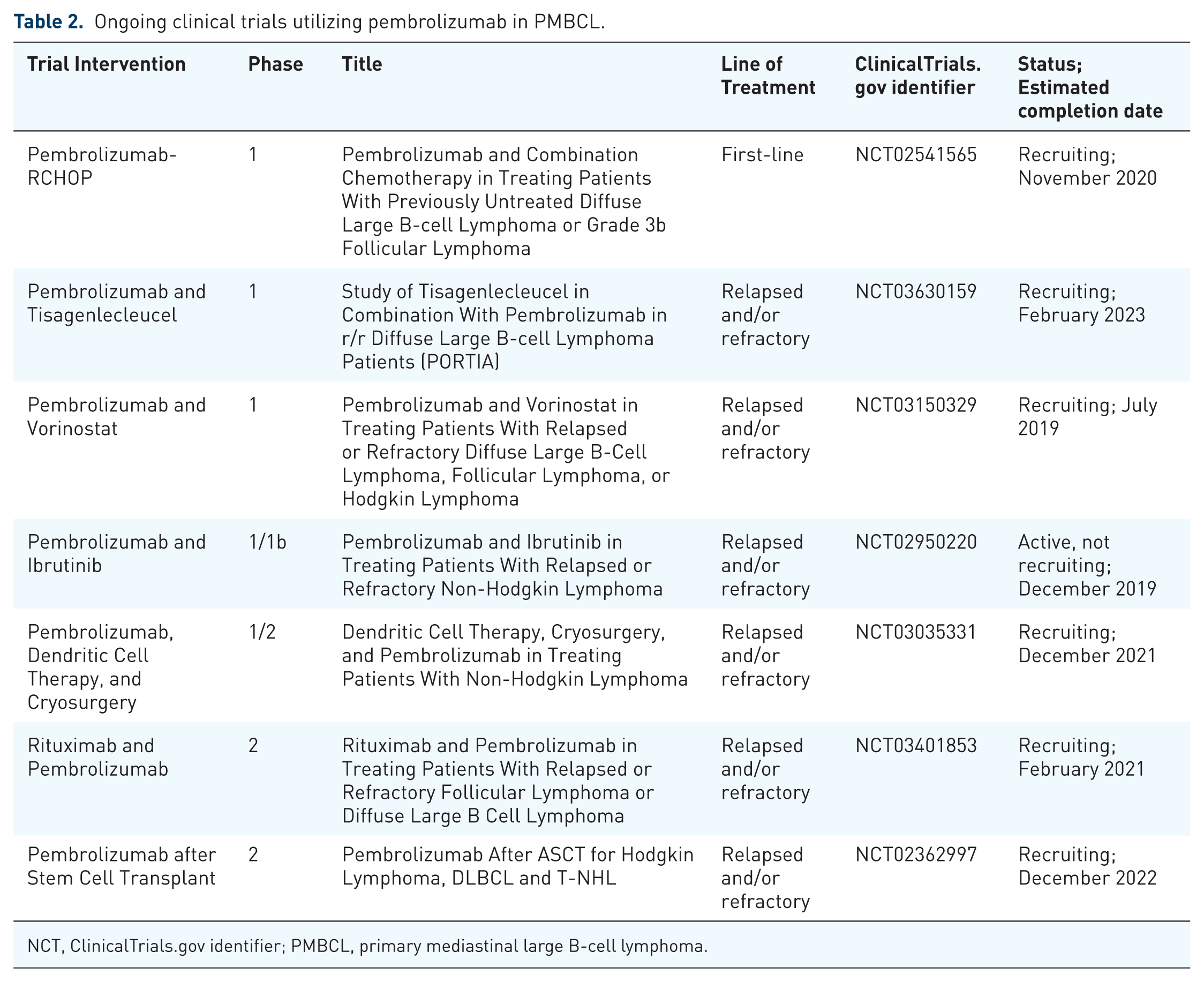
NCT, ClinicalTrials.gov identifier; PMBCL, primary mediastinal large B-cell lymphoma.
Ongoing clinical trials utilizing nivolumab in PMBCL.
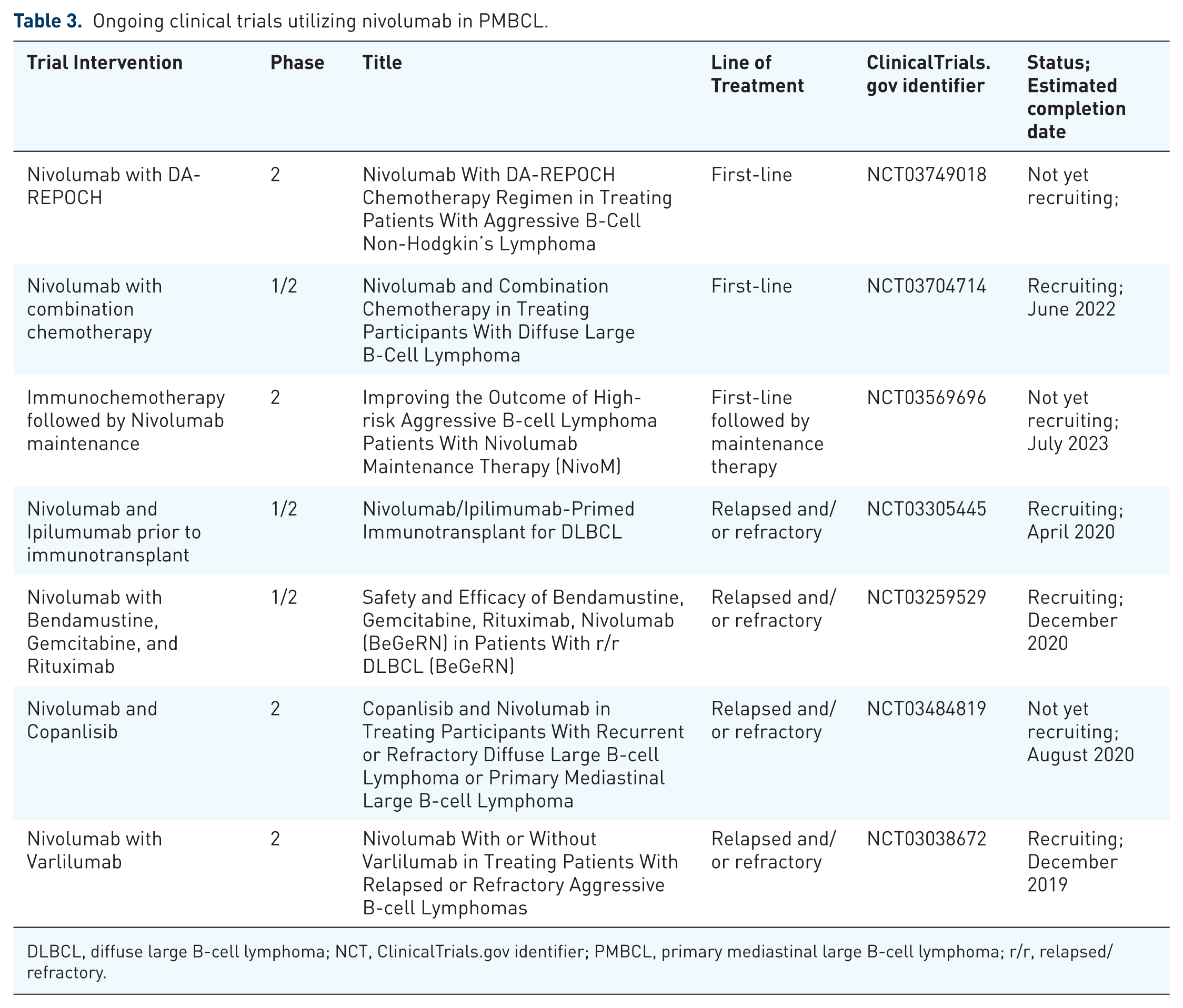
DLBCL, diffuse large B-cell lymphoma; NCT, ClinicalTrials.gov identifier; PMBCL, primary mediastinal large B-cell lymphoma; r/r, relapsed/refractory.
Other targeted therapies for relapsed/refractory PMBCL
As previously discussed, 80% of PMBCL expresses CD30 suggesting a potential benefit from therapy targeting CD30. BV, a chimeric CD30-specific IgG1 antibody conjugated to the microtubule-disrupting agent, monomethyl auristatin E (MMAE) is approved for cHL and anaplastic large B-cell lymphomas, both of which express CD30. 75 Thus, a single-arm phase II trial looking at the use of BV in rrPMBCL patients was conducted. 76 In this study, BV was administered at a dose of 1.8 mg per kg as a single IV infusion on day 1 of each 21-day cycle. A total of 15 patients were enrolled in five Italian centers with a median age of 29 years. Patients were heavily pretreated with a median of three prior treatments. Overall, 12 patients (80%) had disease that was refractory to the last therapy prior to BV. All patients had received rituximab, eight patients (53%) received ASCT, and nine patients (60%) received radiation. The OR rate was 13.3% (2/15) with no patients achieving a CR. Overall, two patients achieved a PR and one patient had SD. The remaining 12 patients (80%) had progression of disease. Given this low OR rate, the study was terminated early.
As mentioned previously, another potential therapeutic target in PMBCL is the JAK/STAT pathway. The JAK2 2 inhibitor, ruxolitinib, and the JAK2/FLT3 inhibitor, SB518, have both been evaluated in HL and PMBCL. However, no conclusion has been made regarding their efficacy due to the low number of cases thus far.77,78
Conclusion
PMBCL is distinctly different from other mature B-cell lymphomas and further studies of effective salvage therapies are needed. Although classified as a subtype of DLBCL, PMBCL is clinically, genetically, and molecularly different from other mature B-cell lymphomas and shares many common features with cHL. Relapsed/refractory PMBCL has a dismal prognosis and consequently attention has been aimed at curative therapy in the frontline setting. With the institution of infusion regimens like DA-REPOCH, more than 90% of patients are cured. Few studies have looked at the efficacy of salvage regimens in rrPMBCL. Commonly used salvage therapies have been similar to those used for DLBCL such as DHAP, ESHAP, GDP, transplant, and more. Several small retrospective studies have shown poor response rates of only up to 25% with these therapies. The genetics of PMBCL are similar to cHL, which suggests that it may respond better to therapies traditionally used in cHL. Pembrolizumab has shown efficacy to cHL and is approved for the treatment of relapsed/refractory HL. Initial phase I and IIb studies assessing its efficacy in rrPMBCL have shown response rates of 41%. Additionally, pembrolizumab is well tolerated with few grade 3 or 4 adverse events. Additionally, combination therapies utilizing pembrolizumab may increase the efficacy and response rate and are currently underway.