
Abstract
Pediatric retinoblastoma survivors exhibit visual deficits. How these visual deficits impact reading skills is unknown. The purpose of this study is to assess reading level, reading acuity, and reading speed among retinoblastoma survivors. Parents of English-speaking retinoblastoma survivors between ages of 8 and 17 consented/assented to participate. Children completed MNRead for reading speed and reading acuity. The Gray Oral Reading Test-Fifth Edition (GORT) was administered to assess reading rate, accuracy, fluency, and comprehension. Five children participated in the study. Two out of five participants fell within the “Below Average” range on the GORT while 3/5 were “Average”. One participant with below average performance ranked below average in all four subtests, while the other participant was below average in accuracy and comprehension only. On the MNRead, all five participants had slower maximum reading speeds and worse reading acuity than the baseline measure for their age. Four out of five participants had a higher (i,e., worse) CPS than their expected baseline measure, suggesting that these individuals may require larger print or higher magnification than their peers to achieve effortless reading. These findings suggest that retinoblastoma survivors may experience reading difficulties. Characterizing the reading challenges in retinoblastoma survivors will be critical in advancing interventions to optimize educational attainment in this population.
Introduction
There are an estimated 20,000 retinoblastoma survivors in the United States, with approximately 350 new diagnoses annually. 1 Retinoblastoma has a near universal cure rate in the United States (>95%). Survivors, as a population, fare quite well in both psychosocial and quality of life measures, although nearly all of these patients have irreversible visual impairment.2–4
Our preliminary evidence indicates that pediatric retinoblastoma survivors exhibit impaired contrast sensitivity and saccades. 5 Whether these findings translate to functional visual deficits, such as reading skills, in this population is unknown. However, impaired contrast sensitivity and saccades have been shown to affect reading ability in individuals with decreased vision due to other conditions.6–10 We hypothesize that decreased contrast sensitivity and saccades may result in decreased reading speed, which is known to impact school performance and may contribute to lower educational achievement in retinoblastoma survivors.11,12 The present study sought to assess the prevalence and magnitude of reading difficulties in this population through an evaluation of reading level, reading acuity, and reading speed.
Methods
Participants
Approval for this study was obtained from the Institutional Review Board at Washington University in St Louis; principles of the Declaration of Helsinki were followed, and written consent was obtained from all patients included in the study. The medical records of all patients with a retinoblastoma diagnosis followed by St Louis Children’s Hospital were reviewed for study eligibility. English-speaking patients between ages of 8 and 17 were eligible. Patients were excluded if they were under active treatment for retinoblastoma including chemotherapy or had completed chemotherapy less than 6 months prior to enrollment, had a pre-existing condition associated with cognitive impairment, or had compromised visual function or impaired activities of daily living. Participants ages 8 to 17 were selected as the MNRead for reading speed and reading acuity has been successfully administered in participants as young as 8 years. Demographic characteristics collected included sex, age at diagnosis, and treatment history. Ocular data was collected, including laterality of retinoblastoma and best-corrected visual acuity (VA) at last follow-up.
Five patients enrolled in the study and completed the reading assessments. Patient ages on the day of testing ranged from 8 to 16 years. All five patients had a history of unilateral enucleation and a best-corrected visual acuity in their remaining eye of 20/30 or better.
Data Collection
Reading difficulties were assessed using the Gray Oral Reading Test-Fifth Edition (GORT) and the MNRead. Testing was administered at the Intellectual and Developmental Disabilities Research Center at Washington University in St Louis. The GORT assesses reading rate, accuracy, fluency, and comprehension and is norm referenced for age 6-23 years old. The GORT has not been used among retinoblastoma survivors, but it has been used among those with decreased vision, including children with strabismus and amblyopia.13,14
The MNRead is as a continuous-text reading acuity chart developed for both normal and low vision individuals. It evaluates reading acuity and reading speed to assess how reading performance depends on print size. It has been used to assess reading performance in children as young as grade 3 with both normal and decreased VA.
Measures
Performance on the GORT is assessed by recording the time a participant spends reading individual passages aloud (rate), the number of words the participant pronounces correctly (accuracy), and the number of questions the participant answers correctly about the passage once the passage has been read and removed from view (comprehension). Rate and accuracy scores are combined to produce a fluency score. The Oral Reading Index (ORI) is the total of the fluency and comprehension scores. Reading rate, accuracy, fluency, and comprehension are reported as percentile ranks and scaled scores. ORI is reported as a standard score. Descriptive ranges are given for scaled scores and the ORI ranging from “Very Poor” to “Very Superior”.
The MNRead produces four measures of reading ability. Reading acuity (RA) serves as an approximation of the smallest print size at which a patient can read an entire sentence without significant errors, with reading performance declining rapidly as this limit is approached. RA measures acuity to the nearest 0.1 LogMAR. Reading speed is measured in words per minute (wpm). The critical print size (CPS) is the smallest print size in LogMAR at which patients can read at their maximum reading speed, indicating the minimum magnification needed for effortless reading.
A final measurement, the Reading Accessibility Index (ACC), is the patient’s mean reading speed across the largest 10 print sizes on the MNRead Acuity Chart, normalized by the mean value for a group of normally sighted young adults. An ACC of 1.00 reflects normal performance while an ACC of 0.00 indicates the patient could not read any sentences in the specified range of print sizes. Values less than 1.00 suggest a reduced accessibility to text in the range of print sizes encountered in daily life, which can be due to slower reading speed, increased CPS, or a combination of both.
Data Analysis
The results of this series are reported and compared to age-based, normative means.
Results
Reading performance and ocular history of 5 retinoblastoma survivors.

adenotes MNRead measures worse than age baseline; SS = Sum of Scaled Scores; ORI = Oral Reading Index; ORI% = Oral Reading Index percentile rank; MRS = Maximum reading speed; CPS = Critical print size; RA = Reading acuity; ACC = Reading Accessibility Index; Pro = prosthesis; BL = bilateral; UL = unilateral.

GORT performance and reading acuity.
All five participants had an ACC below 1.00, indicating a reduced accessibility to commonly encountered texts (Figure 2). The ACC is normalized to normally sighted young adults ages 18-39 years, however, a previous study has defined baseline MNRead measures for ages as young as 8 years.
15
When age at testing was considered, all participants scored below the expected ACC. Oral reading index percentile and reading accessibility index.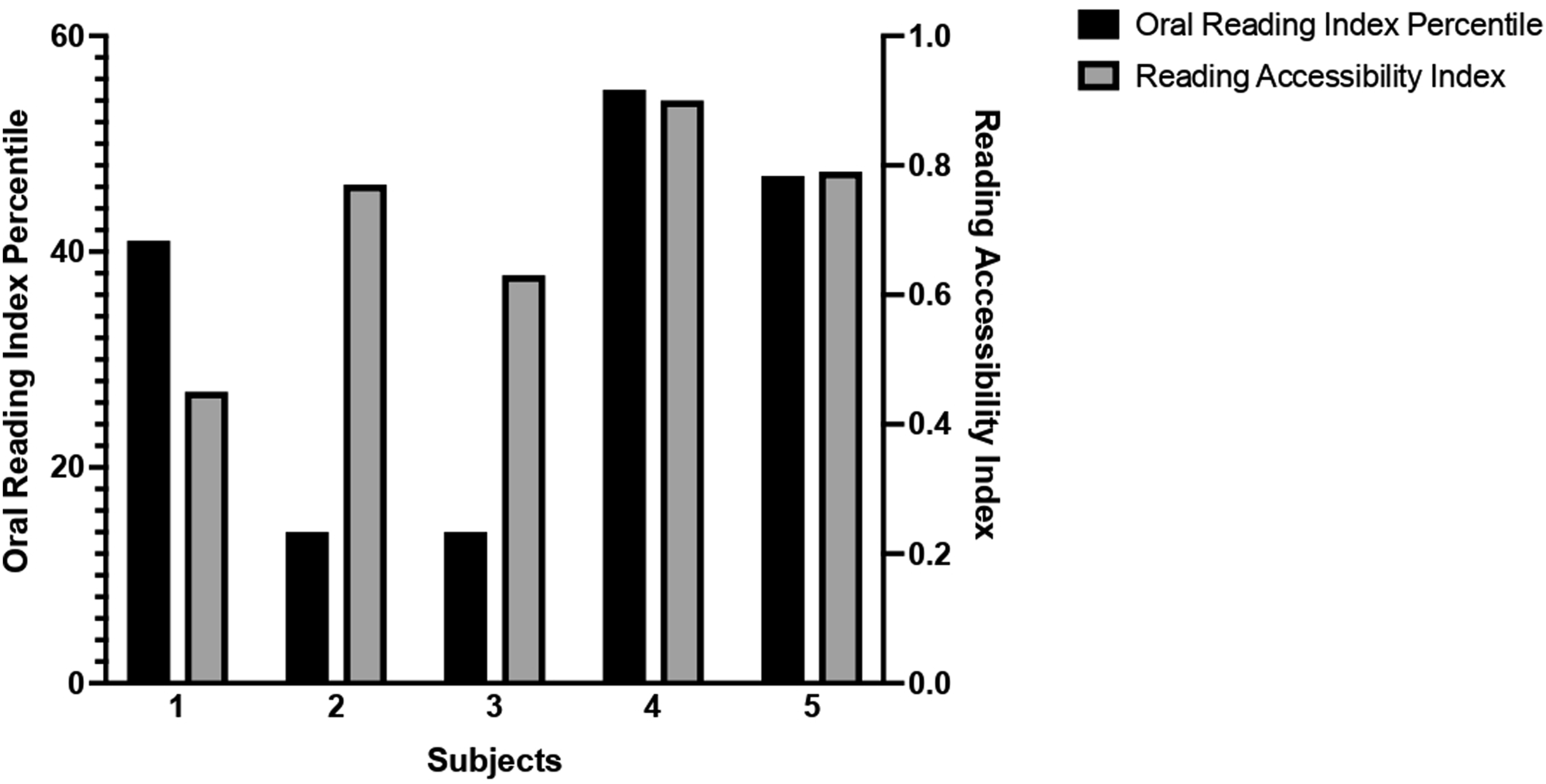
All five participants had slower maximum reading speeds and worse RA than the baseline measure for their age. Four out of five participants had a higher (i,e., worse) CPS than their expected baseline measure, suggesting that these individuals may require larger print or higher magnification than their peers to achieve effortless reading.
Discussion
Our findings suggest that reading difficulties may be common in retinoblastoma survivors, reflected in the observed reading levels, reading performance, and reading acuity. While the significance of these findings is unknown, it is possible that these reading difficulties may impact educational attainment in this population. School modifications based on reading acuity (print size) may benefit these children and compensate for some of these deficits.
Four out of five participants would benefit from a higher magnification of text compared to their peers and all participants had a diminished ability to read text across commonly encountered print sizes, despite all having a best-corrected visual acuity of 20/30 or better. While vision is traditionally measured in terms of visual acuity, other important measures contribute to visual functioning as a whole and thus affect reading ability. Studies of patients with decreased vision due to other causes have shown that impaired contrast sensitivity can lead to decreased reading speed and performance.6–9 Saccades have been identified as another important factor for reading speed. 10
Although visual impairment is a large source of morbidity for retinoblastoma survivors, there is a limited amount of literature on visual impairment in this population due to factors outside of visual acuity, including impaired contrast sensitivity and saccades. Our previous study suggested that a high percentage of retinoblastoma survivors had decreased contrast sensitivity and impaired saccades. 5 The study also noted an association between decreased contrast sensitivity and bilateral disease. 5 Further investigation is necessary to determine whether these findings correlate with the reading difficulties observed in the present study.
Key reading performance measures, ocular history, and demographics.

ORI % = GORT Oral Reading Index percentile rank; ACC = Reading Accessibility Index; Pro = prosthesis; BL = bilateral; UL = unilateral.
Retinoblastoma primarily affects young children at a time crucial for both visual and psychosocial development. Retinoblastoma survivors are a resilient population, with treatment causing minimal negative effects on overall quality of life. Despite this, reading difficulties may be under-recognized in this group. Characterizing these reading challenges will be critical for establishing appropriate academic support for retinoblastoma survivors in order to maximize educational attainment and long-term quality of life. This study was limited by its small sample size. Future studies including more patients and evaluations of reading ability, visual acuity, contrast sensitivity, and saccades would provide further insight into this question.
Footnotes
Author contribution
Sarah Barnett wrote the first draft of the manuscript. All authors made a significant contribution to the concept, design, acquisition and/or interpretation of the data, reviewed and edited the manuscript, and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.