
Abstract
Previously considered a subtype of diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma (PMBCL) is now recognized by the World Health Organization as an independent entity. PMBCL has clinicopathologic features that are separate from systemic DLBCL and harbors some biologic characteristics which overlap with nodular sclerosing classic Hodgkin’s lymphoma (cHL). Similar to cHL, copy number alterations of 9p24.1 are frequently seen in PMBCL, which leads to increased expression of key genes in the region, including programmed death-ligand 1( PD-L1), PD-L2, and JAK2. In addition, PMBCL cells express CD30 in a mostly patchy fashion. In the upfront setting, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab (i.e., DA-EPOCH-R) is the only regimen that has been shown in a prospective setting to result in outstanding outcomes without consolidative radiation to the mediastinum, with a 5-year event-free survival rate of 93% and overall survival rate of 97%. Thus, in recent years, DA-EPOCH-R has been recognized as the preferred frontline regimen. Despite the encouraging results in the frontline setting, the outcomes in the relapsed/refractory setting remain poor. The current approach of salvage chemotherapy followed by autologous stem cell transplantation, as used in patients with DLBCL, does not result in high rates of cure in patients with rrPMBCL. In recent years, the characteristic molecular features identified in PMBCL have provided more treatment opportunities for this patient population. In the relapsed setting, single-agent PD-1 inhibitor pembrolizumab have demonstrated high and durable remission rates. Despite the expression of CD30, the CD30 antibody drug-conjugate brentuximab vedotin (BV) as a single agent has been deemed inactive in this disease. On the contrary, the combinations of BV and PD-1 inhibitor have shown higher response rates than PD-1 inhibitor alone. Moreover, anti-CD19 chimeric antigen receptor T-cell (CAR T-cell) therapy has been positioned as another successful strategy for patients with rrPMBCL. Axicabtagene ciloleucel and lisocabtagene maraleucel are two products used in rrPMBCL.
Keywords
Chemotherapy regimens
Introduction
The 2016 World Health Organization (WHO) classification of lymphoid malignancies identifies primary mediastinal large B-cell lymphoma (PMBCL) as an independent clinical and biologic entity. 1 PMBCL is an aggressive B-cell lymphoma that is thought to arise from thymic (medullary) B-cells. It has clinicopathologic features that are distinct from systemic diffuse large B-cell lymphoma (DLBCL) and shares some clinical and biologic characteristics with nodular sclerosing classic Hodgkin’s lymphoma (cHL). PMBCL comprises 7% of DLBCLs (2.5% of all non-Hodgkin’s lymphomas). It usually affects young women with a median age at diagnosis in their twenties and thirties. 2 Patients usually present with a large mediastinal mass originating in the thymus with a tendency to invade adjacent structures including the pleura, pericardium, and superior vena cava. 3
Morphologically, PMBCL is comprised of large cells with variable nuclear features and variable levels of sclerosis. 4 Less frequently, the tumor cells resemble immunoblasts. Reed–Sternberg (RS)-like cells, if present, comprise a minor fraction of the tumor cells.5,6 In terms of immunophenotype, the tumor cells typically express B-cell-associated markers (CD19, CD20, CD22, and CD79a) and CD45 and are negative for CD5 and CD10. Weak expression of CD30 is often present. 4 The tumor cells also stain for TRAF-1 and nuclear c-REL; these markers are often likely to be positive in RS-like cells. 7 These two markers are rarely present in other forms of DLBCL but are commonly expressed by the RS cells of cHL. In addition to TRAF-1 and c-REL, two other distinguishing markers between PMBCL and DLBCL are CD200 and MAL. These two markers are relatively specific for PMBCL.8,9 With regard to genetic features, there is no pathognomonic cytogenetic change characteristic for PMBCL. Gene expression profiling has shown similarities between PMBCL and cHL, a disorder with which it shares a number of clinical and laboratory features including hyperdiploid karyotypes, often with gains in the JAK2-containing region on chromosome 9p and the genes encoding programmed death-ligand 1 (PD-L1) and PD-L2.10–13
This review will provide an overview of the current treatment options in both the frontline and relapsed/refractory settings in patients with PMBCL.
Treatment strategies in the frontline setting
PMBCL generally has an excellent outcome with a cure rate of 85–90% across all studies.14–18 Due to the lack of randomized studies for this rare histological subtype, the most suitable upfront therapy remains to be defined. Commonly used regimens include R-CHOP, MACOPB/VACOPB, and recently established DA-EPOCH-R. Historically, the inadequacy of chemoimmunotherapy alone with CHOP, R-CHOP, or MACOPB/VACOPB has resulted in routine consolidation with mediastinal radiotherapy. Given that this disease has a predilection to affect young women in their 20s and 30s, mediastinal radiotherapy is associated with increased risk of developing breast cancer 19 and radiation-induced cardiovascular toxicity later in life. 20 Therefore, the focal point of the debate in establishing the optimal frontline regimen is to assess which regimen can potentially mitigate or ideally eliminate the need for consolidative radiation without compromising the outstanding outcomes.
Although great effort has been placed in investigating the aforementioned question, the majority of the studies addressing this question are controversial. Given the rarity of PMBCL, a great majority of the studies investigating this question are retrospective. As such, the decision to proceed with consolidative radiation or not was not standardized across all studies. In fact, historically, consolidative radiation following upfront chemotherapy with R-CHOP or R-M(V)ACOPB was an integral part of the treatment plan and was pursued in all responding patients. On the contrary, the promise of DA-EPOCH-R regimen was to mitigate the need for consolidative radiation and utilize end-of-therapy positron emission tomography/computed tomography (EOT-PET-CT) as a deciding tool in identifying patients who would truly benefit from this treatment modality. Thus, the cross-study comparison of percentage of patients who received radiation in various studies between R-CHOP and DA-EPOCH-R is intrinsically flawed.14,16,21–23 As the majority of patients treated with R-CHOP regimen proceeded with consolidative radiation as part of a pre-planned treatment strategy, whereas the default treatment plan for patients in the DA-EPOCH-R studies was no radiation and the end-of-treatment PET-CT was used to guide the next course of action. The impact of pre-specified treatment plans on the rate of radiation usage was elegantly illustrated by a recent study from the British Columbia Cancer Agency Group. Prior to 2005, patients were recommended to receive R-CHOP followed by radiation (RT era); in contrast, patients treated in 2005 and beyond would only receive radiation if their restaging PET-CT after six cycles of R-CHOP (EOT-PET-CT) was positive, defined as Deauville score 4–5 (PET era). With such a change in a priori treatment plan, the radiation rate dropped from 78% in the RT era to 28% in the PET era, which represented a 64% reduction. It should be emphasized that the 5-year time to treatment progression and overall survival (OS) were similar in both the RT and PET eras. 15
Therefore, it is instructive to look at the results of end-of-therapy PET (EOT-PET) from different frontline regimens shown in Table 1. Acknowledging the intrinsic bias associated with retrospective studies and cross-trial comparison, one could not help but notice that the rates of positive versus negative EOT-PET were remarkably similar across all studies despite different first-line regimens; however, the rates of radiation used were markedly variable in patients treated with R-CHOP versus DA-EPOCH-R. This discrepancy reflects the difference in a priori treatment plans in the two patient populations. For instance, in a prospective study by Martelli et al. 16 of 115 patients who received R-CHOP, R-CHOP-like, or R-M(V)ACOPB regimen for treatment-naïve PMBCL, 89% received consolidative radiation, including 93% of patients who had a negative EOT-PET. In another retrospective study where patients underwent R-CHOP chemotherapy followed by consolidative radiation therapy mostly at treating physician’s discretion, half of patients who achieved PET-negativity at the end of chemoimmunotherapy underwent consolidative radiation. 23 In comparison, the trial by Melani et al. in 93 patients receiving DA-EPOCH-R showed 25 patients (30%) had a positive EOT-PET, defined as Deauville score 4–5. After monitoring with serial PET-CT, only 5 of 25 patients were deemed as having true persistent disease and proceeded with radiation.
Results of end-of-treatment PET-CT after various first-line regimens for PMBCL.
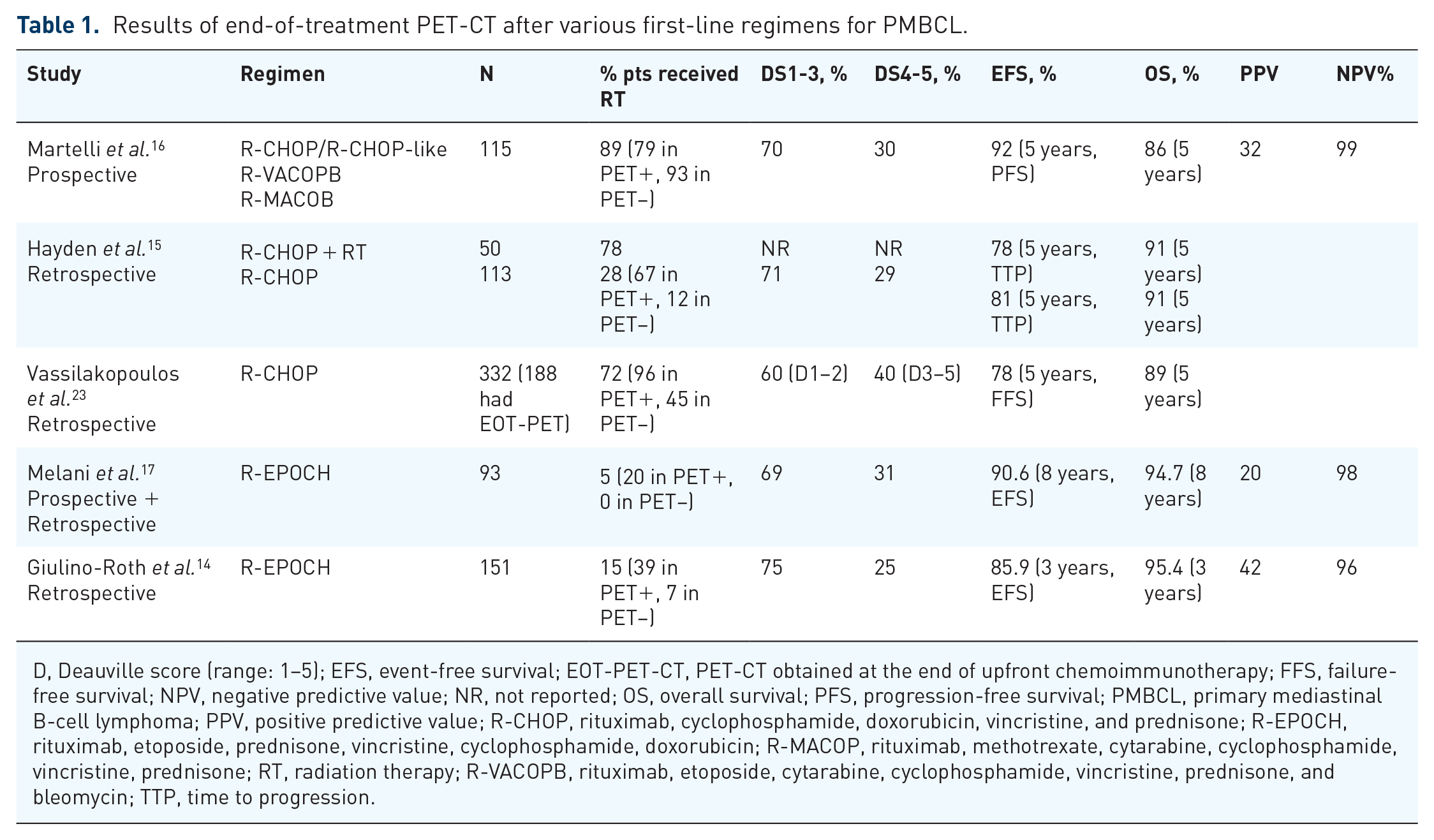
D, Deauville score (range: 1–5); EFS, event-free survival; EOT-PET-CT, PET-CT obtained at the end of upfront chemoimmunotherapy; FFS, failure-free survival; NPV, negative predictive value; NR, not reported; OS, overall survival; PFS, progression-free survival; PMBCL, primary mediastinal B-cell lymphoma; PPV, positive predictive value; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-EPOCH, rituximab, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin; R-MACOP, rituximab, methotrexate, cytarabine, cyclophosphamide, vincristine, prednisone; RT, radiation therapy; R-VACOPB, rituximab, etoposide, cytarabine, cyclophosphamide, vincristine, prednisone, and bleomycin; TTP, time to progression.
Another interesting observation from these major studies is that the rates of positive predictive value (PPV) and negative predictive value (NPV) are strikingly comparable. The PPV of EOT-PET in determining true treatment failure is about 30% (Deauville score 4–5) and the NPV of EOT-PET in determining true complete remission is >95%.14–17,23 In order to remedy the shortcoming of low PPV, the NCI group used serial scans to determine the necessity of radiation in patients with positive EOT-PET after six cycles of DA-EPOCH-R. Based on their results in patients with positive EOT-PET, linear regression analysis of serial scans showed a significant decrease in SUVmax in nonprogressors as compared with progressors. 17 By adding serial scans in 25 patients with a positive EOT-PET, they identified five patients with true treatment failure. As a result, they were able to lower the rate of radiation from 31% (25 of 80 patients with positive EOT-PET-CT) to 5% of the total patient population. Despite a very low rate of consolidative radiation at 5%, the outcomes of the NCI study with DA-EPOCH-R was outstanding. With a median follow-up of 8.4 years, 8-year EFS was 90.6% (95% confidence interval (CI): 81.8–95.2), and 8-year OS was 94.7% (95% CI: 86.3–98.0).17,24 As such, DA-EPOCH-R has become a widely used regimen in treating treatment-naïve patients with PMBCL. The NCI results were validated by a real-world experience, a large retrospective multicenter study of 156 pediatric (N = 38) and adult (N = 118) patients with PMBCL who received DA-EPOCH-R between 2005 and 2015. In this series, at a median follow-up of 23 months, the 3-year EFS was 86% and OS was 95%. Seventy-five percent of this cohort had a negative PET-CT at the end of treatment and 15% of all patients, 39% of EOT-PET-positive patients (14.9% of the entire cohort), proceeded with consolidative radiation therapy. 14
Based on the above discussion, there is universal consensus that particularly in patients with PMBCL and high-risk features, there is a need for more intense chemoimmunotherapy options. A retrospective analysis of a 10-year experience from Lysa Centers, indicated favorable outcomes in patients with PMBCL treated with R-CHOP14 (n = 76) versus patients who were treated with R-CHOP21 (n = 57), with a 5-year progression-free survival (PFS) 89% versus 75%; p = 0.018. 25 There has been no randomized controlled trial to date to establish the superiority of DA-EPOCH-R over R-CHOP or other regimens historically used for this disease. In a large, multicenter cohort analysis of patients with PMBCL, both R-CHOP and DA-EPOCH-R, demonstrated excellent 2-year OS (89% and 91%, respectively). While there were higher complete remission rates with DA-EPOCH-R, patients who received this regimen were more likely to experience short-term treatment-related toxicities but were spared long-term risks associated with mediastinal radiotherapy. 22 In the current era, consideration of early and late toxicities is crucial in determining the appropriate frontline treatment regimen for patients with newly diagnosed PMBCL. In our practice, more intense regimens in the upfront setting are preferred, such as DA-EPOCH-R. Patients with a negative EOT-PET will not receive radiotherapy. Patients with a positive EOT-PET with Deauville score 4–5 (DS4–5) will be followed by serial PET-CT every 6–8 weeks until they exhibit a reassuring downward trend in the SUVmax on subsequent scans. For patients with continued PET-positivity or an increase in SUVmax on subsequent serial scans, we will obtain biopsy whenever feasible, and then refer to radiation oncologists if the residual disease is confirmed. It is imperative to keep in mind that PMBCL is sensitive to radiotherapy if truly indicated. Previous studies have shown that salvage radiotherapy alone is curative in patients with localized residual disease.17,24,26,27 This is uniquely and importantly different from DLBCL. It is also crucial to acknowledge that DS4–5 is a challenging and heterogenous category. Emerging data indicated that DS5 at the end of induction therapy is associated with an inferior outcome. For instance, in a recent study, 49 patients (27% of the entire cohort) were found to have DS 4–5 after the R-CHOP induction therapy, 90% of whom (44 of 49) underwent radiotherapy. The authors reported a 5-year freedom from progression of 92% versus 44% for patients with DS4 and DS5, respectively. 28 Similarly, the British Columbia group reported 5-year time to progression of 57% in the DS5 group after R-CHOP induction. 15 These results corroborate the need for novel approaches in patients with DS5 on EOT-PET.
An emerging effort in patients with PMBCL is to define that risk factors associated with central nervous system (CNS) relapse, which in this otherwise highly curable disease, are associated with dismal outcomes. Kidney/adrenal involvement in PMBCL was reported in 2% and 6% patients, respectively, in two large studies.15,16 although the CNS-IPI prognostic scoring system that is used in patients with DLBCL has not been validated in PMBCL. 29 The rate of CNS relapse in DLBCL has been examined in several studies that included several thousands of patients and is established at approximately 4%; however, the rate of CNS relapsed in PMBCL is not well studied.29,30 In a retrospective series to describe the incidence of CNS relapse among 100 patients with PMBCL who were treated with R-CHOP with or without radiation therapy was compared with 45 patients treated with CHOP with or without radiation therapy. In each cohort, two patients developed CNS relapse: 2% (2/100) R-CHOP ± RT group versus 4.4% (2/45) patients in CHOP ± RT cohort. All patients had isolated CNS relapse. The risk factors were thought to be poor performance status and higher age-adjusted IPI. 31 Other studies have reported a similar CNS relapse rate of 1.6–2.5%.15,32 In our practice, CNS prophylaxis is not routinely used. In very selected cases with high-risk features, such as advanced stage and muliple extranodal sites, we would consider our general practice guidelines for CNS prophylaxis.
Treatment strategies in the relapsed/refractory setting
Despite significant progress in the upfront setting, the outcomes in patients with primary refractory or relapsed PMBCL (rrPMBCL) remain subpar. Like other aggressive B-cell lymphomas, salvage therapy followed by consolidation with high-dose therapy and autologous stem cell transplantation remains the current standard of care.33–35 This treatment strategy has been mostly inspired by treatments used for DLBCL. Given distinct pathologic and genetic features of PMBCL, checkpoint inhibitors and CD30 antibody drug conjugate, brentuximab vedotin (BV), have had promising activity in patients with rrPMBCL. In this section, we will review the landmark trials that have situated these agents in the treatment realm of rrPMBCL.
BV
BV is a potent anti-CD30 antibody drug conjugate that has been approved as single agent in relapsed/refractory cHL after ASCT 36 and anaplastic large-cell lymphoma (ALCL). 37 The CD30 antigen is present in the majority of cases of PMBCL (80%) with heterogenous expression. 38 Therefore, the Italian Lymphoma Foundation performed a single-arm, multicenter, phase-II trial evaluating the efficacy and tolerability of BV as a single agent in patients with relapsed/refractory histologically confirmed CD30+ PMBCL. BV was administered intravenously at 1.8 mg/kg every 3 weeks. Patients who achieved stable disease or better as assessed by the investigator were supposed to receive at least 8, but not more than 16 cycles of study treatment. The primary endpoint was objective response rate (ORR). A total of 15 patients were included in the trial, 53% of which had advanced stage disease, and 74% were refractory to the most recent treatment. Two of 15 patients achieved partial response (PR), yielding an ORR of 13.3%, and the duration of these responses was less than 3–4 months. Originally, 20 patients were planned for the study, but the study group terminated the trial early due to the lack of efficacy. 39 A similar low-response rate was observed in another phase-II study of relapsed/refractory DLBCL treated with BV. In this study, there were six patients with PMBCL, only one patient responded with a complete remission (CR), yielding an ORR of 17%. 40 Given the distinct histologic subtype of PMBCL, being typically characterized by high CD30 expression, these subpar results were unexpected.
Immune checkpoint inhibitors
Copy number alterations (CNAs) of 9p24.1, including chromosomal amplification, gain, polysomy, or translocation, are one of the trademarks of cHL.41,42 CNA of 9p24.1 is also frequently observed in extranodal large B-cell lymphomas, such as PMBCL, primary central nervous system lymphoma (PCNSL), and primary testicular lymphoma (PTL).13,43–45 These genomic alterations can lead to increased expression of key genes in the region, including PD-L1, PD-L2, and JAK2.41,42 PD-L1 and PD-L2 signal through the programmed cell death-protein 1 (PD-1) receptor on T-cells and function as an immune checkpoint to negatively regulate T-cell-mediated immunity. 46 As such, amplification of 9p24.1 in PMBCL provides an opportunity for examining the efficacy of immune checkpoint inhibitors targeting PD-1 such as nivolumab or pembrolizumab. These immune checkpoint inhibitors have shown to be efficacious in treating relapsed and/or refractory cHL.47–50
KEYNOTE-13 trial is a phase-Ib trial which examined the safety, tolerability, and efficacy of pembrolizumab, an anti-PD-1 antibody, in a wide range of hematologic malignancies in multiple cohorts. In the cohort assigned to patients with rrPMBCL, 21 participants were included with a median age of 30 years and median 3 prior lines of therapy. Primary endpoint was ORR and safety. At a median follow-up of 29.1 months, the ORR was 48%, with a CR rate of 33%, and the median duration of response (mDOR) was not reached. 51 These promising results in heavily pretreated patients with rrPMBCL set the stage for the pivotal phase-2 trial, the KEYNOTE-170 study.
Phase-2 KEYNOTE-170 study is a larger effort evaluating safety and efficacy of pembrolizumab in two cohorts: patients with rrPMBCL and patients with Richter’s syndrome. Patients received intravenous pembrolizumab 200 mg on an every-3-week basis until disease progression, intolerance, or completion of 2 years of therapy. Primary endpoint was ORR. The rrPMBCL cohort enrolled 53 patients with a median age of 32 years, and median 3 prior lines of therapy. Of the 33 participants, 24% had received prior radiation, and 70% were not eligible for ASCT due to chemo-refractory disease. At a median follow-up of 12.5 months, the ORR was 45%, with a CR of 13%, and the mDOR was not reached. 52 Based on this trial, on June 13, 2018, the Food and Drug Administration (FDA) granted accelerated approval to pembrolizumab for the treatment of adult and pediatric patients with rrPMBCL who have received two or more prior lines of therapy.
The other noteworthy trial is the phase-II Checkmate-436 study combining nivolumab and BV every 3 weeks until disease progression or unacceptable toxicity in rrPMBCL. Primary endpoint was ORR. Thirty patients were treated and evaluable. At a median follow-up of 11.1 months, ORR was 73% with a metabolic CR rate of 43%. Median DOR, median PFS, and median OS were not reached. Eleven responders proceeded to consolidation with autologous (n = 5) or allogeneic (n = 6) transplantation. Sixteen patients (53%) had grade 3–4 treatment-related adverse events. There were no treatment-related deaths. 53 It should be noted that even though there appeared to be more immune-mediated adverse events with the combination regimen, grade 3–4 adverse events were still infrequent (Table 2). In addition, in the KENOTE–013, –170, Checkmate–436 trials, there were 11, 7, and 7 complete responders, respectively. None of these patients relapsed, including two patients who were off treatment for more than a year. Taken together, the high ORR and DOR achieved on these trials has established PD-1 blockade as a promising treatment strategy for this patient population. A summary of the pivotal trials including checkpoint inhibitors is provided in Table 2.
Summary of trials including checkpoint inhibitors in patients with relapsed/refractory PMBCL.

BV, brentuximab vedotin; CI, confidence interval; CR, complete response; DOR, duration of response; NE, not estimable; NR, not reported; ORR, overall response rate; PMBCL, primary mediastinal B-cell lymphoma; PR, partial response; SD, stable disease.
Chimeric antigen receptor T-cell therapy
Chimeric antigen receptor T-cell (CAR T-cell) therapy has dramatically changed the treatment landscape of B-cell lymphomas, including PMBCL. To date, three CD19-targeted CAR T-products have been approved by the FDA for relapsed/refractory DLBCL. The CAR T-cell therapy constitutes a monumental achievement, as it provides a curative approach for highly chemo-refractory patients, as in many patients with PMBCL in the relapsed setting. The results and important toxicities of the three pivotal trials led to the FDA approval are presented in Table 3.
Summary of the efficacy and safety of three CAR T registration trials.

Axi-cel, axecabtagene ciloleucel; CAR T-cell, Chimeric antigen receptor T-cell; CR, complete remission; CRS, cytokine release syndrome; DLBCL, diffuse large B-cell lymphoma; ICANS, Immune-effector cell associated neurotoxicity syndrome; liso-cel, lisocabtagene autoleucel; PFS, progression-free survival; PMBCL, primary mediastinal B-cell lymphoma; tFL, transformed follicular lymphoma.
Patients with PMBCL were included in 2 of the 3 pivotal CAR T-cell trials, the ZUMA-1 (axicabtagene ciloleucel) and TRANSCEND-NHL-001 trials (lisocabtagene maraleucel), which included 8 and 14 patients with rrPMBCL, respectively. The JULIET trial (tisagenlecleucel) did not include patients with rrPMBCL. All these trials had the same treatment paradigm: peripheral blood mononuclear cell apheresis followed by bridging chemotherapy/radiation therapy at physician’s discretion. Once the CAR T-product was manufactured and received by the treating institution, patients underwent lymphodepleting chemotherapy followed by CAR T-cell infusion. Responders with PMBCL were seen in both ZUMA-1 and TRANSCEND-001 trials, and some exhibited durable responses. In the TRANSCEND-NHL-001 trial, the ORR for 14 patients with rrPMBCL was 79% with seven patients (50%) achieving complete remission. 54 The NCI group, who conducted the very first CAR T-cell therapy in America, recently reported long-term outcomes of 46 patients treated with axicabtagene ciloleucel between 2009 and 2015.55,56 Among 28 patients with DLBCL/PMBCL, 48% had duration of response (DOR) greater than 3 years. Six of 28 patients had PMBCL, with 5 evaluable for response. Among evaluable patients, two achieved CR, two stable disease (SD), one progressive disease (PD), yielding an ORR of 40%. The two patients who achieved CR had DOR of 97+ and 38+ months, respectively. 56
Conclusion
PMBCL is a distinct clinicopathologic entity that is highly curable and predominantly affects adolescents and young adults, with a predilection for young women. In the upfront setting, the goal is to adopt highly curative approaches that could eliminate the need for mediastinal radiation. Using EOT-PET to determine the necessity of radiation led to a dramatic reduction in radiation rate without compromising the outstanding outcomes in this disease. Surprisingly, the rates of positive EOT-PET appeared to be similar for all three commonly used first-line regimens, R-CHOP, RM(V)COPB as well as DA-EPOCH-R. The PPV of a positive EOT-PET is low at 30% for all three regimens. To further reduce the need for mediastinal radiation, the NCI group used serial PET scans in patients with a positive EOT-PET to identify true treatment failures. By doing so, they successfully reduced the radiation rate to 5%, without compromising the outstanding cure rate achieved by DA-EPOCH. It is not known whether similar strategy will be successful in patients treated with R-CHOP. Thus, our current preferred regimen for first-line therapy in patients with PMBCL is DA-REPOECH. Patients with a positive EOT-PET will be monitored by serial PET scans until resolution of fluorodeoxyglucose (FDG)-avidity or establishment of clear evidence of progressive/residual disease.
Despite the encouraging results associated with DA-EPOCH-R in the upfront settings, outcomes for patients with rrPMBCL remain suboptimal, mainly due to the chemo-refractory nature of the disease in the relapse/refractory setting. Radiotherapy is uniquely active in this disease and can be curative for localized recurrences in some cases. Non-chemotherapy-based strategies using checkpoint inhibitors has yielded promising results, although the CR rates remain low. Finally, the recent approval of axi-cel 57 and lisocabtagene maraleucel 54 has further expanded the armamentarium of treatment options for patients with rrPMBCL. These recent advances have truly brightened the horizon for patients with rrPMBCL. To further advance the field, the future trials should focus on the optimal sequencing of the available agents in the relapsed/refractory setting, and examine the potential benefit of considering CAR T-cell therapy as an earlier line of therapy in patients with rrPMBCL.
Footnotes
Author contributions
BF conducted literature review, designed the stucture, wrote the paper and reviewed the paper.
WA conducted literature review, reviewed the paper and supervised the work.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.