
Abstract
Objectives:
Biosimilar filgrastim was compared with lenograstim for autologous haematopoietic stem-cell transplant (HSCT) in patients with haematological malignancies. Data from a separate group of sibling donors who underwent allogeneic HSCT are also reported.
Methods:
Patients with lymphoma or multiple myeloma (MM) who underwent autologous HSCT with biosimilar filgrastim were compared with a historical control group of patients who received lenograstim. Peripheral blood (PB) cells counts were monitored after 7–8 consecutive days of granulocyte-colony stimulating factor (G-CSF) injection and apheresis was performed on day 8 if PB CD34+ cell count was ⩾10 cells/µl. The target PB CD34+ cell doses were ⩾2.0 × 106/kg (lymphoma), ⩾4.0 × 106/kg (MM ⩾60 years old) or ⩾8.0 × 106/kg (MM <60 years old).
Results:
A total of 259 patients were included in the autologous HSCT comparison (biosimilar filgrastim, n = 104; lenograstim, n = 155). In patients with lymphoma and older MM patients (⩾60 years old), no significant differences were observed between groups with regard to stem-cell mobilization parameters. However, in MM patients <60 years old, all parameters were significantly superior in the biosimilar filgrastim group, including the need for 1 rather than 2 apheresis procedures. No significant differences were observed between groups in median number of days to absolute neutrophil count (ANC) or platelet recovery. In the allogeneic setting, 47 sibling donors received biosimilar filgrastim. Mean CD34+ count at the first apheresis was 6.1 × 106/kg. A total of 13 donors needed a second apheresis and 4 required a third. Among recipients, median days to ANC recovery was 16 (10–28) and to platelet recovery was 13 (9–54).
Conclusions:
Biosimilar filgrastim is as effective as lenograstim for autologous HSCT in patients with lymphoma or MM patients ⩾60 years old. However, mobilization with biosimilar filgrastim appeared to be superior to that with lenograstim in younger MM patients.
Introduction
The mobilization of peripheral blood stem cells (PBSC) is usually achieved through the use of human granulocyte-colony stimulating factor (G-CSF) either as a single agent or in conjunction with chemotherapy [Lee et al. 2000; Mohty et al. 2011]. The most commonly used G-CSFs are nonglycosylated filgrastim, manufactured by recombinant DNA technology from E. coli, or glycosylated lenograstim, which is produced in Chinese hamster ovary cells [Vanz et al. 2008].
In Europe, biosimilars of filgrastim have been available since 2008 and are now in widespread clinical use, with four different products being available [Gascon et al. 2013]. The approval of originator products is based on de novo establishment of the product’s safety and efficacy. The foundation of biosimilar development is rigorous structural and functional characterization and comparative studies to confirm there are no clinically meaningful differences in quality, efficacy and safety between the biosimilar and reference products [McCamish and Woollett, 2013].
Comparable quality, efficacy and safety of the biosimilar filgrastim (Zarzio®) with the originator filgrastim (Neupogen®) was demonstrated by extensive protein characterization together with four pharmacokinetic/pharmacodynamic studies in healthy volunteers and a supportive single-arm phase III study for primary prophylaxis of severe neutropenia in breast cancer patients treated with doxorubicin and docetaxel chemotherapy [Gascon et al. 2010; Sörgel et al. 2010]. Based on the totality of evidence from these studies, extrapolation to indications for which biosimilar filgrastim had not been tested, including haematopoietic stem-cell transplant (HSCT), was considered scientifically justified since receptor site kinetics of both products are comparable and indicate the same mode of action for both, i.e. direct stimulation of bone marrow cells through the G-CSF surface receptor.
Several studies have since shown that biosimilar filgrastim is comparable with the originator when used for HSCT [Lefrère et al. 2011; Ianotto et al. 2014; Reményi, 2014]. A recent review of data from more than 900 patients and healthy donors showed the toxicity profile, PBSC yield and efficacy of biosimilar G-CSFs to be equivalent to historical data with the reference G-CSF filgrastim [Schmitt et al. 2014].
As well as filgrastim, lenograstim is also widely used for HSCT. Although filgrastim and lenograstim are generally assumed to have similar clinical characteristics, they are different molecules and the question of whether there are differences between them in stem-cell mobilization efficacy is not fully resolved [Sourgens and Lefrère, 2011]. In this analysis, we compare the use of biosimilar filgrastim with lenograstim in patients with lymphoma or multiple myeloma (MM) who were undergoing autologous HSCT at St Bartholomew’s Hospital, London, UK. We also report the use of biosimilar filgrastim for the mobilization of PBSC ahead of sibling allogeneic transplant, for which previous data are limited.
Methods
Data from patients with lymphoma or MM who underwent autologous HSCT mobilized with biosimilar filgrastim between October 2011 and April 2013 at St Bartholomew’s Hospital, Barts Health NHS Trust, London, UK, were compared with a historical control group of patients who underwent HCST using a similar mobilization protocol with lenograstim from January 2009 to September 2011.
Data were also collected from a separate group of sibling donors and recipients with haematological malignancies who underwent allogeneic HSCT between October 2010 and April 2013.
PBSC mobilization
Patients and healthy donors were primed with biosimilar filgrastim or lenograstim injected subcutaneously at a dose of ~5 µg/kg daily for 7–8 consecutive days. The same dose and administration schedules were used with both products. Peripheral blood cell counts [white blood cells (WBC) and CD34+ cells] were monitored and apheresis was performed on day 8 if the CD34+ cell count was ⩾10 cells/μl. G-CSF administration and apheresis were continued daily until a minimum PBSC yield was achieved; i.e. ⩾2.0 × 106 CD34+ cells/kg for patients with lymphoma; ⩾4.0 × 106/kg for patients with MM aged ⩾60 years and ⩾8.0 × 106/kg for patients with MM aged <60 years. This target dose was planned as part of a double-autograft strategy and was to ensure sufficient cells for two transplants were collected, thereby avoiding the need to re-harvest stem cells from patients for their second transplant when yields may have been compromised by any further chemotherapy received.
Statistical analysis
All statistical analyses were performed using GraphPad Prism 6 Software. Data were tested for Gaussian distribution using the D’Agostino–Pearson omnibus test. Data sets which did not pass the normality test were assumed to have non-Gaussian distribution. Differences between groups were compared using Fisher’s exact test for categorical variables and the Mann–Whitney test for continuous variables. Data were summarized as median and range. A p value ⩽0.05 was considered to be statistically significant.
Results
Autologous HSCT
A total of 259 patients with lymphoma (n = 74) or MM (n = 185) received biosimilar filgrastim (n = 103) or lenograstim (n = 156) for the mobilization of PBSC ahead of autologous HSCT. Patient characteristics were similar between the two treatment groups, although fewer patients in the biosimilar group had lymphoma (19 versus 35%; p = 0.011) (Table 1).
Baseline patient characteristics.

In patients with lymphoma and older MM patients (⩾60 years old), there were no significant differences between treatment groups with regard to any of the stem-cell mobilization parameters measured (Table 2). However, in MM patients <60 years old, all parameters appeared to favour the biosimilar filgrastim group compared with lenograstim, including the number of aphereses required to achieve minimum yield and the total yield of PBSC (Table 2 and Figure 1).
PBSC mobilization parameters following priming with biosimilar filgrastim or lenograstim.

MM, multiple myeloma; PBSC, peripheral blood stem cells; WBC, white blood cells.
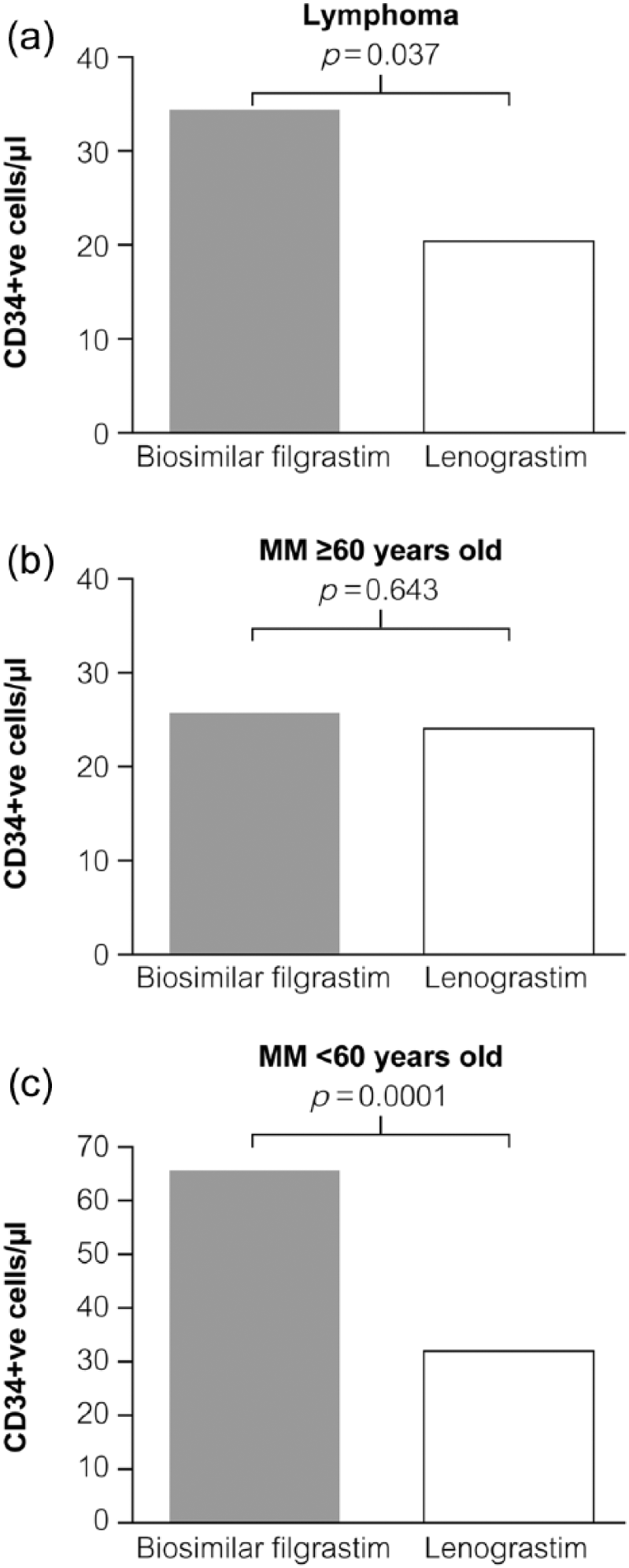
Median (range) CD34+ve cells/µl with biosimilar filgrastim and lenograstim by patient category; (a) lymphoma; (b) MM ⩾60 years old; and (c) MM <60 years old.
Among patients who proceeded to transplant (n = 56 with lymphoma and n = 133 with MM), there were no significant differences in median number of days to absolute neutrophil count (ANC) recovery (>0.5 × 109/l) or platelet recovery (>20 × 109/l) between biosimilar filgrastim and lenograstim (Figure 2).

Number of days to (a) absolute neutrophil count (ANC) recovery >0.5 × 109/l and (b) platelet recovery >20 × 109/l.
Allogeneic HSCT
In the allogeneic setting, 47 sibling donors received biosimilar filgrastim. The median donor age was 52 years (range, 19–69) with a male to female ratio of 26:21. The indication for transplant was acute myeloid leukaemia (n = 11), acute lymphoblastic leukaemia (9), mantle cell lymphoma (5), myelodysplastic syndrome (4), chronic myeloid leukaemia (4), Hodgkin’s lymphoma (3), chronic lymphocytic leukaemia (2), T-cell prolymphocytic leukaemia (2), follicular lymphoma (2) myelofibrosis (2), myeloma (2) and lymphoma (not specified, 1). The median recipient age was 50 years (range, 21–66), median weight was 76 kg (range, 52–137) and the male to female ratio was 38:9. Mean CD34+ count at the first apheresis was 6.1 × 106/kg. A total of 13 donors needed a second apheresis, 4 of whom required a third. Among the sibling recipients, median time to ANC and platelet recovery was 16 days (range: 10–28 days) and 13 days (range: 9–54 days), respectively.
Discussion
Filgrastim and lenograstim differ in their chemical structures and physicochemical properties, and it has been reported that lenograstim is more active than filgrastim in vitro [Nissen, 1994; Querol et al. 1999]. This has been attributed to lenograstim, unlike filgrastim, being glycosylated, which may increase resistance to proteolysis and thereby confer greater stability [Oh-Eda et al. 1990; Wang et al. 1996]. However, glycosylation is not required for receptor binding or biological activity of the protein [Nissen, 1994], and glycosylated and nonglycosylated G-CSF variants have been shown to have the same pharmacokinetic and pharmacodynamic profiles in vivo [Tanaka et al. 1997].
Cumulative data from patients and healthy volunteers suggest there are no clinically relevant differences between filgrastim and lenograstim in their approved indications and no reason to prefer one recombinant G-CSF over the other [Bönig et al. 2001]. However, a small number of studies conducted over the past 15 years or so have continued to suggest differences in mobilization efficacy between the two growth factors. In an early investigation, lenograstim was reported to be superior to filgrastim in terms of CD34+ cell and CFU-GM mobilization in a randomized crossover trial in 32 healthy male volunteers [Höglund et al. 1997]. More recently, in an analysis of 360 allogeneic sibling and unrelated donors, the use of lenograstim rather than filgrastim was associated with superior PBSC mobilization (p < 0.002) [Bertani et al. 2014]. Similarly, in a retrospective study of 146 patients undergoing autologous HSCT, lenograstim achieved adequate mobilization and the CD34+collection target more quickly and with fewer leukaphereses compared with filgrastim [Ria et al. 2014]. In a randomized study with 501 healthy unrelated donors, lenograstim mobilized progenitor cells into the peripheral blood more effectively than filgrastim in men but not women [Fischer et al. 2005]. Also, reduced-dose lenograstim (7.5 µg/kg/day) was as effective as filgrastim 10 µg/kg/day in a randomized study of patients undergoing autologous HSCT [Ataergin et al. 2008].
Conversely, a retrospective case-controlled study of patients undergoing HSCT following high-dose chemotherapy reported that filgrastim significantly reduced the duration of neutropenia, days of G-CSF administration, and led to earlier hospital discharge compared with lenograstim [Kim et al. 2003]. Other studies have reported that no significant differences were observed between lenograstim and filgrastim in patients or healthy donors undergoing PBSC mobilization [Lefrère et al. 1999; Huttmann et al. 2005; Sivgin et al. 2013; Pórez-López et al. 2013].
The introduction of biosimilars of filgrastim raises another question with regard to possible differences between growth factors. Biosimilars of filgrastim are now widely used in the UK and elsewhere and several studies having reported that biosimilar filgrastim is comparable with the originator filgrastim product for peripheral stem-cell mobilization [Bönig et al. 2014]. Although the biosimilar filgrastim used in our analysis has not previously been compared with lenograstim, comparison of a different biosimilar filgrastim product (XM02) with lenograstim showed no differences when given for neutrophil recovery after autologous HSCT, with a median time to ANC engraftment of 11 days for the biosimilar group and 12 days for the lenograstim group [Gardellini et al. 2013].
Similarly, our comparison shows that biosimilar filgrastim is as effective as lenograstim for autologous HSCT in patients with lymphoma or MM patients over 60 years of age. However, in younger MM patients, all mobilization factors appeared to favour biosimilar filgrastim over lenograstim. Reasons for this are unclear, but may represent differences in the patient population or treatment schedules used. For example, factors such as sex, age, donor weight, premobilization WBC count, G-CSF dosing schedules (strength and frequency of administration), disease stage and extent of prior treatment can all influence whether a donor is a good or poor mobilizer [Ings et al. 2006; Bertani et al. 2014]. Although no obvious differences in patient characteristics were apparent between groups in the younger MM patients, it is possible the biosimilar filgrastim-treated group were inherently better mobilizers due to some unidentified factor. Moreover, since the study was not a prospective randomized trial but involved comparison with a historical control group, it is possible that changes in practice over time were a factor.
We also assessed the use of biosimilar filgrastim administered to healthy donors for allogeneic transplant. Data on the use of biosimilar filgrastim for PBSC mobilization in healthy donors are limited and, given the absence of clinical data and the different risk–benefit profile in this setting, concerns over their use have been raised. The World Marrow Donor Association (WMDA), for example, recommends that biosimilars should not be used for mobilization in healthy donors unless the donor is followed on a study [Shaw et al. 2011].
There are a small number of previous reports that compare biosimilar with originator filgrastim use in allogeneic transplant. Schmitt and colleagues reported on 22 donors and patients who received either biosimilar (XM02) or originator filgrastim, with a similar yield of CD34+ stem cells as well as CD3+ T-cells and nucleated cells in both groups and a safe engraftment in all patients [Schmitt et al. 2013] Nine HLA-identical sibling donors mobilized with biosimilar filgrastim (Zarzio®) were compared with nine donors mobilized with originator filgrastim with no significant differences in mobilization outcomes between the two groups [Antelo et al. 2013]. Finally, no differences in efficacy or safety were observed between 26 healthy related donors who received biosimilar filgrastim (Zarzio®) for allogeneic stem-cell mobilization at a single centre compared with a matched historical control group (n = 48) treated with originator filgrastim at the same centre [Lefrère et al. 2013].
In our analysis, biosimilar filgrastim was successfully used to mobilize haematopoietic stem cells in sibling donors for allogeneic transplantation. The minimum CD34+ yield required was achieved upon the first apheresis in most donors (73%) and, on average, 6.1 × 106 CD34+ cells/kg were harvested, which is consistent with previously reported data. Taken together, these preliminary findings suggest biosimilar filgrastim is effective in allogeneic stem-cell mobilization.
However, further studies are required to prospectively compare biosimilar filgrastim with its originator product and assess longer term safety outcomes of using biosimilar filgrastim in healthy donors. A non-interventional, prospective, long-term safety analysis of biosimilar filgrastim in 200 healthy, unrelated stem-cell donors undergoing PBSC mobilization is ongoing. Interim data indicate that biosimilar filgrastim was effective, with the majority of donors achieving the target CD34+ cell dose of 5 × 106/kg body weight of the recipient with a median of one apheresis. The acute-phase safety profile of biosimilar filgrastim was consistent with the known toxicities of G-CSF and no cases of splenic rupture were observed [Becker et al. 2013].
The availability of biosimilars offers many potential benefits, in particular greater affordability. Across the London region, switching from originator filgrastim to a biosimilar was reported to be associated with an estimated annual cost saving of £1 million, with G-CSF purchasing costs being reduced from £3.3 million in 2010 to £2.3 million in 2011 [Gascon et al. 2013].
In conclusion, biosimilar filgrastim appears to be as effective as lenograstim for autologous HSCT in patients with lymphoma or MM. Biosimilar filgrastim was also successfully used to mobilize haematopoietic stem cells in sibling donors for allogeneic transplantation. Evidence to date suggests the use of biosimilar filgrastim for PBSC is effective and safe, and is likely to result in significant cost savings.
Footnotes
Conflict of interest statement
S.A. has received support for meetings and unrestricted educational grants from Amgen, Chugai and Sandoz. The other authors declare no conflicts of interest in preparing this article.
Funding
Medical writing support was provided by Andy Bond, Spirit Medical Communications Ltd, funded by Sandoz.