
Abstract
High-grade B-cell lymphomas with recurrent chromosomal break points have been termed ‘double hit lymphoma’ (DHL). The most commonly seen DHL is diffuse large B-cell lymphoma (DLBCL) with t(14;18) and t(8;14) or t(8;22) resulting in overexpression of BCL2 and MYC, respectively. The increased proliferation due to MYC overexpression, without the ability for an apoptotic brake as a result of BCL2 overexpression, results in ‘the perfect storm of oncogenesis’. Thus this disease presents a number of diagnostic and therapeutic challenges for the hematologist. The first and foremost challenge is to recognize the DHL. As different morphological entities can be affected it is incumbent on pathologists and clinicians to maintain a high index of suspicion especially in disease that appears unusually aggressive or refractory to therapy. Diagnosis by fluorescence in situ hybridization (FISH) is a sensitive and specific method for detection of the disease but is time-consuming and expensive. While detection by immunohistochemistry (IHC) is sensitive and correlates with survival, standardized methods for this are not widely agreed upon. The second and equally important challenge in DHL is optimizing clinical outcome in a group of patients for whom the prognosis is widely regarded as poor. While improvements have been achieved by dose escalating standard chemotherapeutic regimens, many patients continue to do badly. Furthermore as a disease of aging many patients are unsuitable for dose-intensive chemotherapy regimens. There are now multiple novel targeted agents in various stages of clinical development that offer hope for better outcomes without undue toxicity. Among the most exciting of these developments include specific inhibitors of both BCL2 and MYC.
Introduction: challenging lymphomas
Traditional pathological diagnosis of lymphoma has been based upon morphological appearance of involved tissue under light microscopy and definition of lineage by immunohistochemistry (IHC) or flow cytometry. Over recent years there has been increased recognition of the limitations of this approach in adequately differentiating disease entities in terms of clinical outcome, especially among aggressive B-cell lymphomas. Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoma in Western countries [Friedberg and Fisher, 2008; Friedberg, 2012] and is defined by the World Health Organization (WHO) as a ‘neoplasm of large B lymphoid cells’ with a ‘diffuse growth pattern’ [Harris et al. 2008]. However, amongst patients with DLBCL, clinical behavior and responses to therapy can be heterogeneous [Barrans et al. 2010].
The mainstay of therapy for aggressive B-cell lymphoma is R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone) or R-CHOP-like regimens. Chemoimmuno-therapy in DLBCL has improved 2-year overall survival (OS) to greater than 70% [Coiffier et al. 2002; Sehn et al. 2005; Pfreundschuh et al. 2006]. However, an ongoing challenge remains how to deal with early relapsing or primary refractory disease. These patients continue to have poor outcomes even after salvage with high-dose therapy (HDT) and autologous stem-cell transplant (SCT) and are candidates for augmentation of first-line therapy, including addition of novel agents with a view to improving outcomes [Gisselbrecht et al. 2010]. Understanding the genetic drivers of poor prognosis aggressive B-cell lymphomas is key to identifying high-risk individuals, and the prospective identification of patients at risk is a necessary first step.
Patients with high-grade clinically aggressive lymphomas and transformed disease are an enriched population for so-called ‘double hit’ lymphoma (DHL) [Pedersen et al. 2012]. Thangavelu and others in 1990 [Thangavelu et al. 1990] provided an early description of lymphoid malignancies characterized by both t(14;18) and t(8;14) or t(8;22) with resulting concurrent overexpression of both BCL2 and MYC. These lymphomas displayed aggressive biological behavior. The definition of DHL has been expanded over time to refer to high-grade B-cell lymphomas with recurrent chromosomal breakpoints resulting in activation of two or more oncogenes [Aukema et al. 2011]. It is therefore an historical quirk that we retain the name DHL even in an era where we recognize that multiple genetic events occur in the development of most B-cell lymphomas [Cigudosa et al. 1999; Lohr et al. 2012]. Although DH chromosomal changes are recognized in a number of B cell malignancies including follicular lymphoma (FL), acute lymphoblastic leukemia and B cell lymphoma unclassifiable, by far the most common histological subgroup affected is DLBCL. For the purposes of this review unless otherwise specified below DHL will refer to DLBCL with chromosomal translocations that result in overexpression of both BCL2 and MYC proteins.
DHL is important because many authors now believe that standard chemo-immunotherapy alone is insufficient therapy [Friedberg, 2012; Lin et al. 2012] with reports of a median OS of approximately one year [Green et al. 2012b]. Nonetheless, barriers to improving current outcomes are multiple and include: (1) defining a homogenous group of lymphomas to be included in the definition of this disease; (2) optimizing accurate, widely available and timely detection of this high-risk entity in clinical practice; and (3) identification of augmented regimens with meaningfully enhanced antilymphoma efficacy.
Defining DHL: genetics and phenotype
Overexpression of MYC and BCL2 proteins in the same B cell classically arises as a result of chromosomal translocations whereby the relevant genes are juxtaposed to the promoter regions of genes that are constitutively active during B-cell development, most typically the immunoglobulin heavy chain (IGH) gene. The 14;18 translocation juxtaposes the IGH and the BCL2 genes, resulting in overexpression of the anti-apoptotic protein BCL2. t(14;18) is the hallmark of follicular lymphoma, occurring in 85% of patients of European background and 70% of patients with Asian background [Biagi and Seymour, 2002]. The vast majority of cases of follicular lymphoma have high level of expression of BCL2 protein [Pezzella et al. 1990]. In contrast t(14;18) occurs less frequently in DLBCL where it is seen in between five and 30% of cases [Barrans et al. 2003]. BCL2 promotes the survival of cells in the face of major stressors such as DNA-damage and growth factor deprivation. Not only is avoidance of apoptosis through overexpression of BCL2 a recognized hallmark of cancer driving its development [Hanahan and Weinberg, 2000] it also mediates resistance to chemotherapy in experimental models of lymphoma [Schmitt and Lowe, 2001]. This latter attribute likely explains the association of BCL2 overexpression with poorer prognosis in patients with DLBCL treated with CHOP in the pre-rituximab era [Mounier et al. 2003]. It may also underpin the inability of chemotherapy alone to cure follicular lymphoma.
Overexpression of the MYC proto-oncogene due to its juxtaposition with IGH in the t(8;14) or with IGL or IGK in the t(8;22) and t(2;8) light chain variants respectively, influences a multitude of cellular functions including proliferation [Anderson et al. 2015], metabolism and protein synthesis. When a MYC translocation occurs in isolation or in the context of a simple karyotype, as in the case of Burkitt lymphoma, the increase in proliferation is accompanied by increased apoptosis [Fanidi et al. 1992; Murphy et al. 2008]. Morphologically this is recognized by the classical ‘starry sky’ pattern of Burkitt lymphoma. Detection of a MYC rearrangement is thought to confer inferior outcome in DLBCL [Savage et al. 2009; Barrans et al. 2010; Valera et al. 2013]. However in DLBCL, MYC translocations are infrequent as a single hit and are usually found as part of a complex karyotype [Boerma et al. 2009; Smith et al. 2010].
The combination of increased proliferation and reduced apoptosis, conferred by co-expression of MYC and BCL2, results in the ‘perfect storm’ of oncogenesis resulting in aggressive difficult to treat malignancies [Fanidi et al. 1992; Johnson et al. 2009; Li et al. 2012; Pedersen et al. 2012; Cheah et al. 2015]. Although MYC overexpression in isolation results in aggressive lymphoma morphology [Mohamed et al. 2001], at least two studies have found that MYC protein overexpression is clinically more meaningful when associated with BCL2 [Green et al. 2012b; Johnson et al. 2012]. In a study by Barrans and others, MYC rearrangements (often t(8;22)) occurred in approximately 14% of untreated de novo DLBCL, with the incidence of concurrent MYC and BCL2 rearrangements being approximately 10% [Barrans et al. 2010]. The incidence of DH status increases to around 20% amongst patients with aggressive lymphoma transformed from more indolent diseases such as follicular lymphoma [Pedersen et al. 2012]. This may represent acquisition of MYC during the process of transformation. Paradoxically, other studies suggest that the incidence of DHL is approximately the same amongst cohorts of relapsed versus newly diagnosed disease [Cuccuini et al. 2012].
While cytogenetically defined BCL2+/MYC+ DHL accounts for 60–90% of all DHL [Aukema et al. 2011; Petrich et al. 2014], other combinations of translocations seen include BCL6+/MYC+ (approximately 5%), BCL2+/BCL6+/MYC+ (also known as triple hit lymphoma [THL], approximately 8%) [Petrich et al. 2014] as well as rare translocations involving other genes including CCND1, BCL3 and PAX5 [Cheah et al. 2015]. The importance of DHL has been increasingly recognized because of its profound impact on clinical outcome, particularly in DLBCL where early relapse following rituximab-containing chemo-immunotherapy portends a poor prognosis [Gisselbrecht et al. 2010]. One study by Niitsu and others, demonstrated 2-year survival of 23% in MYC+/BCL2+, compared with 65% in MYC+/BCL2-, 81% in MYC-/BCL2+ and 84% in MYC-/BCL2- lymphomas [Niitsu et al. 2009].
DHL are associated with a high prevalence of independent adverse risk factors in DLBCL including B symptoms, high lactate dehydrogenase, advanced age, extra nodal disease, bone marrow involvement, higher Ki-67 (median 80%), Ann Arbor stages III and IV as well as central nervous system (CNS) disease [Niitsu et al. 2009; Savage et al. 2009; Barrans et al. 2010; Snuderl et al. 2010; Friedberg, 2012; Cheah et al. 2015]. Even accounting for high international prognostic index (IPI) scores, DHL status confers a poor prognosis [Le Gouill et al. 2007]. Unlike many conventional DLBCL risk factors the adverse prognosis portended by DHL status is not negated by chemo-immunotherapy with rituximab [Savage et al. 2009]. DHL affects adults of all ages [Cheah et al. 2015] and there is a male predominance [Oki et al. 2014]. Among 129 DHL patients from MD Anderson the most predictive adverse clinical features at diagnosis were poor performance status and stage four disease [Oki et al. 2014].
Optimizing diagnosis of DHL: practical versus purist
Accurate detection of adverse prognostic markers such as MYC and BCL2 as well as other genes conferring DH or TH status including BCL6, CCND1, BCL3 and PAX5 is key to identifying high-risk patients [Petrich et al. 2014; Cheah et al. 2015]. DHL patients are ideal candidates for clinical trials of novel agents and optimization of standard chemotherapeutic approaches, so early and accurate detection is essential.
In routine clinical practice there are two key methods available for detecting dysregulated MYC and BCL2: fluorescence in situ hybridization (FISH) to identify translocations and IHC to identify protein overexpression. FISH is the gold standard for detection of high-risk DH or TH translocation status. It is a reproducible technique that correlates with clinical outcome [Niitsu et al. 2009] and is used to define DHL in the majority of clinical trials. Some authors advocate FISH testing in all new diagnoses of DLBCL [Landsburg et al. 2014], as it is a both sensitive and specific test for DHL status (Figure 1). Over time FISH has become cheaper and hence more widely available, with establishment of standardized reference laboratories. However it can be time-consuming meaning that results may not always be available to prospectively use in planning treatment decisions. In addition, optimal tissue samples are required for this technique.

Detection of DHL by FISH. The G-banded karyotype was 49,XY,+8,t(8;14)(q24;q32),+12, t(14;18)(q32;q21),+r[11]/46,XY[18]. (A) FISH using the LSI MYC (8q24) dual color break apart rearrangement probe (Vysis) showed two intact copies of MYC and one rearranged (split) MYC signal. In metaphases the rearranged 5’MYC signal (red) was located on the derivative chromosome 8 [der(8)der(8;14)] and the 3’MYC signal (green) was located on a derivative chromosome 14 [the der(14)t(8;14)]. (B) FISH using the LSI IGH/BCL2 t(14;18) dual color dual fusion translocation probe (Vysis) identified two IGH/BCL2 fusion signals: one on a derivative chromosome 14 [der(14)t(14;18)] and one on the derivative chromosome 18 [der(18)t(14;18)]. Additional IGH signals (green) were seen on the der(8)t(8;14) and the der(14)t(8;14). A BCL2 signal (red) was present on the intact chromosome 18.
IHC to detect double protein expression is often used clinically to rapidly screen for DHL and when positive every effort should be made to confirm DHL status using FISH. IHC lacks standardization with no reliable cut off for positive used between clinical trials [De Jong et al. 2007]. Furthermore there is currently a paucity of evidence to support changing clinical practice based on the results of IHC alone. It also lacks sensitivity and may miss translocation-positive cases where the translocation is present in less than 40% of cells [Horn et al. 2013]. However, IHC to detect double protein expression is an inexpensive and widely available technique that is commonly utilized in clinical practice (Figure 2). More recently, adoption of standardized IHC methods has been associated with greater predictive value for this technique. With many current trials prospectively examining outcome in patients both by standardized IHC and FISH, the role of IHC in the detection of DHL is likely to become clearer.

Detection of DHL by IHC. IHC of DH DLBCL is characterized by (A) diffuse growth of large B lymphoid cells on H+E with (B) high Ki-67, (C) high BCL2 and (D) high MYC expression.
Using a cut off for positive of ⩾40% MYC positive cells, concurrent MYC and BCL2 were detected by IHC in 21% of DLBCL [Johnson et al. 2012]. Using a cut off for positive of ⩾50%, it was shown that among 77 cases of DLBCL, all patients with a MYC translocation were detected by IHC [Kluk et al. 2012]. Furthermore, in this study 4 out of 77 patients who were positive for MYC by IHC but negative by FISH demonstrated increased MYC transcription by gene expression testing and all IHC MYC positive cases demonstrated a poor prognosis [Kluk et al. 2012]. Others suggest that IHC MYC ⩾ 70% is the optimal cut off giving a sensitivity of 100% and a specificity of 93% for MYC expression as measured by quantitative real-time polymerase chain reaction (QRT-PCR) [Green et al. 2012a]. Among 193 patients with B-cell lymphoma treated with R-CHOP, 29% demonstrated increased MYC and BCL2 expression by IHC: all of whom had a poor outcome [Green et al. 2012b]. In this study only 11% had a detectable MYC rearrangement by FISH and only 6% were DHL by FISH [Green et al. 2012b]. The apparent incidence of DH status appears to increase from around 10% of DLBCL when defined by FISH to between 20% and 30% with IHC [Green et al. 2012b]. The higher incidence of DH status with IHC over FISH likely pertains to detection of protein overexpression driven by mechanisms other than translocations e.g. microRNA overexpression, amplification or mutation [Cheah et al. 2015] (Table 1). Similar issues arise in detection of BCL2 abnormalities by IHC.
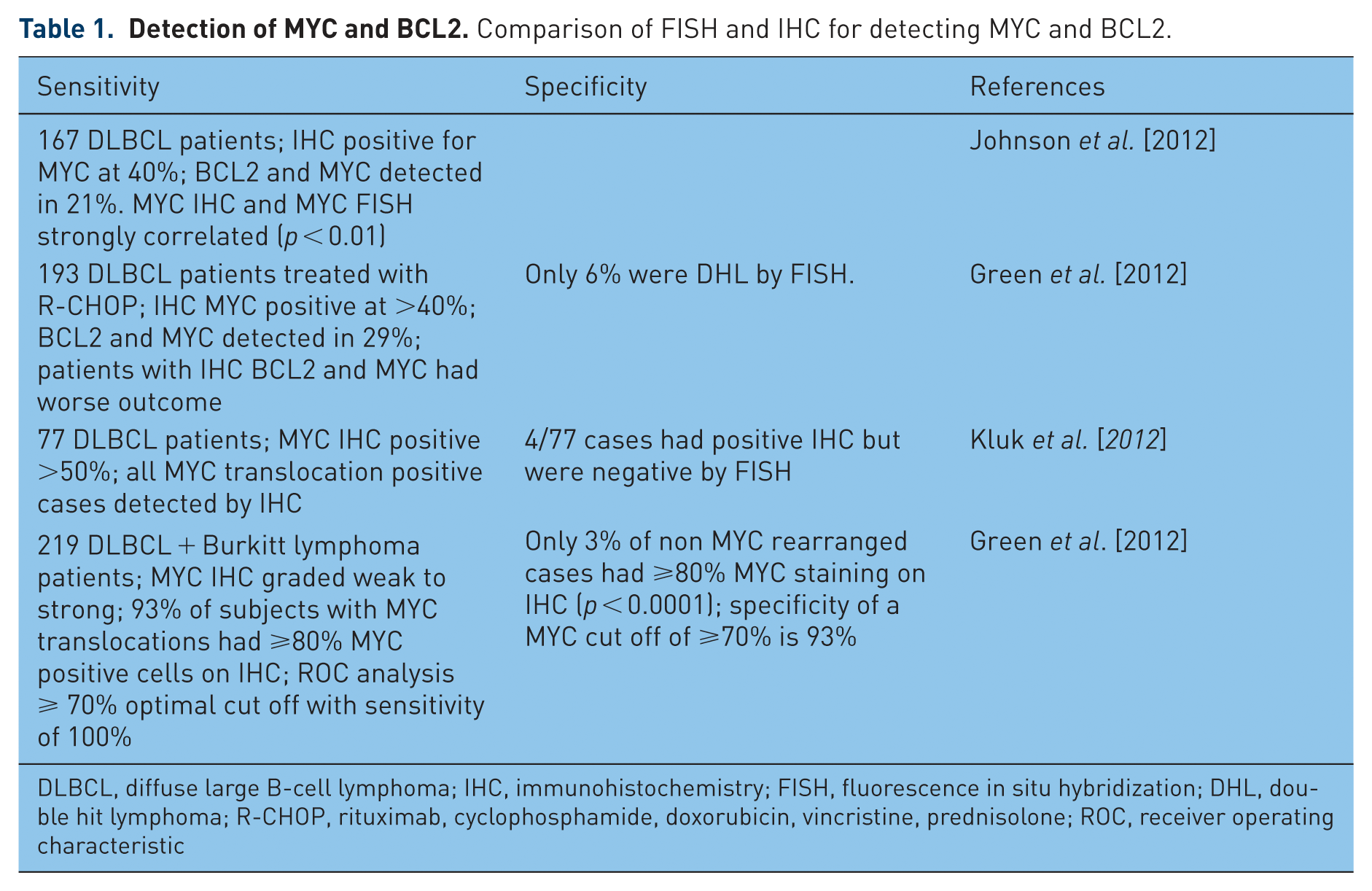
DLBCL, diffuse large B-cell lymphoma; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization; DHL, double hit lymphoma; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone; ROC, receiver operating characteristic
All new diagnoses of DLBCL should have IHC for MYC and BCL2 at a minimum [Friedberg, 2012] and when one or both is positive FISH should be performed for MYC, BCL2 and BCL6 to confirm DHL status. However, the cut off for positive IHC remains controversial in the literature, and in cases that are borderline positive, confirmatory testing with FISH is necessary. A standardized approach to the diagnosis of this entity will facilitate assessment of incidence and optimized management approaches.
Improving prognosis in DHL: incremental versus paradigm shifts
Given the poor outcome seen in DLBCL that relapses early post-chemo-immunotherapy [Gisselbrecht et al. 2010] optimizing therapy remains the key clinical challenge in DHL [Klapper et al. 2008; Oki et al. 2014; Pedersen et al. 2014]. The challenges here are twofold: (1) optimizing chemo-immunotherapy regimens to minimize the incidence of primary refractory and early relapsing disease (collectively, early treatment failure) and (2) salvaging individuals with poor response to initial therapy.
Approaches to optimizing traditional chemotherapeutic regimens, to minimize the incidence of early treatment failure, is critical, as outcomes in these patients remain poor even with HDT followed by autologous SCT [Gisselbrecht et al. 2010]. Variations on R-CHOP, including R-CHOP administered every 14 instead of every 21 days or the addition of etoposide to the regimen, have resulted in incremental benefits in survival of questionable significance, often at the expense of increased toxicity [Pfreundschuh et al. 2004]. Given the poor results with traditional chemo-immunotherapeutic approaches in the early treatment failure setting, much of the current research effort is directed towards evaluation of the safety and efficacy of a multitude of novel agents in the treatment of high-risk lymphoma such as DH DLBCL.
The key challenges in the field of novel agents for DHL and DLBCL in general are (1) defining which combinations of agents optimize clinical outcome while minimizing toxicity and (2) ordering the utilization of new agents and standard chemotherapeutics for example sequential therapy versus maintenance therapy [Anderson et al. 2015]. These challenges are compounded by the fact that DHL, like many cancers, is a disease of aging with a median age of diagnosis in the seventh decade of life [Green et al. 2012b; Johnson et al. 2012]. While the optimal therapeutic approach for this difficult group of patients remains unknown, ongoing clinical trials particularly with novel agents offer the hope of better outcomes for patients in the future [Friedberg, 2012]. Given that DHL patients are often poorly recognized and represent only a subset of poor prognosis DLBCL, much of the available data regarding optimizing treatment in DHL must be inferred from studies in a wider group of relapsed and refractory DLBCL patients.
Optimizing traditional chemotherapeutic approaches for DHL
Despite the prognosis in DHL, R-CHOP chemotherapy remains the backbone of treatment given the good outcomes achieved in DLBCL patients as a whole. Multiple studies have addressed the question of 14- versus 21-day treatment cycles and the addition of etoposide to the regimen [Pfreundschuh et al. 2004]. To date the numbers of patients with DHL included in these studies are too small to define whether this group of patients does better with increased dose intensity or the addition of etoposide, and evidence in favor of such approaches is anecdotal at best. Furthermore the incremental clinical benefit derived from modified R-CHOP-like regimens is not sufficient to justify the additional toxicity. Future clinical trials must prospectively look at outcomes in this high-risk subgroup.
DA-R-EPOCH (dose adjusted rituximab, etoposide, prednisolone, vincristine, cyclophosphamide and doxorubicin) is another variation on the traditional chemo-immunotherapy approach and has demonstrated efficacy and tolerability in patients, median age 50, with untreated de novo DLBCL [Wilson et al. 2008]. However, in this study the impact of MYC status was not assessed. The MD Anderson group looked at 129 cases of DHL treated with R-CHOP, R-EPOCH or R-HyperCVAD/MA (hyper-fractionated cyclophosphamide, vincristine, doxorubicin alternating with cytarabine plus methotrexate) [Oki et al. 2014]. R-HyperCVAD/MA had significantly more complete remissions (CRs) than R-CHOP (p = 0.011) and R-EPOCH was significantly better than R-CHOP in terms of event-free survival (EFS) (p = 0.004) [Oki et al. 2014]. Given the success of R + CODOX-M/IVAC (rituximab plus cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate, ifosfamide, etoposide and high dose cytarabine) in MYC positive Burkitt lymphoma, some authors have considered its use in high-grade large B-cell lymphomas characterized by MYC and BCL2 expression [Corazzelli et al. 2012]. However, tolerability is poor in older age groups and there remains a paucity of data to support a survival benefit.
The traditional role of SCT in DLBCL has been to salvage patients with chemo-sensitive disease on relapse after CHOP [Gisselbrecht et al. 2010]. However in the R-CHOP era, patients with treatment failure within 6–12 months have a poor prognosis, even with HDT and SCT [Gisselbrecht et al. 2010]. This has led some groups to investigate the utility of autograft in first remission as well as allograft for patients at high risk of relapsed and refractory disease, in particular the DHL group. The MD Anderson group looked at SCT in first CR (CR1) among 23 DHL patients and compared them directly to 48 patients who did not receive a transplant [Oki et al. 2014]. Their findings suggest that transplant in CR1 has no effect on OS [Oki et al. 2014]. Furthermore, the utility of transplant is limited by poor tolerability in the elderly and those with multiple comorbidities [Sorror et al. 2005]. Thus SCT in CR1 cannot be recommended based on available evidence.
Finally, DHL status is a recognized risk factor for CNS relapse in DLBCL [Snuderl et al. 2010; Oki et al. 2014] and most authors recommend the use of CNS prophylaxis as part of routine therapy for these patients. Given the poor outcomes associated with traditional therapeutic approaches to DHL and the toxicities associated with many of the dose escalated regimens proposed to mitigate the risk of lymphoma related death, there is no current universally accepted standard of care approach for this condition. Thus, wherever possible patients with DHL should be managed as part of a clinical trial.
Novel targeted approaches to the treatment of DHL
Given the poor prognosis associated with DHL status, it is an area of active preclinical and early phase clinical research for exploring novel approaches to the treatment of difficult lymphomas. As DHL is characterized by overexpression of both BCL2 and MYC, approaches targeting these specific pathways are particularly exciting areas of exploration (Table 2). Due to the relative rarity of DHL, there are few studies looking at this population in isolation. However many lessons pertaining to the optimization of outcomes in DHL may be drawn from studies in the broader group of relapsed or refractory DLBCL.
Targeted therapy for DHL. The two approaches involve (a) inhibition of BCL2 or (b) inhibition of MYC. Ideally the combination of both approaches would be tested in clinical trials along with chemo-immunotherapy.

DLBCL, diffuse large B-cell lymphoma; DHL, double hit lymphoma; R/R, relapsed/refractory; ORR, overall response rate.
Targeting BCL2 and MYC in DHL: the Holy Grail
BCL2 inhibition
BCL2 overexpression impairs a malignant cell’s ability to undergo apoptotic death and underpins the development of malignancy as well as chemo-resistance in many hematological malignancies [Hanahan and Weinberg, 2000; Anderson et al. 2015]. The first extensively validated potent BCL2 inhibitor was the BH3 mimetic, ABT-737 [Oltersdorf et al. 2005]. As a single agent ABT-737 had no single-agent activity in a robust in vivo murine model of BCL2 and MYC overexpressing DHL. However, the combination of ABT-737 with cyclophosphamide demonstrated significant synergy, resulting in better outcomes than achieved with either agent alone, and apparent cures in this model [Mason et al. 2008]. ABT-737 did not have suitable pharmacokinetic properties for clinical development. Consequently, an orally available analogue, ABT-263 [Tse et al. 2008] (now known as navitoclax), was generated and this showed activity with in vitro DHL cell lines [Sasaki et al. 2011].
In addition to targeting BCL2, navitoclax and ABT-737 also targeted the BCL2-family members, BCLxL and BCLw [Anderson et al. 2014]. Very early in its clinical development navitoclax was associated with a dose-dependent thrombocytopenia [Roberts et al. 2012], due to circulating platelet dependence on BCLxL for survival in the periphery [Mason et al. 2007; Zhang et al. 2007]. Thus, in clinical trials of navitoclax dose escalation was limited by on-target thrombocytopenia and the full anti-BCL2 potential of the drug at higher doses may not have been realized. Among four evaluable patients with refractory or multiply relapsed DLBCL on the phase I trial of single agnet navitoclax in NHL, none achieved a partial response (PR) [Wilson et al. 2010], in line with what had been observed in the murine model.
The clinical imperative for dose escalation unencumbered by BCLxL-mediated thrombocytopenia led to the development of a BCL2 selective inhibitor: ABT-199 [Souers et al. 2013]. ABT-199, (now known as venetoclax), demonstrated preclinical efficacy in MYC driven murine lymphoma models [Vandenberg and Cory, 2013] and in DHL cell lines where it appears to produce a cytotoxic effect, especially when used in combination with either traditional chemotherapy or other novel agents [Johnson-Farley et al. 2015]. Venetoclax is currently in early phase clinical trials in patients with relapsed or refractory NHL including DLBCL [ClinicalTrials.gov identifier: NCT01328626]. Preliminary results from the phase I single agent study suggest greater activity than seen with navitoclax, with an 28% overall response rate (ORR) observed among 18 patients with DLBCL [Davids et al. 2014]. Given the success in preclinical studies of combination therapies of BH3 mimetics (ABT-737, venetoclax) and conventional DNA-damaging chemotherapy approaches, the results of ongoing clinical trials with venetoclax in combination with chemo-immunotherapy in broad populations of patients with NHL and related diseases are awaited with interest.
MYC inhibition
Inhibition of MYC is likely pivotal to the development of truly novel approaches to treatment of DHL. Although targeting transcription factors with small-molecule inhibitors has proved technically challenging, there are several agents currently being developed to modulate MYC expression or activity indirectly in vivo. To date, indirect targeting of signaling cascades downstream of MYC has yet to bear fruit. For example, Aurora kinase A and B are upregulated by MYC, and when blocked cells undergo apoptosis [den Hollander et al. 2010]. Yet, a clinical trial of a selective aurora kinase A inhibitor in patients with relapsed or refractory DLBCL saw responses in only three out of 21 patients [Friedberg et al. 2014]. Progress is being made in the targeting of the regulation of MYC activity. Inhibition of the BET bromodomain mitigates the effect of MYC overexpression by preventing signal transduction, important in regulating MYC transcriptional initiation and elongation [Delmore et al. 2011]. JQ1 inhibits the bromodomain BRD4, thereby reducing MYC transcription [Filippakopoulos et al. 2010]. While this agent has demonstrated preclinical activity, including specifically in DHL cell lines [Johnson-Farley et al. 2015], it has not been suitable for clinical development. However, other BET bromodomain inhibitors are currently in phase I clinical trials for patients with relapsed or refractory lymphomas including GSK525762 [ClinicalTrials.gov identifier: NCT01943851] and CPI-0610 [ClinicalTrials.gov identifier: NCT01949883]. Results are eagerly anticipated.
Other novel approaches to DHL treatment: lessons from relapsed and refractory DLBCL
Approaches to modifying the immune system as a way of treating relapsed and refractory DLBCL have been very popular after the stunning success of rituximab in improving outcomes [Coiffier et al. 2010]. While these agents have not been specifically tested in DHL a number are proving promising in relapsed or refractory DLBCL more generally. Approaches currently being explored include optimized anti-CD20 antibodies [Cillessen et al. 2007; Morschhauser et al. 2013], anti CD40 antibodies [Advani et al. 2006], anti-PD1 monoclonal antibodies [ClinicalTrials.gov identifier: NCT02362997] and vascular endothelial growth factor (VEGF) antibodies [Willett et al. 2004; Stopeck et al. 2012]. In the search for efficacy, some monoclonal antibodies have been conjugated to a variety of drugs and radioactive molecules [Bartlett et al. 2013; Advani et al. 2010; Ribrag et al. 2014; Morschhauser et al. 2004]. More recently, bispecific T-cell engager (BiTE) antibodies with specificity to both B and T cells have been developed in order to enhance T-cell-mediated tumor cytotoxicity [Viardot et al. 2011]. Modified autologous T cells engineered to recognize CD19, also known as chimeric antigen receptor T cells (CART cells) have shown promise in clinical trials of relapsed or refractory DLBCL [Kochenderfer et al. 2013; Kochenderfer et al. 2015]. Finally drugs such as lenalidomide, which have immunomodulatory effects on lymphoma, have also shown some efficacy [Witzig et al. 2011].
Kinase inhibitors may also play a role in future attempts to better treat DHL. Data to date in B-cell lymphomas indicate activity for inhibitors of signaling downstream of the B-cell receptor. What role drugs such as ibrutinib [Wilson et al. 2012] or idelalisib [Lannutti et al. 2011; Furman et al. 2014] may play in new combination approaches to DHL is unclear. Currently ibrutinib is one of the few agents in DHL specific trials [ClinicalTrials.gov identifier: NCT02272686].
Conclusions: towards a brighter future
DHL remains a challenging disease on a number of levels. To ensure appropriate diagnosis, there needs to be widespread availability of fast, reliable and affordable detection methods. Once diagnosed, specific treatment strategies are needed, but as yet there is no universally accepted therapeutic approach. While it is widely acknowledged that standard R-CHOP chemotherapy is insufficient to cure many of these cases, alternatives are not clear. Likely ways forward for this disease will come in two guises: (1) intensified regimens using standard agents such as DA-R-EPOCH and (2) inclusion of novel agents that either target the malignant B cell generally (e.g. immunotherapy) or the roots of the DHL problem, overexpression of MYC and BCL2 proteins. The greatest challenge going forward in this disease will be finding new agents that work to ameliorate the poor prognosis conferred by DH status. Wherever possible every effort should be made to accurately diagnose DHL using FISH and confirmed cases should be enrolled in clinical trials both in the upfront and relapsed/refractory setting.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MAA is supported by a Jill and Ross Webster Bequest Fellowship. DCHS and AWR are supported by Fellowships from the National Health and Medical Research Council of Australia (grant numbers 1043149 and 1079560, respectively). This work was made possible through Victorian State Government Operational Infrastructure Support and Australian Government NHMRC IRIISS.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Research funding from AbbVie and Genentech; Employee of Walter and Eliza Hall Institute of Medical Research which receives milestone payments related to venetoclax.