
Abstract
Inguinal sebaceous gland carcinoma is extremely rare, often mistaken for inflammatory skin lesions, leading to delays in diagnosis and treatment. We reported a rare clinical case of a 59-year-old male patient who presented to the hospital with a lesion in the left groin area, characterized by raised nodules, gradually increasing in size, accompanied by itching. The disease had been progressing for over 3 years, with no prior history of sexually transmitted infections or urinary tract infections. The patient underwent wide local excision surgery with lymph node dissection. Histopathological findings and postoperative immunohistochemistry confirmed sebaceous gland carcinoma presenting in the left groin area with metastasis to 2 groin lymph nodes. After surgery, the patient underwent adjuvant radiation therapy. At the end of the radiation therapy, no tumor recurrence was detected, and no radiation-related toxicity was noted. The patient was discharged and followed up regularly. The patient remains stable after 6 months of follow-up, with no signs of disease recurrence or treatment complications. In conclusion, inguinal sebaceous gland carcinoma is sporadic, so clinical features and optimal treatment methods are poorly understood. Further research is warranted to clarify this rare condition.
Key finding
Introduction
Sebaceous gland carcinoma is an exceedingly rare form of skin cancer, estimated to account for about 0.05% to 0.7% of all skin cancers. 1 The disease originates from the epithelial cells of the sebaceous gland tissue and can manifest in any skin location, most frequently observed on the head and neck area, particularly around the eyes. 2 The disease is infrequent when manifested in the inguinal skin. Based on our understanding and research in medical literature, only 3 cases of sebaceous gland carcinoma presenting in the inguinal skin have been reported to date.2,3 Clinically, the disease is prone to be mistaken for inflammatory skin lesions in sexually transmitted infections and urinary tract infections, leading to delays in diagnosis and treatment. 4 To date, advancements in pathological examination and immunohistochemical techniques enable the accurate diagnosis of this rare condition. Treatment for sebaceous gland carcinoma includes various methods, including surgery, chemotherapy, and radiation therapy, with surgery playing the most crucial role. Radiation therapy is reserved for cases with nerve invasion, lymph node involvement, or when patients refuse surgery. Systemic treatments like chemotherapy, targeted therapy, and immunotherapy are often recommended for metastatic stages. 5 We reported a rare clinical case of sebaceous gland carcinoma in a male patient with metastasis to the left groin lymph nodes.
Case presentation
The patient was a 59-year-old male with a history of lipoma on the neck, shoulders, back, and both arms for 10 years, and alcohol addiction for 40 years, with no history of genitourinary diseases. In June 2023, the patient was admitted to the hospital due to a lesion on the left groin area, which had been present for 3 years. Initially, the lesion appeared as small uneven nodules with itching, gradually increasing in size. The patient had attempted self-treatment with various topical medications without improvement. Clinical examination revealed a 10 mm-sized raised lesion with uneven borders on the left groin area, without ulceration (Figure 1(A), left panel). Laboratory investigations, including complete blood count, blood biochemistry test, and urinalysis, were within normal limits. Pathological examination of the skin lesion showed sebaceous gland carcinoma. Ultrasonography of the groin area revealed a 15 mm-sized left groin lymph node with loss of normal structure, and cytological examination confirmed metastatic carcinoma in the left groin lymph node. Clinical and paraclinical features of inguinal sebaceous gland carcinoma patient. A. inguinal sebaceous gland carcinoma lesion in the left groin area (left panel) and inguinal sebaceous gland carcinoma lesions and metastatic lymph nodes on computed tomography (right panel). B. The surgical incision in the left groin area (6 months after operation) (left panel) and no signs of recurrence on ccomputer tomography 6 months after operation (right panel). C. Microscopy: HE staining and immunohistochemistry.
Rectal endoscopy revealed no abnormal lesions. The thoracic computed tomography (CT) scan demonstrated no detectable abnormalities. The abdominal-pelvic CT scan showed dermal tissue thickening in the left groin region, measuring approximately 4 mm in thickness and 15 mm in length, with imaging features consistent with localized drug absorption following injection. The left groin lymph node had a diameter of 11 mm, also showing drug absorption after injection (Figure 1(A), right panel). Preoperative diagnosis: Skin carcinoma with metastasis to the left groin lymph node. The patient underwent wide excision of the tumor and lymph node dissection. Postoperative findings: in macroscopy, a lobulated mass measuring 1.8 cm in diameter with a solid grey cut surface. On HE staining, tumor cells were arranged in uneven nests, spreading pagetoid in the epidermis, the tumor cells had round nuclei and distinct nucleoli. Metastasis was presented in two groin lymph nodes (Figure 1(C), left panel). At higher magnification, the multivacuolated cells exhibit round to oval vesicular nuclei, punctate nucleoli, and prominent mitotic activity (Figure 1(C), right panel). Immunohistochemistry staining revealed positive for CK7, EMA, while CK5/6, p53, MelanA, HMB45, PAX8, and PSA were negative (Figure 1(C)). Final diagnosis was sebaceous gland carcinoma of the left inguinal skin with metastasis to the left groin lymph nodes. Four weeks after the operation, the patient started adjuvant radiotherapy with a planned dose of 50 Gy in 25 fractions. During and after the radiation therapy process, no radiation-related toxicity was observed. The patient was discharged from the hospital and was regularly monitored every 3 months at the outpatient clinic from September 2023. At 6 months of follow-up, the patient remains clinically stable with no evidence of disease recurrence (Figure 1(B)).
Discussion
Sebaceous gland carcinoma is a rare malignant tumor that can metastasise to lymph nodes or distant sites. The tumor is typically categorised into two types: ocular, which constitutes 75%, and extraocular, which constitutes 25%. Extraocular tumors have a better prognosis due to a lower rate of distant metastasis. Recurrence and distant metastasis rates were 29% and 21%, respectively. 6
The exact pathogenesis of sebaceous gland carcinoma is not yet fully understood. However, related risk factors include advanced age, 7 Asian or South Asian ethnicity, 8 female gender, previous radiation exposure, 9 and genetic predisposition associated with Muir-Torre syndrome. 10
Patient features of the previously reported cases of sebaceous carcinoma of inguinal skin.
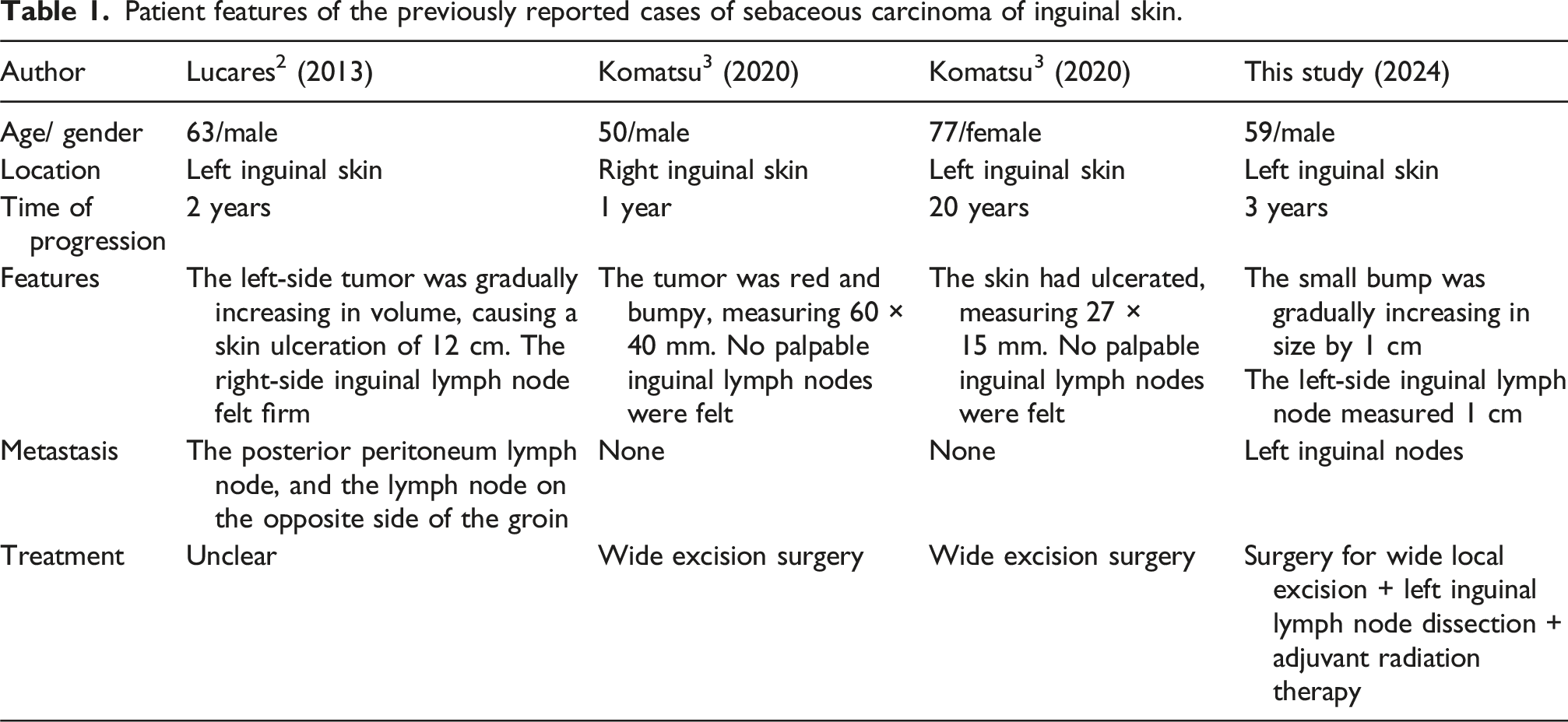
In the 4 cases of sebaceous gland carcinoma manifested on the left inguinal skin (including our one clinical case), the patients’ average age was 62 years old, with a higher incidence in males compared to females (3:1 ratio). The ratio of patients with lesions on the left side of the groin was higher than that on the right side (3:1 ratio). The progression of the disease was slow, with an average duration of 6.5 years. The morphology and size of the tumors were highly varied, ranging from small bumps to extensive skin ulcerations measuring up to 12 cm in diameter. Lymph nodes might or might not be palpable. In the first case, the patient palpated a firm, hard, and adherent lymph node on the opposite side, which was also the case with the largest primary tumor. There seemed to be no correlation between tumor size and lymph node metastasis. For instance, in the second case, the tumor size was 60 × 40 mm with no lymph node metastasis, while in our case, the tumor was 10 mm, yet there were metastases to 2 lymph nodes. This result was also consistent with the findings of Xiaoxue Wang, who reported on 12 cases of sebaceous gland carcinoma manifested in the vulva. 11
Diagnosing sebaceous gland carcinoma poses many difficulties and relies mainly on histopathological examination and immunohistochemical markers. Due to its rarity, it requires differential diagnosis from other primary skin cancers as well as metastatic cancers to the skin and lymph nodes, such as squamous cell carcinoma, basal cell carcinoma, metastatic squamous cell carcinoma, and melanoma. The tumor cells strongly expressed Cytokeratin 7 (CK7) and Epithelial Membrane Antigen (EMA), consistent with sebaceous gland carcinoma. They were negative for Cytokeratin 5/6 (CK5/6) and p63, and the histopathological morphology didn’t show horn pearls or intercellular bridges, ruling out the diagnosis of squamous cell carcinoma. Both sebaceous gland carcinoma and basal cell carcinoma are positive for BerEp4; however, they show different EMA expressions, with EMA typically positive in sebaceous gland carcinoma and negative in basal cell carcinoma. In our case, the positive expression of EMA excluded basal cell carcinoma. Balloon cell melanoma, a rare variant of melanoma characterized by balloon-like, lightly pigmented cells, was also a differential diagnosis. This diagnosis was excluded as the tumor cells in our case are negative for MelanA and HMB45. Metastasis from the kidney and prostate glands was ruled out as the tumor cells were negative for Paired box 8 protein (PAX8) and Prostate Specific Antigen (PSA). 12
Regarding the treatment method for sebaceous gland carcinoma, surgery with complete circumferential peripheral and deep margin assessment remains the standard treatment. 5 It remains uncertain whether lymph node dissection is required. Some authors suggest that for sebaceous gland carcinoma manifested outside the orbital region, the lymph node metastasis rate is only 0.9%, and lymph node biopsy is not recommended for this patient group. 13 However, based on previous individual case reports, the lymph node metastasis rate is relatively high in patients with sebaceous gland carcinoma manifested on the skin of the vulva or penis,14,15 with rates possibly up to 50%. 16 To avoid missing lymph node metastases and minimise the complications of lymph node dissection, lymph node biopsy was recommended for patients with sebaceous gland carcinoma manifested on the inguinal skin.
Postoperative radiation therapy is recommended for patients with sebaceous gland carcinoma manifested outside the orbital region when there is histopathological evidence of perineural invasion or in cases where patients refuse surgery. The role of adjuvant radiation therapy in patients with sebaceous gland carcinoma metastasised to the lymph nodes is not well-established due to the limited number of patients in this group. However, there were small studies suggesting that radiation therapy with a total dose not exceeding 55 Gy significantly reduced the recurrence rate in the area.17,18
In our clinical case, the patient underwent wide local excision surgery accompanied by left inguinal lymph node dissection due to the presence of left inguinal lymph node metastasis confirmed by preoperative cytology. Afterwards, the patient received adjuvant radiation therapy for the tumor, with a dose of 50 Gy delivered in 25 fractions. Evaluation after treatment showed no radiation toxicity and no residual damage detected. The patient has been discharged for 6 months and continues regular follow-up involving clinical examinations, blood tests, and soft tissue ultrasound of the groin, none of which have demonstrated evidence of disease recurrence. The patient continues to maintain a complete response. We will continue to monitor the patient every 3 months for the first 2 years and every 6 months thereafter to detect and intervene early if the disease recurs.
Conclusion
Sebaceous gland carcinoma manifested on the skin is an extremely uncommon condition. Through reporting clinical cases, we aim to share information about the clinical characteristics and experiences in the diagnosis and treatment selection for this rare condition, contributing to improving the prognosis for patients with sebaceous gland carcinoma.
Footnotes
Acknowledgments
We acknowledge the patient and all the participating author for their contribution to the paper.
Consent for publication
The information and images included in this article have received written consent from the patient for publication and research purposes.
Author contributions
Khanh Ha Nguyen is the primary author of the article. She played a key role in the diagnosis, treatment consultation, and patient communication. In addition, she contributed to drafting the main sections of the article and revising both the content and references. Thanh Trinh supported the diagnosis, treatment, and post-discharge follow-up of the patient. She was responsible for creating tables, gathering imaging and pathology data, and assisting in the preparation of the literature review for the case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analysed during this case report are included in this article. Further enquiries can be directed to the corresponding author.