
Abstract
Keywords
Introduction
Primary tumors of the trachea are rare pathologies, among these is the inflammatory myofibroblastic tumor which is an entity whose etiology has not been established.1–3 However, the presence of an intermediate malignancy potential is considered due to its association with the alteration of the ALK gene which codes for the tyrosine kinase receptor. 4 Histologically it demonstrates a mixed inflammatory pattern accompanied by elongated fusiform well differentiated cells that in immunohistochemistry studies shows up to 50% positivity for ALK.1,5 A prevalence of 0.04–0.07% is currently described among tracheal tumors, with a probability of recurrence between 18% and 40% depending on the resectability of the tumor.3,5,6 The most common symptoms associated with the disease are dyspnea and stridor, as well as persistent wheezing and repeated pneumonia.5,7 However, considering that it is a pathology with low incidence and varied presentation, its diagnosis is usually late. 8 By 2025, only a limited number of pediatric subglottic IMT cases have been reported in the literature, with fewer than ten well-documented cases,9–12 most requiring tracheostomy before or after tumor resection, and only a few achieving immediate decannulation. These reports highlight persistent diagnostic delays and the absence of standardized surgical or postoperative protocols. No established protocol is found in case of incomplete resection. 7
Case description
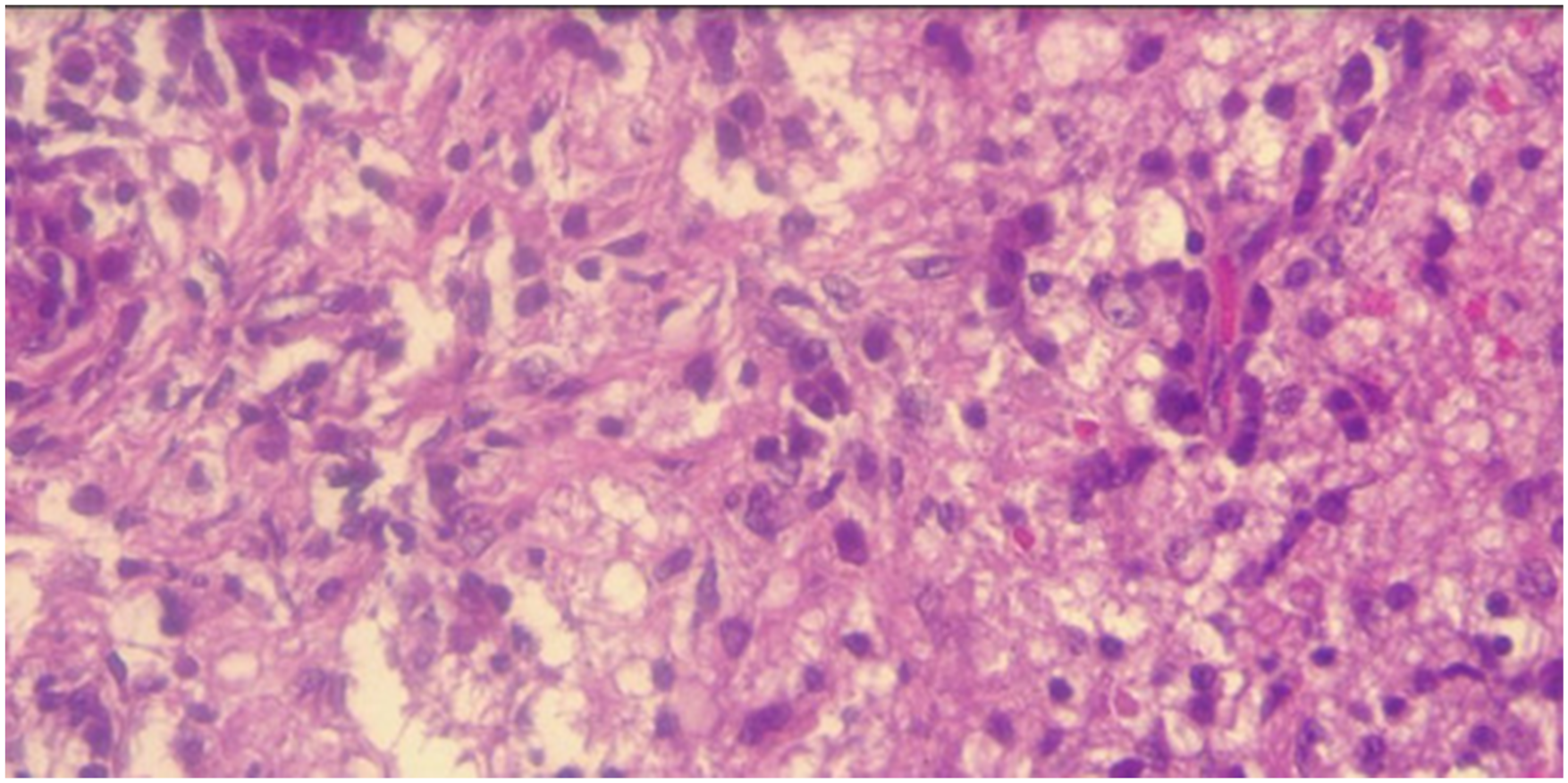
A 10-year-old male patient presented with a clinical picture of progressive exertional dyspnea associated with laryngeal stridor, which was exacerbated at night. He was initially evaluated in the city of Pereira, where diagnostic imaging revealed a nodular-appearing lesion in the left subglottic region that obliterated the airway lumen, measuring 2.7 mm in diameter (Figure 1). Because of these findings at the referral center, a tracheostomy was performed, and he was referred for comprehensive management by a pediatric airway surgery team. At our institution, bronchoscopy was performed, showing a left-lateral tumor lesion of approximately 1 cm in a submucosal position at the subglottic level (at the cricoid and first tracheal ring), which occluded 80% of the airway. The team decided to perform an open surgical procedure (Figure 2), during which they completely resected the lesion and closed the tracheostomy without complications (Figure 3). Bronchoscopy in the first postoperative week demonstrated adequate airway patency and surgical wound healing (Figure 4). After surgical procedure, the histopathological report confirmed an inflammatory myofibroblastic tumor (Figure 5). After 5 years of follow-up, the patient has evolved satisfactorily, is asymptomatic, and does not require supplemental oxygen. Computed tomography of the thorax showing image of nodular appearance dependent on the left subglottic región. This is the only image available due to the limited resolution of the CT scanner used at the referring institution. Surgical visualization of the tumor. Surgical specimen. Bronchoscopy after surgery were the tumor was located. Histopathology of the tumor.



Discussion
Inflammatory myofibroblastic tumor (IMT) could be considered as a reaction of an insult, one of the theories is that it is a product of a response to trauma, viral or autoimmune disease. 13 The incidence of this type of tumor is less than 0.1%, being more common in pediatric age and young people, with a slight predominance in the female sex.7,8 Its malignant potential has been demonstrated due to the presence of metastasis, recurrence and genetic abnormalities. A local recurrence rate of 37% and a metastatic recurrence rate of 11% have been described.3,4,13,14 The intra-tracheal location of this pathology is infrequent, constituting 0.04 to 0.07% of all respiratory tract neoplasms in which 50% involve the bronchial tree and lungs.1,5
The clinical presentation varies from being asymptomatic or presenting: cough, dyspnea, fever, stridor, respiratory symptoms, among others. Constitutional symptoms may also occur in advanced disease.7,13,15 Our patient presented with stridor and exertional dyspnea.
The definitive diagnosis is obtained after the histopathological study of the surgical specimen, however, several previous imaging and paraclinical studies are required.6,13 Radiological findings may be nonspecific, however, CT and MRI can provide tumor information on size, location and relationship to other structures, ultrasound may show images with irregular borders and different echogenicity.1,3,15 This tumor often has increased vascularity on color doppler examinations, CT shows low, equal, or high attenuation compared with the surrounding tissue and MR images may show low signal intensity on T1 and T2. Bronchoscopy could help in the diagnosis of this type of pathology.6,13,16 There is not a specific guide for diagnosis and treatment of Inflammatory myofibroblastic tumors.
Currently, the treatment of IMT consists of surgical resection with a recurrence rate of about 25% when complete resection is not achieved or the tumor behaves aggressively. 14 For surgical planning it is important to know the anatomy, the location of the tumor in relation to other organs, vascularization and whether there is transmural involvement of the trachea. 16 If complete surgical resection is not possible, other systemic therapy options may be required, particularly ALK-directed therapy in ALK-positive IMT.4,9 Even though complete surgical resection confers prognostic value.6,15 Long-term follow-up is mandatory to detect recurrence early. This case contributes new insight to the pediatric airway IMT literature by documenting immediate decannulation at the time of resection, 5 years of recurrence-free survival, and initial diagnostic delay due to asthma misdiagnosis. Given the scarcity of reported cases, collaborative multicenter efforts are needed to improve case characterization, refine surgical strategies, and define long-term prognosis9–12
Conclusion: Inflammatory myofibroblastic tumor is a rare entity, especially in the pediatric airway, and its diagnosis is often delayed due to frequent misdiagnosis as more common conditions such as asthma, which increases the risk of life-threatening airway obstruction. Our case reinforces the need for early endoscopic evaluation of persistent stridor and confirms that complete surgical excision is the gold-standard treatment. Moreover, given the tumor’s intermediate malignant potential and recurrence risk, meticulous long-term surveillance is mandatory. Future collaborative studies across countries are needed to consolidate knowledge on pediatric airway IMT, improve diagnostic accuracy, standardize surgical approaches, and optimize outcomes.
Footnotes
Author’s note
This article was presented at virtual congress: “XXII Congreso Colombiano de Cirugía Pediátrica” September 2020.
Acknowledgements
Hospital Infantil Universitario de San José, Fundación Universitaria de Ciencias de la Salud – FUCS for allowing us to obtain the patient for this manuscript.
Ethical considerations
Hospital Infantil Universitario de San José y Hospital de San José does not require ethical approval for reporting individual cases or case series. Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
Written informed consent from the patient’s mother and legal guardian was obtained and uploaded as a separate document. Informed consent was obtained from the patient’s mother and legal guardian for the use of medical history information and images acquired in the outpatient clinic and surgical procedure.
Author contributions
Idea/Concept: Shary Acosta, Design: Shary Acosta and Lina Barón, Control/Supervision: Diana Romero, Data Collection/Analysis/Literature Review:Shary Acosta, Lina Barón and Diana Romero. Manuscript preparation: Shary Acosta, Lina Barón. Manuscript editing and review: Diana Romero.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. No additional datasets were generated or analyzed.
Declarations
The authors have no financial or proprietary interests in any material discussed in this article. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The manuscript has been read and approved by all the authors and the requirements for authorship have been met.