
Abstract
Objective
Primary mediastinal B-cell lymphoma (PMBCL) lacks standard treatment regimens. This study aimed to identify the disease’s clinical features and prognostic factors.
Methods
This retrospective study included 56 patients with PMBCL. Patient demographic details and clinicopathological characteristics were summarized, and their effects on progression-free survival (PFS) and overall survival (OS) were analyzed.
Results
The median patient age was 29 years (range, 14–56). Twenty-two patients received DA-EPOCH-R (dose-adjusted etoposide, vincristine, and doxorubicin for 96 hours with bolus doses of cyclophosphamide and oral prednisone, as well as rituximab), and 34 patients received R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone). Clinical/laboratory parameters, overall response rates, and 5-year PFS and OS rates did not differ between the treatment groups. Kaplan–Meier analysis indicated that late-stage disease and a higher International Prognostic Index (IPI) were associated with shorter PFS and OS. Furthermore, patients with B symptoms and first-line treatment non-responders exhibited worse OS. 18Fluorodeoxyglucose-positron emission tomography/computed tomography quantitative parameters, such as higher metabolic tumor volume (MTV) and total lesion glycolysis (TLG), were corrected with shorter PFS.
Conclusions
This study revealed that stage IV disease, higher IPI, and B symptoms were poor prognostic factors in patients with PMBCL. Significantly, higher MTV and TLG portended worse PFS.
Keywords
Introduction
Primary mediastinal B-cell lymphoma (PMBCL) is a distinct subtype that accounts for approximately 2% to 3% of all cases of non-Hodgkin B-cell lymphoma. 1 PMBCL displays a female predominance with a median age at diagnosis of 30 years, and it is characterized by a large mass on the mediastinum at disease onset. 2 PMBCL has a unique clinical paradigm, as its molecular characteristics more strongly resemble Hodgkin lymphoma rather than diffuse large-B cell lymphoma. PMBCL carries a high possibility of cure following standard anthracycline-containing chemoimmunotherapy, but prognosis is worsened if adequate responses are not rapidly achieved or if the disease recurs. 3 Because of the relatively rare incidence of the disease and the absence of prospective, randomized controlled clinical trials, the optimal first-line treatment modality has not been defined. R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) with or without consolidative radiotherapy was initially the standard treatment regimen for the disease. However, a phase II study highlighted the strong efficacy of DA-EPOCH-R (dose-adjusted etoposide, vincristine, and doxorubicin for 96 hours with bolus doses of cyclophosphamide and oral prednisone, as well as rituximab) in patients with PMBCL without a need for mediastinal radiation. 4
Factors predicting the outcome of therapy remain unavailable. Several studies proposed that the International Prognostic Index (IPI), the presence of pleural or pericardial effusion, and certain molecular markers such as C-MYC and BCL2 might serve as prognostic factors for PMBCL.5,6 However, these conclusions require further verification.
18Fluorodeoxyglucose-positron emission tomography/computed tomography (18FDG-PET/CT) has long been an imaging tool for lymphoma staging. 7 It also has value in predicting diagnosis, evaluating treatment response, and providing prognostic information for lymphoma and other solid tumors.8–11 To date, the quantitative parameters of 18FDG-PET/CT have been investigated in several lymphoma entities, including PMBCL, illustrating its prognostic value.12–14
In the current study, we retrospectively reviewed a cohort of patients with PMBCL to provide insights into treatment modalities and the prognostic utility of certain clinical characteristics, as well as clarify the features of 18FDG-PET/CT. The results both corroborated several putative prognostic factors described by other researchers and revealed previously unrecognized indicators that can be assessed by 18FDG-PET/CT.
Materials and methods
Patients
We performed a computer-assisted search of the Fudan University Shanghai Cancer Center pathology files and clinicopathological database of patients with PMBCL treated in the Department of Medical Oncology from January 2008 to April 2020. All patients were pathologically confirmed to have PMBCL, and all pathological results were reviewed by experienced pathologists in the Department of Pathology, Shanghai Cancer Center. Our study was approved by the Ethics Committee of the Fudan University Shanghai Cancer Center (2 January, 2017; approval number: IRB1612167-18), and written informed consent was obtained from all subjects. This study conforms to the relevant STROBE guidelines. 15 We have de-identified all patient details in the study. For each patient, the following data were collected: demographics, presence of superior vena cava syndrome at disease onset, size of the mass, Ann Arbor stage, IPI, Eastern Cooperative Oncology Group (ECOG) performance score (PS), pathological and imaging parameters, laboratory data, type of treatment, and survival status.
18F-FDG PET/CT was performed using a Biograph mCT Flow PET/CT scanner (Siemens Healthcare, Erlangen, Germany) according to standard clinical scanning protocols. All patients fasted for at least 6 hours before the scan, and none had a blood glucose level >8.7 mmol/L. A whole-body scan was acquired approximately 1 hour after the intravenous administration of 5.18 MBq/kg 18F-FDG. CT was performed first (120 kVp, 0.33 s/rotation, CARE Dose 4D, pitch = 1) using a slice thickness of 3 mm and reconstructed into a 512 × 512 matrix (voxel size = 0.98 ×0.98 × 3 mm3). Then, PET was performed with a speed of 1.8 mm/s, and the TrueX and TOF algorithms (two iterations, 21 subsets, and 5 mm full width at half maximum) without filtering and smoothing were used to reconstruct the PET images. For all PET reconstructions, the matrix size was 200 × 200, resulting in anisotropic voxels of 4.07 × 4.07 × 3 mm3. The PET images were converted into standardized uptake values by normalizing the activity concentration to the dosage of injected 18F-FDG and patient body weight.
Statistical analysis
All analyses were performed using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA). The χ2 test was used to compare clinical and laboratory data between the treatment groups. Overall survival (OS) was measured from the date of diagnosis to the date of death attributable to any cause or the last date of follow-up. Progression-free survival (PFS) refers to the period from the beginning of treatment to disease progression or death of any cause. For survival analyses, Kaplan–Meier survival curves were constructed, and differences were tested by the log-rank test. The data of patients alive at the end of the study were censored. All P values were two-sided, and the results were considered significant at P < 0.05.
Results
Patient characteristics
Fifty-six consecutive patients were enrolled in the study, including 24 (42.9%) male and 32 (57.1%) female patients, and all patients were hospitalized. The median patient age was 29 years (range, 14–56) at the time of diagnosis. According to the Ann Arbor staging criteria, 53 (94.6%) patients had stage I/II disease, whereas three (5.4%) patients had stage IV disease. IPI (including age > 60, ECOG PS > 2, stage III or IV, elevated lactate dehydrogenase [LDH] level, and >1 extranodal site) was determined in all patients as follows: IPI = 0, 18 (32.1%); IPI = 1, 35 (62.5%); and IPI ≥2, 3 (5.4%). Patients with PMBCL have a wide clinical spectrum but typically present with mediastinal masses. The symptoms of PMBCL in our study were non-specific, including chest distress, chest pain, cough, edema, and asthenia. Concerning the laboratory findings, 36 (64.3%) patients had elevated LDH levels, and 22 (39.3%) patients presented with B symptoms. Basic features of the patients concerning clinical and laboratory parameters were recorded (Table 1).
Baseline characteristics of 56 patients with primary mediastinal B-cell lymphoma.
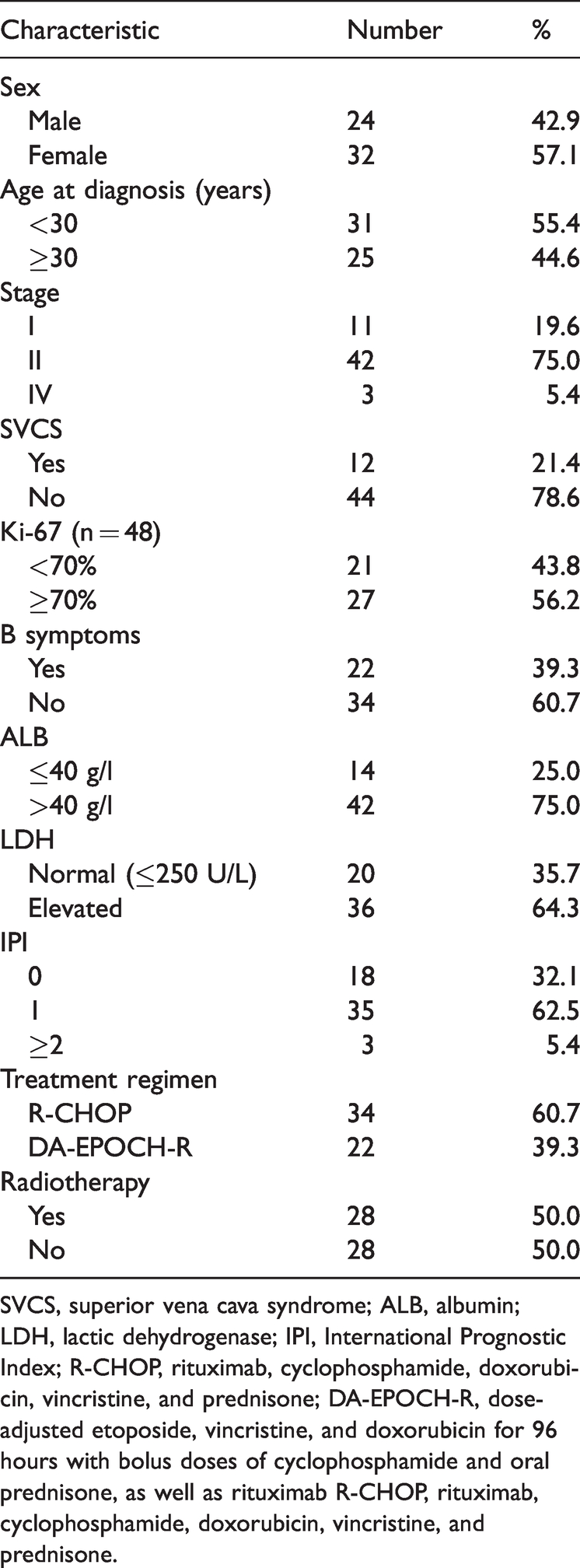
SVCS, superior vena cava syndrome; ALB, albumin; LDH, lactic dehydrogenase; IPI, International Prognostic Index; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; DA-EPOCH-R, dose-adjusted etoposide, vincristine, and doxorubicin for 96 hours with bolus doses of cyclophosphamide and oral prednisone, as well as rituximab R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Treatment and response
Survival data were available for a median follow-up of 1072 days (range, 182–3648 days). After the diagnosis of PMBCL, 22 patients received DA-EPOCH-R, and 34 received R-CHOP. There were no statistically significant differences of clinical and laboratory parameters between the two treatment groups (Table 2). The overall response rate was 100% for DA-EPOCH-R, versus 91.2% for R-CHOP. In total, 59.1% (13/22) and 41.2% (14/34) of patients achieved complete remission in the DA-EPOCH-R and R-CHOP groups, respectively. In the DA-EPOCH-R group, 31.8% (7/22) of patients received radiotherapy following six cycles of treatment after achieving partial remission. In contrast, 61.8% (21/34) of patients underwent radiotherapy after treatment with the R-CHOP regimen. The 5-year PFS and OS rates were higher in the DA-EPOCH-R arm, albeit without significance (Figure 1). There were more treatment-related grade 3/4 hematologic adverse events in patients treated with DA-EPOCH-R. All non-hematologic adverse events were grade 1/2 and tolerable in both treatment groups (Table 3).
Differences of clinical and laboratory parameters in patients with primary mediastinal B-cell lymphoma according to the treatment regimen.
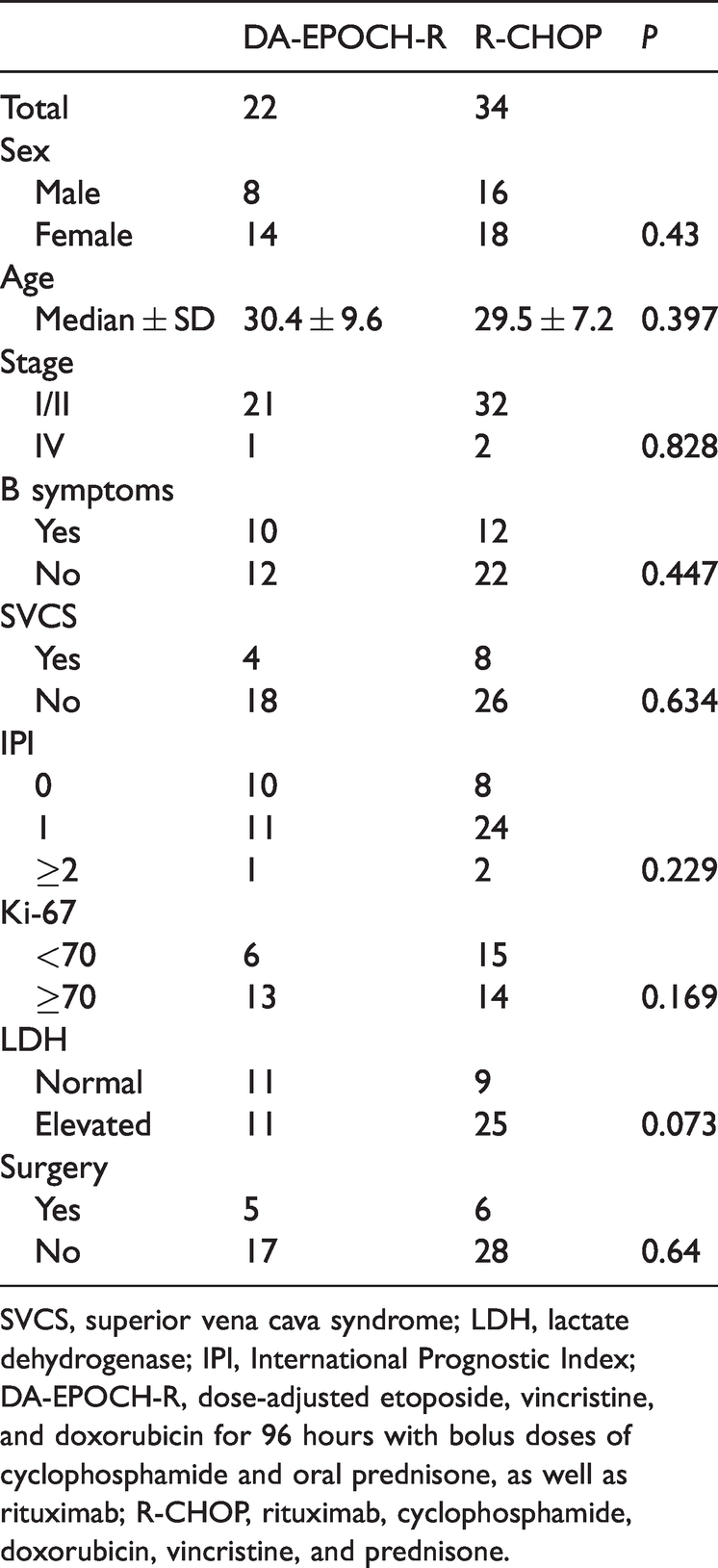
SVCS, superior vena cava syndrome; LDH, lactate dehydrogenase; IPI, International Prognostic Index; DA-EPOCH-R, dose-adjusted etoposide, vincristine, and doxorubicin for 96 hours with bolus doses of cyclophosphamide and oral prednisone, as well as rituximab; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.

Survival of patients with PMBCL treated with different chemotherapy regimens. The PFS and OS of patients with PMBCL treated with DA-EPOCH-R and R-CHOP are presented.
Adverse events of chemotherapy.

DA-EPOCH-R, dose-adjusted etoposide, vincristine, and doxorubicin for 96 hours with bolus doses of cyclophosphamide and oral prednisone, as well as rituximab; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
The impact of patients’ clinical parameters on OS
Kaplan–Meier analysis indicated that late-stage disease, the presence of B symptoms at diagnosis, and higher IPI were associated with worse OS (P < 0.001, P = 0.01, and P < 0.001, respectively; Figure 2a–c). The treatment outcome of first-line chemotherapy was also correlated with OS (P = 0.001; Figure 2d).

Correlations between clinical parameters and OS. Kaplan–Meier analysis illustrating the associations of stage (a), B symptoms (b), IPI (c), and treatment outcome (d) with OS in patients with primary mediastinal B-cell lymphoma. The meanings of lines with different colors are indicated in each panel.
The correlation between patient features and PFS
We found that patients with late-stage disease and higher IPI had shorter PFS (P = 0.016 and P = 0.017, respectively; Figure 3a–b). In our study, 26 patients (9 men and 17 women) underwent baseline 18FDG-PET/CT at our hospital. Among these patients, 11 received DA-EPOCH-R as the first-line treatment, and 17 patients received radiotherapy. Half of the patients achieved complete responses, and the other 13 patients exhibited partial responses. We also analyzed the prognostic value of pretreatment 18FDG-PET/CT functional parameters of the primary lesion, such as maximum and mean standardized uptake values, metabolic tumor volume (MTV), and total lesion glycolysis (TLG). MTV ≥ 500 and TGL ≥ 2500 at baseline were correlated with worse PFS (P = 0.002 and P = 0.023, respectively; Figure 3c–d).

Associations between clinical features and PFS. Kaplan–Meier curves illustrating the associations of stage (a), IPI (b), metabolic tumor volume (MTV), and total lesion glycolysis (TLG) with PFS in patients with primary mediastinal B-cell lymphoma. The meanings of lines with different colors are indicated in each panel.
Discussion
PMBCL is a unique subtype of lymphoma with distinctive clinicopathological features. It is difficult to identify because its symptoms are nonspecific, and it is not easy to radiographically distinguish this disease from other mediastinal diseases, such as thymoma, or other types of lymphoma. In recent years, the rapid development of pathological assessment tools and the wide usage of PET/CT have increased the accuracy of disease diagnosis. The frontline management regimen is of great importance, but no standard treatment has been identified. In our study, 60.7% of patients were treated with R-CHOP with or without consolidation radiotherapy, whereas 39.3% of patients were treated with DA-EPOCH-R. The treatment outcome of the two chemotherapy regimens has remained controversial. Some studies revealed that DA-EPOCH-R was superior to R-CHOP,16,17 whereas others observed no significant difference in outcomes, although increased toxicity was noted in the DA-EPOCH-R group. 18 The results of our study were consistent with the latter findings because the overall response, 5-year PFS, and 5-year OS rates were similar between the groups. However, patients treated with DA-EPOCH-R having a shorter median duration of follow-up should be considered.
Because of the rarity of PMBCL and the heterogeneity of treatment modalities in different countries or regions, there have been few investigations in PMBCL with large sample sizes, resulting in no unified standard of care. The treatment regimen largely depends on the region and choice of the investigators. Although evidence preferentially supports the use of DA-EPOCH-R because of its superior tumor control and ability to obviate the need for radiotherapy in most patients, 19 this treatment regimen often leads to higher costs, greater granulocyte-colony stimulating factor usage, longer hospitalization, and a higher number of hematological adverse events. DA-EPOCH-R also often requires a central line, which might be difficult in patients with bulky mediastinal tumors in the first treatment cycle and might increase the risk of venous thrombosis.
Recent research recorded a complete response rate of 62.2% for MCOP-B as the first-line treatment. 20 Dose-dense RCHOP-ICE resulted in 5-year PFS and OS rates of 93% and 98%, respectively. 21 Studies also reported the outcomes of R-CHOP-21 and DA-EPOCH-R-28 in PMBCL and suggested that R-CHOP-21 may be an alternative treatment regimen. 22 However, in our study and in most centers, DA-EPOCH-R-21 is the most commonly used regimen rather than DA-EPOCH-R-28. In addition, studies retrospectively reviewed patients with PMBCL who were treated with R-CHOP alone without radiation or sequential RCHOP-RICE without radiotherapy.21,23 We inclined to believe that treatment decisions should be made considering patients’ medical histories and short-term and long-term toxicities.
Considering prognostic parameters, we found that advanced stage and higher IPI were associated with worse PFS (P = 0.016 and P = 0.017, respectively) and OS (both P < 0.001), which was consistent with another report. 24 However, the use of IPI in the diagnosis of PMBCL is unspecific regarding the median age at the time of diagnosis and the limited area of lesions in the mediastinum. In addition, patients with B symptoms and those who did not achieve complete or partial responses after first-line treatment had worse OS (P = 0.01 and P = 0.001, respectively). 18FDG-PET/CT has been recognized as an important imaging tool for response assessment in PMBCL. The widely adopted Deauville five-point scale and Lugano classification have standardized PET/CT interpretation and improved the management of patients with lymphoma.25–28 However, there is a risk of false positivity when using the Deauville criteria alone to predict prognosis. Studies are needed to identify a more powerful predictor in PET/CT, such as the standardized uptake value, MTV, and TLG. However, Ceriani et al. demonstrated that only TLG had significant association with OS and PFS. 29 In our study, we found that pretreatment MTV and TLG on PET/CT were correlated with PFS. Knowledge of these distinctive prognostic features is critical for clinicians, and more aggressive treatment regimens might be required for patients harboring high risk factors. In addition, a study revealed that elevated metabolic heterogeneity on PET/CT permit the early identification of refractory patients who might benefit from treatment intensification. 12 We did not analyze this factor in the current study.
In recent years, there has been substantial progress in elucidating the biology of PMBCL.30,31 Considering its unique biological features, new options such as brentuximab vedotin, anti-PD1 agents, JAK2 inhibitors, and CAR-T therapy are emerging for the treatment of relapsed or refractory PMBCL.32–35 We cannot deny some limitations of this study, such as the lack of molecular data and the relatively small sample size. The morbidity of PMBCL is low in China, which prevented us from enrolling a large number of patients. Nonetheless, we performed this retrospective investigation to obtain clues for developing new frontline treatment modalities and better therapeutic procedures for investigation in clinical trials.
Footnotes
Acknowledgements
This work was supported by National Science and Technology Major Project (2017ZX09304021) and National Natural Science Foundation of China (82060041).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.