
Abstract
Improved understanding of the mechanisms of lymphomagenesis has resulted in a surge of development for new targeted agents. An impressive number of biological agents targeting different steps in the pathways of tumor proliferation, survival and apoptosis have become available. The management of patients with indolent non-Hodgkin lymphomas (iNHLs) is rapidly transforming with incorporation of those targeted biological agents into the front-line and relapsed/refractory setting. This review highlights several categories of novel biological agents and will discuss their potential role in the contemporary management of patients with iNHLs.
Introduction
Non-Hodgkin lymphomas (NHLs) represent about 4% of all malignancies, with an estimated incidence in the US of 72,240 in 2017. 1 The indolent NHLs (iNHLs) comprise a heterogeneous group of low-grade lymphomas which classically include follicular lymphoma (FL), marginal zone lymphoma (MZL), a subset of mantle cell lymphomas (MCLs), and chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). The iNHLs tend to have a low proliferative rate and grow slowly; their historical management simplistically can be divided in expectant observation for asymptomatic disease, and treatment for symptomatic or bulky disease. Retreatment is frequently required for relapse as iNHLs are considered an incurable malignancy by standard approaches. However, timing and best choice for initial treatment can be controversial. The optimal timing of first treatment is not entirely clear as most data comparing upfront chemotherapy versus watchful waiting predate the era of rituximab.2–4 With improved ways to prognosticate5–8 and the development of novel agents, treatment paradigms for iNHLs are being redefined.
Biological advancements have helped to better define mechanisms of lymphomagenesis which in turn informed specific treatment targets in iNHLs. Routed in the lack of predictive biomarkers, national therapeutic guidelines apply standardized regimens to nonstandardized individuals. 9 Although many patients with iNHLs can enjoy prolonged survival, a subgroup of patients with high-risk features, such as primary refractory or early relapsed disease, have an uncharacteristically poor prognosis with current standard therapy. 10 Ideally, improved understanding of the defining molecular drivers and processes leading to treatment resistance in iNHLs will permit prescription of better targeted therapies that can switch off the underlying lymphoma drivers or overcome resistance mechanisms while limiting off-target adverse effects (AEs).
In this paper, we aim to outline the development and incorporation of novel targeted therapy in the treatment of indolent B-cell lymphomas with a focus on currently or ‘soon-to-become’ available agents. Contemporary mechanisms of biologic therapies to be discussed include those directed towards cell surface antigens, tumor microenvironment, as well as intracellular pathways, such as phosphoinositide 3-kinase (Pi3K)/Akt/mammalian target of rapamycin (mTOR), the B-cell receptor (BCR) pathways, and the nuclear factor (NF)-kB and Bcl-2 pathways of survival and apoptosis, which are summarized in Table 1. The treatment of CLL/SLL has evolved substantially from the remainder of the iNHLs and thereby exceeds the scope of our review. We suggest to refer to other published exhaustive reviews. 11
Selected studies of targeted agents in indolent NHL.
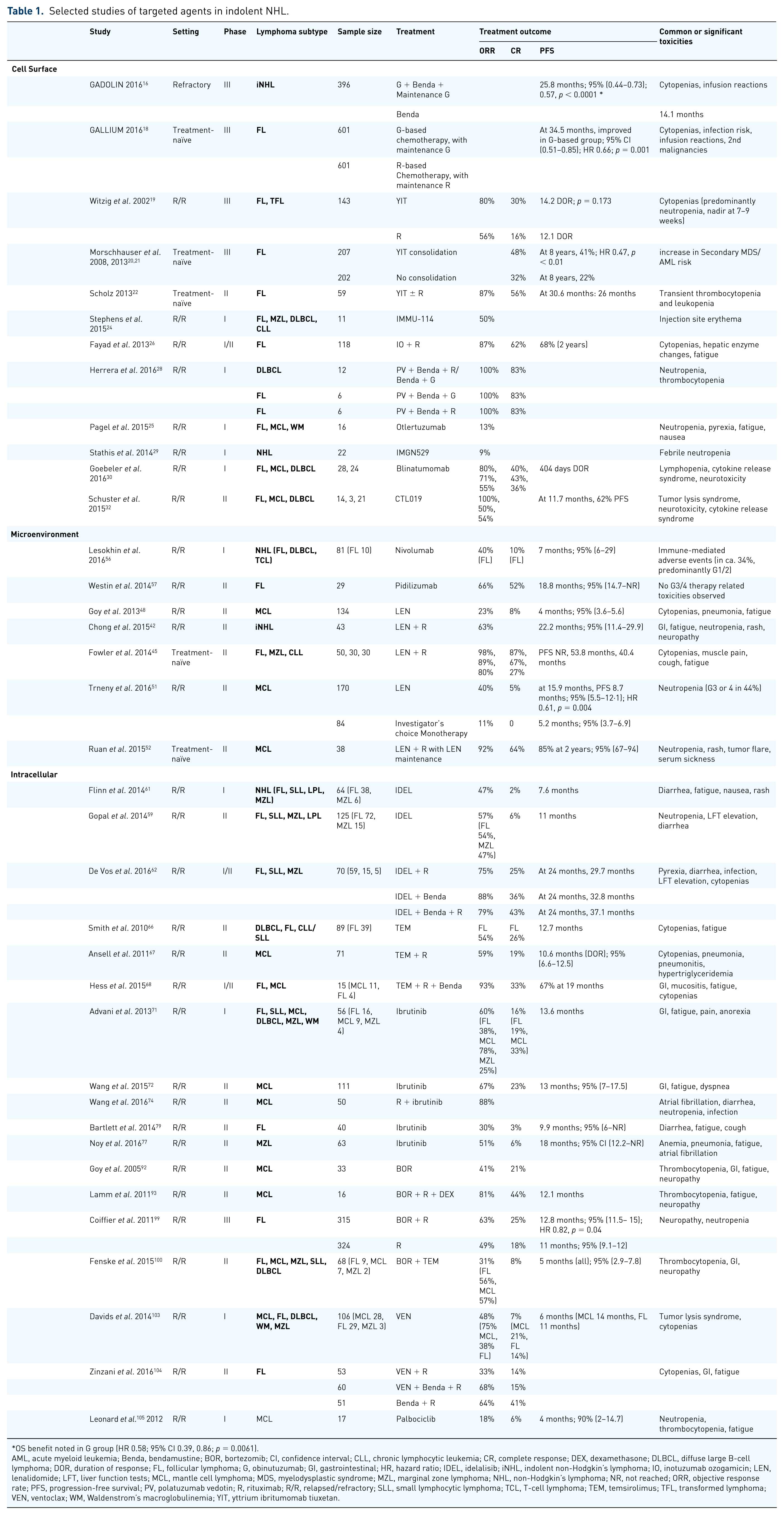
OS benefit noted in G group (HR 0.58; 95% CI 0.39, 0.86; p = 0.0061).
AML, acute myeloid leukemia; Benda, bendamustine; BOR, bortezomib; CI, confidence interval; CLL, chronic lymphocytic leukemia; CR, complete response; DEX, dexamethasone; DLBCL, diffuse large B-cell lymphoma; DOR, duration of response; FL, follicular lymphoma; G, obinutuzumab; GI, gastrointestinal; HR, hazard ratio; IDEL, idelalisib; iNHL, indolent non-Hodgkin’s lymphoma; IO, inotuzumab ozogamicin; LEN, lenalidomide; LFT, liver function tests; MCL, mantle cell lymphoma; MDS, myelodysplastic syndrome; MZL, marginal zone lymphoma; NHL, non-Hodgkin’s lymphoma; NR, not reached; ORR, objective response rate; PFS, progression-free survival; PV, polatuzumab vedotin; R, rituximab; R/R, relapsed/refractory; SLL, small lymphocytic lymphoma; TCL, T-cell lymphoma; TEM, temsirolimus; TFL, transformed lymphoma; VEN, ventoclax; WM, Waldenstrom’s macroglobulinemia; YIT, yttrium ibritumomab tiuxetan.
Targeting the cell surface
The tumor cell surface contains many unique antigens, which can be overexpressed, mutated or selectively expressed compared with normal tissues. Through targeting with monoclonal antibodies (mAbs), cell killing can be achieved via direct blockade or agonist activity at the receptor level, immune-mediated cell killing mechanisms, and indirect effects of antibody on tumor vasculature or stroma 12 (see Figure 1).
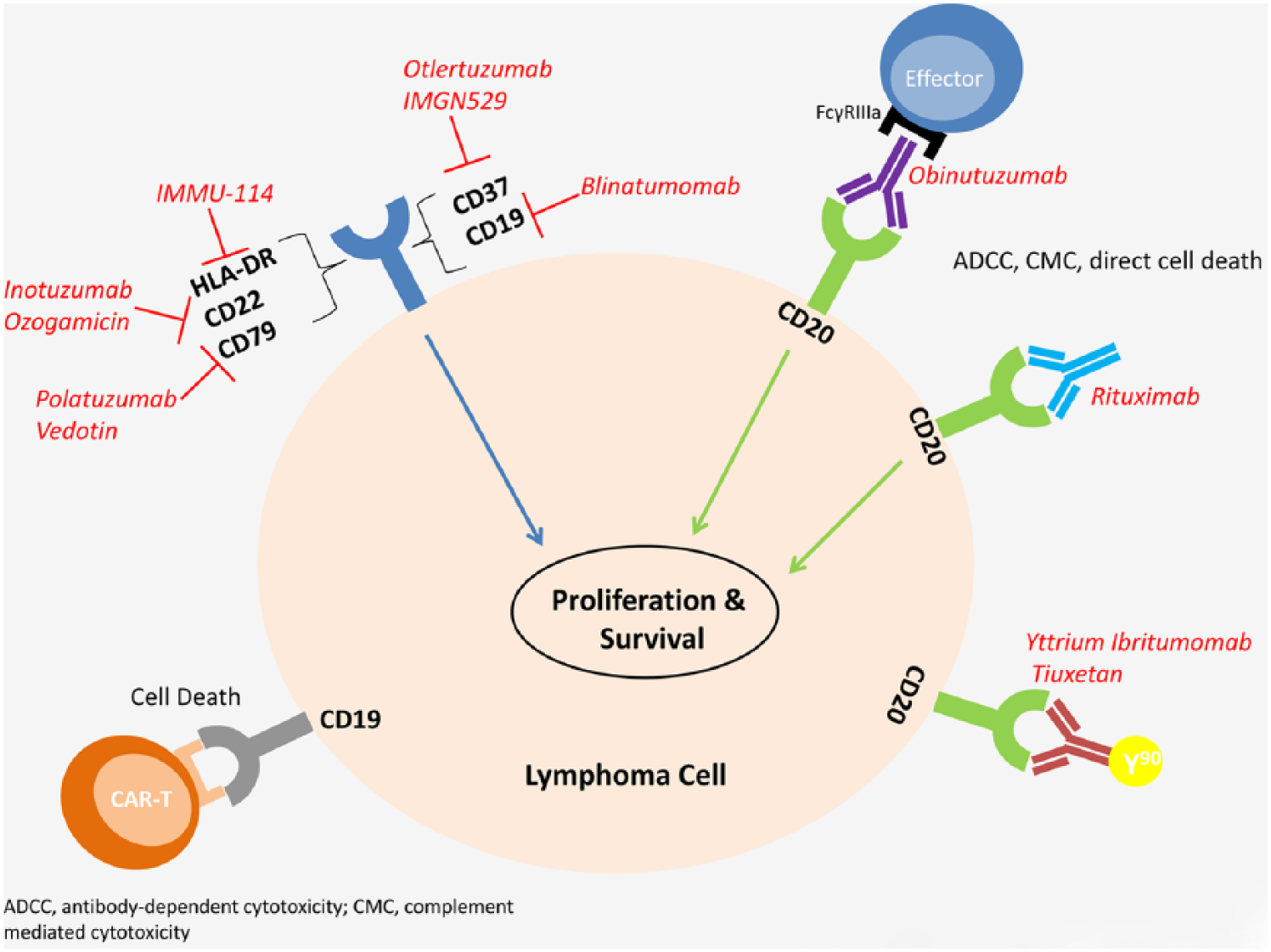
Cell surface targets.
CD20 is a B-cell antigen expressed during differentiation from the pro-B-cell phase until the plasma cell phase and is present on almost all normal and malignant B-cells. 13 Rituximab (R) is a chimeric mAb directed against CD20, believed to deplete B-cells through multiple mechanisms including antibody dependent cellular cytotoxicity, complement dependent cytotoxicity, and direct effects on cell signaling pathways involved in proliferation, survival and apoptosis. 14 Since its initial United States Food and Drug Administration (US FDA) approval in 1997, R has revolutionized B-cell lymphoma treatment and become the prototypical anticancer-targeted antibody. Subsequently, other potentially more potent anti-CD20 mAbs were developed, such as obinutuzumab (G), a type II, humanized anti-CD20 mAb with enhanced affinity for FcγRIIIa receptors on effector cells and enhanced direct killing. 15 Its US FDA approval in 2016 for FL was based on findings of the GADOLIN trial in rituximab refractory iNHL showing superior median progression-free survival (PFS) and overall survival (OS) in the combination group of G + bendamustine (B) with maintenance G versus B alone (PFS 25.8 months versus 14.1 months; OS not reached versus 53.9 months). 16 Obinutuzumab was evaluated in first-line treatment of FL in the GALLIUM study which compared G-based chemotherapy with R-based chemotherapy in combination with maintenance. 17 At a median follow up of 34.5 months, improved PFS was noted in the G treatment arm [hazard ratio (HR) 0.66, p = 0.001] with a 3-year PFS of 73.3% versus 80.0%, along with higher incidence of cytopenia, infection and infusion reactions. No OS benefit was found. Rituximab and obinutuzumab are now staples in the upfront and subsequent lines of therapy for all CD20-positive lymphomas.
Yttrium-90 ibritumomab tiuxetan (YIT; Zevalin®) is an anti-CD20 mAb linked via a chelator to the radioisotope yttrium-90 which is currently approved in relapsed/refractory (R/R) NHL as well as in consolidation after first-line chemotherapy for FL. A randomized trial of YIT versus rituximab in R/R FL or transformed lymphoma (tFL) demonstrated an improved objective response rate (ORR) (80% versus 56%) and complete response (CR) rate (30% versus 16%) albeit with similar duration of response (DOR) at 14.2 months versus 12.1 months (p = 0.6). 18 YIT was then studied as consolidation of remission after first-line therapy in advanced FL and showed prolonged PFS (HR 0.465, p < 0.0001) with conversion of partial response (PR) into CR in 77% of patients. 19 The 8-year follow-up data continue to show a 3 year benefit in median PFS (19% PFS advantage) however with a statistical increase in myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML) annualized incidence (0.5% versus 0.07%, p = 0.042). 20 Subsequent phase II data evaluating YIT in first-line treatment of FL showed a significant ORR (87%) and PFS with potential for deep lasting responses in those who achieve CR. 21 While YIT is reasonably well tolerated, it poses concern for prolonged myelosuppression; bilateral bone marrow aspirate and biopsy is recommended to rule out significant (>25%) lymphoma involvement prior to administration. YIT’s contemporary role is not clear, but may be considered in elderly and frail patients not otherwise candidates for intensive therapy. Similarly, iodine-131 tositumomab (Bexxar®) is an anti-CD20 radioimmunotherapy agent that was US FDA-approved for R/R iNHLs refractory to R; however, it was discontinued by its manufacturer in 2014. 22
Anti-HLA-DR antibodies are an intriguing new target as they are expressed on lymphoma cells at higher levels than typical B-cell markers. A phase 1 dose finding study of IMMU-114 showed clinical activity in FL, MZL, diffuse large B-cell lymphoma (DLBCL) and CLL with 50% (n = 4 of 8) assessable patients achieving an objective clinical response. Because of concerns for significant infusion-related toxicities, IMMU-114 is administered subcutaneously. 23
CD37 is a cell surface tetraspanin present on normal and malignant B-cells. It has been evaluated in a phase I trial as a target with humanized anti-CD37 protein otlertuzumab (TRU-016) in R/R FL, MCL and Waldenstrom’s macroglobulinemia (WM). A total of 16 patients were treated with two objectives responses and 11 patients with stable disease. Toxicities included neutropenia, pyrexia, fatigue and nausea. 24 Further studies are ongoing to define the role of these apparently active surface antibodies in iNHLs.
To potentiate the effects of mAbs, investigators have coupled antibodies directed at the lymphoma cell surface with cell toxins, thereby creating immunoconjugates (ICs). Inotuzumab ozogamicin (IO) is an IC whereby an immunoglobulin (Ig)G4 anti-CD22 antibody is linked to cytotoxic calicheamicin. In R/R FL, IO in combination with rituximab has demonstrated an ORR of 87% (CR 62%) and 2-year PFS of 68%. 25 Common AEs were hematologic and altered liver function. Polatuzumab vedotin, which links CD79b to monomethyl anti-tubulin auristatin E 26 was evaluated in a phase I trial of R/R FL. ORR was 75–76% with CR 10–44%: a trend towards better tolerability was noted at the lower dose and through shorter treatment (8 cycles) in combination with bendamustine and R or G. Of 12 FL patients enrolled, 67% (8/12) had grade ⩾3 AEs including neutropenia and thrombocytopenia; however, the ORR was 100%. DOR has not yet been reported. 27 IMGN529, a CD37 target conjugated to maytansinoid anti-mitotic DM1, was evaluated in a phase I study of 33 R/R NHLs and demonstrated encouraging anti-lymphoma effects. 28 These IC agents are promising and being evaluated in larger trials as single agents as well as in combinations.
Cell surface markers can also be exploited by identifying lymphoma cells to the immune system. The bispecific antibodies (Bispecific T-cell Engager, or BiTE) incorporate a tumor antigen such as CD19 and a CD3 T-cell surface glycoprotein, and thereby bring together tumor cells and T-cells, triggering T-cell activation and cytotoxicity with cytokine production only when both binding sites are occupied. Blinatumomab is the first in class drug and has been approved as second-line treatment of acute lymphoblastic leukemia. It was shown in a phase I study to have anti-lymphoma activity at very low doses, however with significant neurologic and cytokine-related AEs. Of 76 total patients, 28 patients with FL had an ORR of 80% and 24 patients with MCL had an ORR of 71%. 29 Administration requires a continuous infusion for up to 8 weeks per cycle. Currently, blinatumomab’s side effect profile and cost make it prohibitive for off-label use despite its potential in iNHLs. Newer less toxic and less cumbersomely administered BiTE agents however may offer an effective immunotherapy for high-risk R/R patients.
Adoptive immunotherapy using chimeric antigen receptor T-cell therapies (CAR-T) harnesses the concept of redirecting T-lymphocytes towards specific cell surface cancer antigens via engineering chimeric antigen receptors. Limited responses were seen until a co-stimulatory signal was added with CD28. 30 Further study suggested benefit for conditioning regimens that lead to lymphodepletion, such as fludarabine or cyclophosphamide, by improving CAR-T-cell expansion and persistence in the host.31,32 The largest experience to date has been in treatment of ALL 33 and NHL31,34–36 using CD19-targeted CAR-T. These trials highlighted encouraging response rates in otherwise refractory patients and the potential for durable remissions. Results of the CTL019 trial for R/R DLBCL, MCL and FL were presented in 2015. 31 After apheresis of peripheral blood leukocytes, patients received lymphodepleting chemotherapy followed by infusion of CTL019 cells 1–4 days later. Of the 38 patients enrolled, 14 had FL and 3 had MCL. ORR at 3 months was 100% for FL (7/7) and 50% for MCL (1/2 reported) with 100% PFS in FL at 11.7 months follow up. 31 Another CD19-directed CAR-T, KTE-C19, has recently reported promising results in aggressive lymphomas including DLBCL, tFL and primary mediastinal lymphoma.34–36 Based on the promising results, US FDA approval is anticipated for 2017. Safety concerns continue to loom for CAR-T, as cytokine release syndrome and neurotoxicity 37 have prompted discontinuation of several other investigational programs. Within the current realm of iNHLs, CAR-T will likely soon have an important role in the treatment of fit patients with refractory disease where otherwise hematopoietic stem cell transplant may be considered. However, concerns exist with regard to the unique AE profile, logistical obstacles towards manufacturing, and longevity of response. Newer generation CAR-T-cell therapies might be able to overcome these obstacles.
Targeting the microenvironment
The cellular context in which lymphoma arises and persists has been increasingly studied. The tumor microenvironment of B-cell lymphomas, consisting of immune and stromal cells, blood vessels, and extracellular matrix, enables cancer pathogenesis and progression as well as immune evasion 38 (see Figure 2).
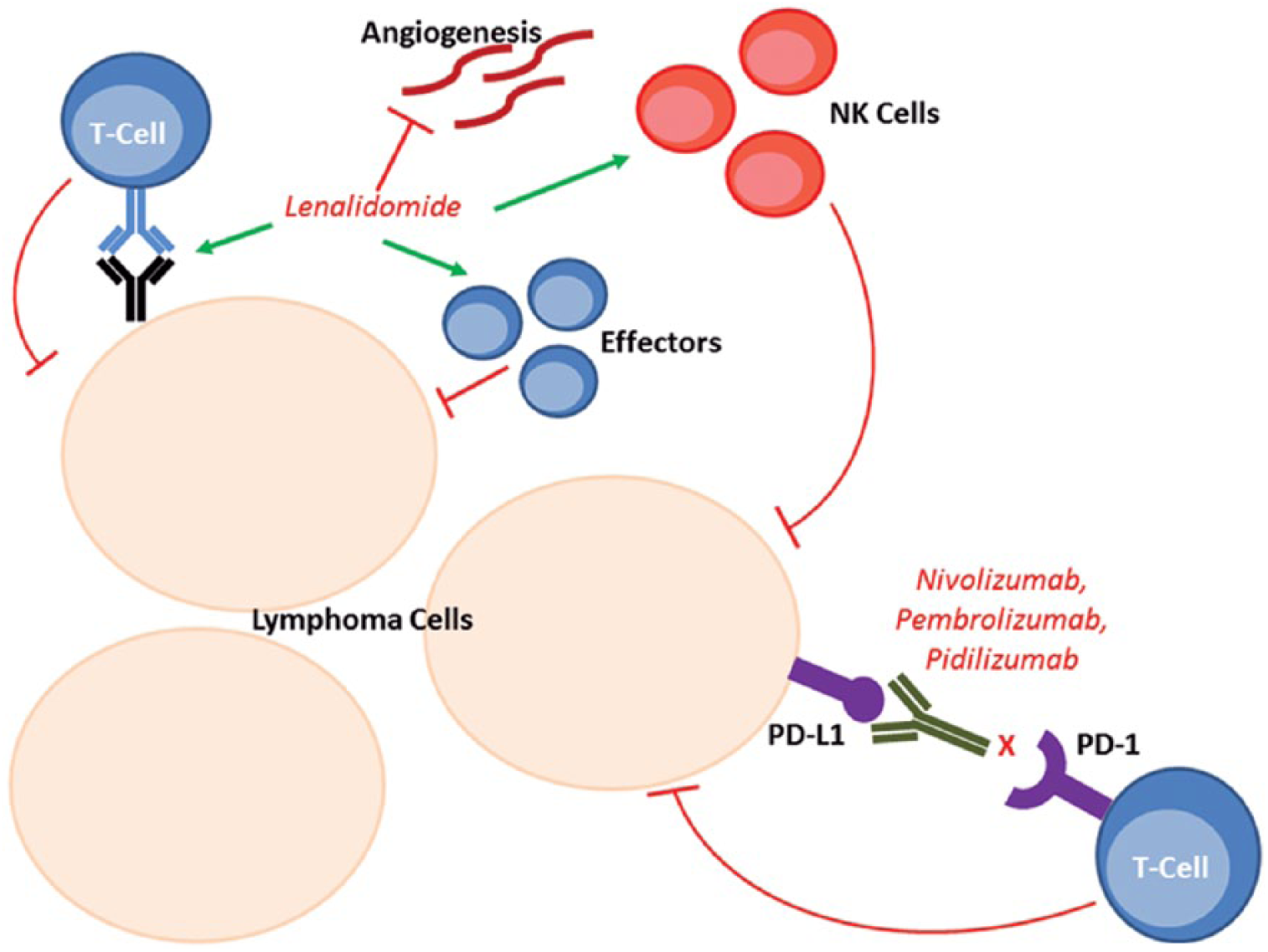
Microenvironment.
Immunomodulatory drugs (Imids) act via immune modulation through T-cell immune synapse enhancement, natural killer (NK)/T-cell effector augmentation, and anti-proliferative effects. 39 Established as a staple in the therapy of plasma cell neoplasms, their role in treatment of iNHLs is still evolving. Lenalidomide (LEN) is a second-generation Imid with anti-proliferative and anti-angiogenic properties, which has been evaluated in iNHL lymphoma and is US FDA-approved for the treatment of MCL. An early phase II trial in R/R iNHLs demonstrated durable responses with ORR of 23%, 40 prompting further study. LEN was combined with R showing an improved ORR (ranging between 63 and 77%) and PFS of 12.4–22.2 months.41–43 Having established its activity in the R/R setting, Fowler and colleagues 44 evaluated the combination in untreated iNHLs (FL = 50, MZL = 30, SLL = 30) reporting an ORR of 98% (63% CR), prompting an ongoing phase III trial in untreated FL [ClinicalTrials.gov identifier: NCT01938001].
In MCL, LEN showed particularly promising activity.13,45–49 MCL-001 47 was a single arm trial of LEN in bortezomib pretreated patients reporting an ORR of 28% (7.5% CR) and PFS of 4 months. This led to the randomized phase II MCL-002 50 in which LEN demonstrated superior PFS when compared with investigator’s choice monotherapy [8.7 versus 5.2 months, HR 0.61, confidence interval (CI) 0.44–0.84; p = 0.004]. In the upfront setting R + LEN followed by LEN maintenance in patients who were not candidates for intensive chemotherapy resulted in an ORR of 92% (64%,CR) and 2-year PFS of 85%. 51 The regimen was well tolerated and compared favorably with historical controls treated with traditional induction therapy, thereby highlighting its potential for the initial treatment of MCL. 52 The ongoing Intergroup E1411 trial [ClinicalTrials.gov identifier: NCT01415752] compares R + bendamustine ± bortezomib induction followed by rituximab ± LEN maintenance and results are eagerly awaited.
The current data underpin a significant role for Imids, specifically LEN, in the management of iNHLs in both first and subsequent lines of therapy. LEN appears as a good building block for future biological combination regimens. The best partner(s), however, remain to be defined, particularly in the front-line setting.
The lymphoma tumor microenvironment is also implicated in enabling immune escape. The T-cell programmed death-1 (PD-1) receptor acts to mitigate the T-cell response to antigen stimulus upon contact with its ligands PD-L1 and PD-L2. 53 This interaction results in apoptosis of activated T-cells and is a necessary homeostatic function to maintain T-cell tolerance to self and limit cellular destruction. 54 Malignancies can exploit this pathway via upregulation of PD-L1 which promotes evasion from activated T-cell or recruited NK cells. The checkpoint inhibitors are a class of mAb designed to reverse immune evasion pathways by inhibiting PD-1 activity by blocking ligand binding. Most mature data in hematologic malignancies are available for the PD-1 inhibitors pidilizumab (humanized IgG1), pembrolizumab (humanized IgG4) and nivolumab (human IgG4). Lesokhin and colleagues presented data evaluating nivolumab in R/R NHL. 55 A total of 10 patients with FL were enrolled with 4 responders (40% ORR; 10% CR). No responses were seen in other iNHL subtypes (MCL = 4, SLL = 2, MZL = 1). Immune-related AEs, attributed to enhanced T-cell activity, were noted in 34% of patients despite being mostly grade ⩽2. Another PD1-inhibitor, pidilizumab, was combined with R in a phase II study of 29 patients with R/R FL. 56 ORR was reported at 66% (CR 52%) with a median PFS of 18.8 months. This was superior to historically reported ORR and CR for rituximab alone (40% and 11% respectively) and no ⩾ grade 3 AEs were seen. An ever-expanding number of trials of various agents activating the anti-cancer immune response seek to define the role of immune-oncology in the management of iNHLs. These trials explore monotherapies, combination therapies with chemotherapy or radiation therapy (taking advantage of a possible abscopal effect), as well as ways other agents that also augment the immune response such as other immune checkpoint inhibitors, IDO1 inhibitors, Imids, or vaccine therapy. While not yet ready for prime time, the checkpoint inhibitors have the potential to allow durable anti-lymphoma activity in some patients. The current challenge is to determine how best to augment somewhat limited single agent responses by either identifying reproducible predictive biomarkers or synergistic combination therapies.
Intracellular signaling pathways
B-cell receptor (BCR) signaling and PI3K/Akt/mTOR
The PI3K/Akt pathway is a key regulator of survival during cellular stress, notably in malignancies with inherent limitations of oxygen and nutrient supply. mTOR is a serine/threonine kinase which processes signals initiated by nutrient status, growth factors, and cellular stimuli to regulate downstream signaling required for cell growth, metabolism and cell cycle progression. 57 The activation of the PI3K/Akt/mTOR pathway results in cell growth and survival, leading to competitive growth advantage, metastatic competence, angiogenesis, and therapy resistance. See Figure 3.
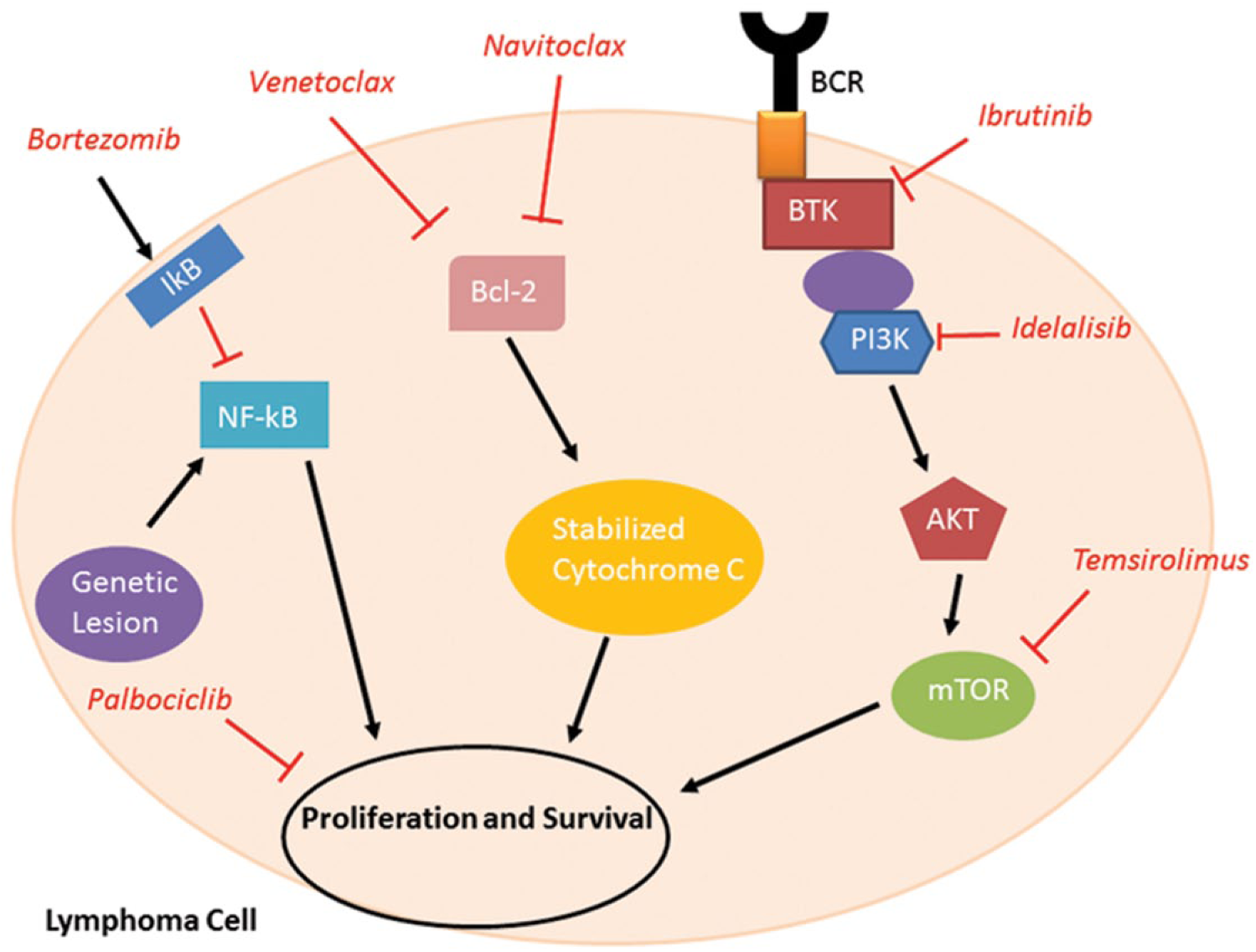
Intracellular targets.
Idelalisib targets the δ isoform of PI3K, an enzyme downstream from the BCR, which signals through Akt and mTOR. Its US FDA approval in 2014 for relapsed iNHLs refractory to both rituximab and an alkylating agent is based on single agent activity with an ORR of 57% (CR 6%), a median DOR of 12.5 months and PFS of 11 months. 58 Idelalisib may be particularly useful in high-risk patients as demonstrated by a post-hoc analysis 59 that showed similar outcomes in patients with FL who relapsed within 24 months after initial chemoimmunotherapy (ORR 56.8%; CR 13.5%; PFS 8 months) as in lower risk patients. Its efficacy, even in chemorefractory patients, was again demonstrated in heavily pretreated iNHLs with an ORR of 47% (CR 1.6%) and PFS 7.6 months. 60 However, several trials evaluating combinations of idelalisib with other agents 61 showed excessive and unexpected toxicities. For example, the combination of LEN, rituximab and idelalisib resulted in significant liver injury, rash, hypotension, lung infection/inflammation and sepsis.62,63 Prominent phase III studies assessing idelalisib combination therapies in CLL and iNHLs were halted due to increased mortality with opportunistic infections such as cytomegalovirus (CMV) reactivation and Pneumocystis jirovecii pneumonia. 64 Efficacy and safety data from second-generation PI3K-δ inhibitors, which have a postulated better toxicity profile, are eagerly awaited. Nevertheless, the current monotherapy use of idelalisib after two systemic therapies in FL is well established and presents a valuable treatment option for chemorefractory patients.
Temsirolimus (TEM) is a selective mTOR inhibitor that inhibits PI3K signaling, which in turn controls translation of cyclin D1. Although TEM is not US FDA-approved for lymphoma therapy, it is approved for treatment of R/R MCL in Europe. As a single agent, it has shown anti-lymphoma activity particularly in R/R FL with an ORR of 53.8% (CR 25.6%) and PFS 12.7 months. 65 Combination of TEM + R in R/R MCL showed an ORR of 59% (CR 19%). 66 A subsequent phase I/II trial consisting of bendamustine + R + TEM in R/R FL and MCL showed a robust ORR 93% (14/15), CR 33% (only seen in MCL patients). Toxicities were predominantly hematologic. 67 Combinations of TEM with other agents are being explored. The relevant mechanism of action makes mTOR inhibitors an attractive agent for combination therapies for both indolent and aggressive lymphomas, however single agent activity is limited.
BCR signaling and Bruton’s tyrosine kinase
Activation of the BCR leads to phosphorylation of numerous downstream protein tyrosine kinases such as Lyn, Syk, and Bruton’s tyrosine kinase (BTK). These kinases can be constitutively activated in several hematologic malignancies. BTK, a cytoplasmic tyrosine kinase, is an integral component of the BCR pathway that acts as a necessary bridge to activate the subsequent downstream cascade following BCR complex activation. It plays an important role in B-cell development, including proliferation, maturation, differentiation, apoptosis, and cell migration.68,69 Ibrutinib is a highly potent, selective and irreversible small molecular inhibitor of BTK, binding to C481 in the kinase domain. It is currently approved for the treatment of MCL after one prior therapy, MZL after one prior CD20-directed therapy, as well as CLL/SLL and WM. In a phase I study of 56 R/R lymphoma patients (FL 16, MCL 9, MZL 4), ibrutinib achieved an ORR of 60% (CR 16%) with overall PFS of 13.6 months with only infrequent adverse events of mostly cytopenias. Of particular interest was the excellent response noted in MCL patients (ORR 78%; CR 33%). 70 An open-label phase II study was conducted in R/R MCL71,72 showing ORR 67% (CR 23%) and a 24-month PFS and OS of 31% and 47% respectively. Common AEs included diarrhea, fatigue, nausea and dyspnea. Additionally, ⩾3 grade bleeding was noted in about 6% of patients and atrial fibrillation in 11%. When combined with rituximab in R/R MCL, the ORR was found to be 88% (CR 44%). 73 Ibrutinib appears to increase Bcl-2 dependence in CLL patient samples 74 and combination studies of ibrutinib plus the Bcl2 inhibitor venetoclax (VEN) are ongoing (see also below). 75
In addition to MCL, ibrutinib has activity in MZL as demonstrated by Noy and colleagues with a reported ORR of 51% (CR 12%) and PFS of 18 months.76,77 AEs included anemia (14%), pneumonia (8%), atrial fibrillation (6%), and two cases of grade ⩾3 bleeding. This trial led to the recent US FDA approval in MZL. Unfortunately, ibrutinib has not been as efficacious in FL with lower ORR and CR rates,78,79 specifically in R refractory patients (ORR 11% versus 42% in R sensitive patients). Second-generation BTK inhibitors, such as acalabrutinib, are in clinical trials and promise an improved toxicity profile and enhanced activity.
Agents targeting the BCR pathway have considerable activity in iNHLs and found their place in the management of R/R MCL, MZL, and FL. However, there is no ‘one size fits all’ answer. For example, ibrutinib has a clear role in the management of R/R MCL and MZL, however less activity in FL. Certain biomarkers may help predict response to these agents with most data available for ibrutinib. These include mutations in MYD88 (increased response in WM) and CXCR4 mutation (less response),80,81 ABC cell type (increased response in DLBCL), 82 CD79B overexpression (increased response in DLBCL), 83 and CARD11 mutations (resistance). 84 While single agent therapy is valuable, rational combination with other agents 85 have the potential to produce highly effective purely biological therapies that may revolutionize the care of iNHL patients.
Apoptosis and survival pathways: NF-kB and Bcl-2
NF-kB activation in lymphomas is highly prevalent and significantly implicated in lymphomagenesis for multiple subtypes. Activation generally up-regulates anti-apoptotic genes thereby providing cell survival mechanisms to weather physiologic stress triggered inflammatory response 86 (see Figure 3). Proteasome inhibitors were the first agents in clinical use to target NF-kB activation. Bortezomib (BOR) is the prototypical drug and US FDA-approved for the treatment of MCL. Regarded to have several different mechanisms, bortezomib is best known for stabilization of IkB (an NF-kB inhibitor) leading to apoptosis, cell cycle or growth arrest and stress response.87–90 BOR showed promise in a phase II study of R/R MCL with an ORR of 41% (CR 21%). 91 In combination with rituximab and dexamethasone, ORR in R/R MCL was 81.3% (CR 43.8%) with a PFS of 12.1 months. 92 In front-line treatment of MCL, BOR has been incorporated into R-CHOP-like regimens demonstrating improved ORR and PFS compared with R-chemotherapy alone.93–95 In other iNHL subtypes, BOR has shown modest activity.96,97 The LYM 3001 trial compared BOR + R with R alone in R/R FL 98 and found improved PFS and ORR of the combination, however increased grade ⩾ 3 AEs without an OS benefit. BOR when added to temsirolimus in R/R NHL resulted in an ORR of 91% among all patients including those with DLBCL. Median PFS in iNHL histologies ranged from 7.5 to 16.5 months. 99 BOR is clearly an active drug in MCL, especially if combined with other agents, and multiple studies are evaluating BOR combinations in other iNHLs.
Bcl-2 apoptotic pathways regulate the precarious balance of pro-survival and pro-apoptotic proteins. Under conditions of stress, inhibition of Bcl-2-like proteins leads to destabilization of mitochondrial membranes with release of apoptogenic molecules. 100 Constitutive Bcl-2 oncogene activation, such as with t(14;18) found in FL, plays an important role in lymphomagenesis (see Figure 3). Navitoclax was an early inhibitor of BCL-2, BCL-X and BCL-w with significant activity against lymphoma. Unfortunately, a phase I study of navitoclax in NHL showed propensity towards thrombocytopenia given the implication of BCL-X in platelet survival. 101 This dampened further development. VEN is a BH-3 mimetic and specific inhibitor of Bcl-2 which shifts the regulatory balance towards apoptosis. Despite concerns in early phase trials relating to tumor lysis syndrome deaths, a modified stepping dose protocol overcame this issue and impressive clinical activity led to expedited US FDA approval in CLL. A phase I study of VEN in NHL (including MCL, FL, MZL, DLBCL, tFL, and WM) demonstrated good tolerability and signaled efficacy. 102 A total of 28 patients with MCL had an ORR of 75%, CR of 21%, and PFS of 14 months. The FL subgroup, consisting of 29 patients, had an ORR of 38%, CR of 14%, and PFS of 11 months. MZL had three patients treated with two partial responses and no CR. VEN, when combined with ibrutinib in R/R MCL, demonstrated good tolerability and efficacy with data from 8 of 24 planned patients reported. 75 VEN was also combined with rituximab ± bendamustine in an ongoing phase II trial of pretreated FL. ORR appears improved with triple therapy (56–68%) albeit at the cost of increased gastrointestinal and hematologic toxicity. R-VEN showed 33% ORR in this population. 103 Bcl-2 inhibition offers an attractive and logical target in treating lymphoma with encouraging single agent activity in iNHLs, notably for MCL and CLL/SLL. Rational combination therapies of venetoclax with rituximab and other agents will certainly play a prominent part in the future management of iNHLs.
Cell cycle dysregulation is implicated in lymphomagenesis, particularly in MCL, where cyclin D1 overexpression is a hallmark. Palbociclib, or PD0332991, is a selective CDK4/6 inhibitor, which primarily causes G1 cell cycle arrest in MCL through blocking Rb protein phosphorylation. 17 patients with R/R MCL were evaluated in a phase Ib study. 104 Notable toxicities were neutropenia, thrombocytopenia, fatigue and diarrhea. Of 16 evaluable patients, responses were seen in 3, 1 of which achieved CR. PFS was 4 months signaling efficacy. The experience with CDK4/6 inhibitors in breast cancer will hopefully encourage further investigation in iNHLs.
Conclusion
The increasing number of molecular targeted agents is revolutionizing the treatment of patients with iNHLs. Most data is available for the use as single agents or in combination with CD20-mAbs in the R/R setting, where impressive responses especially in high-risk or otherwise chemotherapy-refractory patients can be observed with manageable toxicities. However, their true potential lies in rational combinations of targeted drugs and the possibility of purely biological therapy that can precisely address disease specific deregulated pathways in a synergistic approach not commonly achievable with cytotoxic therapy. Biomarkers are emerging that can help inform the likelihood of response to specific agents prior to treatment initiation, although thoroughly validated predictive markers are still lacking. The choice of an optimal therapy is often limited by the inherent problems of interpreting outcomes of small subsets of patients in single arm trials without a control population. In order to further advance our understanding of the true potential of these agents in iNHLs, clinical trial enrollment remains the gold standard of care. When clinical trial enrollment is not possible, patient and disease specific variables must be considered in choosing a targeted therapy. Limited approved indications currently prohibit oftentimes access to novel therapies and use frequently remains off-label. As more clinical data become available for specific iNHLs, we must remain tireless advocates for our patients in a climate where managed care organizations often become adjudicators on treatment options.
Effective and safe combinations of targeted biological agents have already resulted in better therapy for patients with iNHLs, including those with high-risk disease. In our enthusiasm for the novel drugs, we must however remain wary of potentially serious and unexpected toxicities as noted in recent clinical trials stemming from unforeseen off-target effects in nonhematological cells or unintended inhibition of physiological immune responses. Treatment with targeted agents, while often well tolerated, may also result in lower rates of CR and commonly requires indefinite administration, thereby exposing patients to complications of long-term use and putting stress on the economics of healthcare. While we continue our quest for the molecular silver bullet to the indolent B-cell lymphomas, development must be a diligent and careful process as we learn to manipulate important cellular pathways to the benefit of our patients.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.