
Abstract
Objective
To investigate the efficacy of all-trans retinoic acid (ATRA) in human gastric dysplasia.
Methods
In this double-blind study, patients with precancerous gastric dysplasia with or without intestinal metaplasia (IM) received either conventional treatment consisting of omeprazole and sucralfate (control group) or conventional treatment plus ATRA. Gastric mucosal biopsies were performed before and after drug treatment and were analysed histologically; expression of retinoblastoma (Rb) protein and HER2 protein in gastric mucosa were measured using immunohistochemistry.
Results
A total of 122 patients were included in the study, 63 in the ATRA group and 59 in the control group. In the ATRA group, dysplasia was attenuated in 43 out of 63 patients (68%) compared with 22 out of 59 patients (37%) in the control group; however, IM was not affected by treatment in either group. ATRA treatment was associated with significantly increased Rb expression and decreased HER2 expression in gastric mucosa.
Conclusions
The use of conventional therapy plus ATRA for gastric dysplasia was associated with improved efficacy compared with conventional therapy alone. It was also accompanied by increased Rb expression and decreased HER2 expression in gastric mucosa. The addition of ATRA to conventional therapy for gastritis may improve the prognosis of gastric dysplasia.
Introduction
Gastric cancer is one of the most common malignancies worldwide, and has a high mortality rate. 1 Among the factors known to contribute to the development of gastric cancer are diets high in salt or smoked foods, cigarette smoking, bile reflux and Helicobacter pylori infection. 2 In addition to dietary and environmental factors, multiple genes may also play a role in gastric carcinogenesis. Important genetic factors include inactivation and mutation of tumour suppressor genes such as the retinoblastoma gene, activation of proto-oncogenes such as HER2, dysfunction of apoptosis genes and instability of microsatellite DNA.3,4 Furthermore, epigenetic alterations have been shown to occur during gastric neoplastic transformation in genes involved in tumour suppression and progression, cell-cycle regulation, cell growth and adhesion.5,6
Similar to other precancerous lesions, gastric precancerous lesions may persist for many months or years before advancing into invasive gastric cancer. 7 Disease progression starts with chronic nonatrophic gastritis, followed by atrophic gastritis, gastric intestinal metaplasia, low- and high-grade dysplasia, and eventually invasive carcinoma. 8 Intestinal metaplasia (IM) is the transformation of gastric epithelium into intestine-like morphology and is known to predispose to malignancy. 8 Gastric dysplasia (also known as gastric intraepithelial neoplasia and noninvasive gastric neoplasia) is an unequivocal neoplastic epithelial alteration in cell morphology and organization. 7 A large proportion of low-grade gastric dysplasia can be reversed spontaneously and endoscopic monitoring with biopsy is recommended. 9 However, severe, high-grade dysplasia requires therapy to avoid its development into invasive cancer.8,10 Thus it is important to identify agents that can induce regression of precancerous lesions or prevent advancement to invasive cancer.
All-trans-retinoic acid (ATRA) is a derivative of vitamin A and a member of the retinoid signalling molecule family. Other important isomer members in this family include 13-cis-retinoic acid and 9-cis-retinoic acid. 11 The functions of retinoids are mainly mediated by two types of nuclear retinoid receptors: retinoid acid receptor and retinoid X receptor, which are members of the steroid and thyroid hormone receptor superfamily. 12 Both types of retinoid receptor form homo- or heterodimers. 13 ATRA is a critical factor for normal embryogenesis and regulates cell proliferation, differentiation and maturation. 14 Clinically, ATRA is approved as a therapeutic agent for acute promyelocytic leukaemia (APL), because of its ability to induce the differentiation of promyelocytes into granulocytes, 15 and for skin diseases such as acne vulgaris. 16 ATRA has also been found to be effective in the treatment of several types of cancers in solid tissues such as thyroid, 17 skin, 18 prostate, 19 breast 20 and cervix. 21 Additionally, the chemopreventive effects of ATRA have been reported in skin premalignant lesions. 22 A low dose of 13-cis-retinoic acid has been shown to be effective in the prevention of human oral carcinogenesis. 23
A possible role for ATRA in gastric cancer has been suggested by its inhibition of gastric cancer cell growth and metastasis in vitro,24,25 and its chemoprevention of gastric precancerous lesions (dysplasia and gastric IM) induced by the chemical carcinogen N-methyl-N′-nitro-N-nitrosoguanidine in rats.26,27 Furthermore, ATRA has been shown to increase survival times in human advanced gastric cancer. 28 Thus, it was hypothesized that ATRA may prevent the progression of premalignant human gastric dysplasia and this was investigated using a randomized controlled trial. In addition, two protein markers were analysed to show gastric neoplastic transformation. The retinoblastoma gene (pRb/p105, RB1 or pRb) was the first tumour suppressor gene discovered in humans, 29 and mutation or loss of this gene has been reported in malignant tumours in many organs including the eye, lung, breast, oesophagus, stomach and colon. 30 The retinoblastoma protein (Rb) regulates the cell cycle and controls cell growth and differentiation; 30 elevation of Rb protein expression has been shown to inhibit proliferation of gastric cancer cells.31,32 The HER2 (NEU, C-erbB-2 or p185) gene encodes a 185 kDa transmembrane glycoprotein with tyrosine kinase activity. 33 Overexpression of the HER2 protein promotes mitosis and is associated with gastric carcinogenesis.34–36 HER2 status has been reported to be associated with gastric cancer, and HER2 overexpression has been shown to be correlated with decreased overall survival.37–39 Therefore, expression of Rb and HER2 were used in the present study as negative and positive markers, respectively, of neoplastic transformation.
Patients and methods
Patients
Patients aged between 20 and 70 years with precancerous gastric dysplasia with or without IM, diagnosed by endoscopy between November 2008 and May 2012 at the First Affiliated Hospital of Henan University of Science and Technology, Luoyang, China, were recruited to the study. The presence of gastric mucosal dysplasia and IM was confirmed by experienced pathologists (L.X. and one other). Exclusion criteria included pregnancy or breast-feeding, stomach cancer, tumours at other sites, upper gastrointestinal bleeding, diseases of the liver, kidney, cardiovascular or cerebrovascular system, and allergy to the drugs used.
The treatment protocol (no. 2008012) was approved by the Ethical Committee of the First Affiliated Hospital of Henan University of Science and Technology, and all patients provided written informed consent.
Treatment
Patients were randomized using a random number table to receive either conventional gastritis therapy alone or in combination with ATRA treatment. Both groups received 20 mg omeprazole (a proton pump inhibitor) twice a day and 1 g sucralfate (a cytoprotective agent for gastric mucosa) three times a day; both drugs were given for 4 weeks. 10 In addition, the ATRA group received ATRA at a dose of 18 mg/m2 body surface area per day for 12 weeks; this was started at the same time as conventional treatment. This dose of ATRA was based on the oral dosage for skin diseases and the duration of treatment was based on a study of retinoid use for the prevention of human oral carcinogenesis. 23 The control group received placebo pills that had the same colour and taste as the ATRA pills. All drugs were taken orally.
Details of the patient's general condition, clinical symptoms and adverse reactions were recorded. Haemoglobin level, white blood cell count, liver and kidney function tests and electrocardiography were performed before and after the drug treatment.
Diagnosis of H. pylori infection
The rapid urease test and the C 13 or C 14 urea breath test were performed before the start of treatment to determine H. pylori infection. When either or both tests were positive, the patient was considered to be colonized with H. pylori.
Pathological assessment
Gastric endoscopy was performed on all patients within 1 week before and 1 week after drug treatment. To ensure an accurate pathological diagnosis, a minimum of three gastric mucosa biopsies were collected 2.5 cm from the pylorus at locations of 3, 6 and 9 o'clock, as well as one from the gastric incisura angularis. Biopsies were also taken from any other abnormal areas seen. The samples were fixed in 10% formalin, embedded in paraffin wax and then sectioned (4-µm thick sections). One section from each biopsied area was then stained with haematoxylin and eosin (H&E) for histopathological examination.
Gastric dysplasia was classified as indefinite, mild, moderate or severe, according to the Vienna classification of gastrointestinal epithelial neoplasia based on the degree of architectural alteration of the epithelium and cytological atypia. 40 A grade of indefinite was used to indicate that there was no evidence of dysplasia. The presence of gastric IM was determined by the occurrence of goblet cells in the section. 41 Patients who demonstrated heterogeneous stages of pathology in biopsy samples were excluded from the study.
Comparison of the grade of gastric dysplasia before and after drug treatment was used to score drug efficacy as highly effective (dysplasia reduced by least two grades), effective (dysplasia reduced by one grade) or ineffective (no change in pathology). The efficacy rate was presented as the percentage of the highly effective, effective and ineffective results compared with the total number of results. Drug efficacy on IM was determined by its absence in H&E-stained sections after treatment.
Immunohistochemistry
Biopsy samples from the pylorus and gastric incisura angularis were also fixed in 10% formalin and embedded in paraffin wax. Sections 4 µm in thickness were cut and mounted on poly-
A semiquantitative method was used to assess the immunohistochemical staining. Analysis of the results was performed by two researchers in a blinded manner. To quantify Rb staining, 10 different fields (at 400 × magnification) were selected from each slide. The number of Rb-positive cells, indicated by a brown staining in the nucleus, was counted in 100 cells per field. The percentage of positively stained cells was scored as 0 for ≤ 5%, 1 for 6–25%, 2 for 26–75% and 3 for > 75%. In addition, staining intensity was scored as 0 for no staining, 1 for weak staining, 2 for moderate staining and 3 for strong staining. The intensity score was added to the percentage score to obtain the final score; a final score of 0–1 was classified as negative, 2–3 as positive and 4–6 as strongly positive.
The numerical scoring of HER2 staining was performed in a similar manner to Rb; HER2 protein staining was located in the plasma membrane. The major difference was that a percentage of positively staining cells < 10% was scored as 0. When the staining was not continuous and weak it was considered to be positive, whereas continuous stain and medium or above medium intensity was considered to be strongly positive.
Statistical analyses
The Wilcox pair-wise test was used to analyse the distribution of dysplasia severity between the two patient groups before treatment. The Mann–Whitney U-test and Ridit analysis were used to analyse differences in the responses of patients to ATRA therapy. Spearman's bivariate analysis was used to determine the correlation between the efficacy of ATRA on dysplasia and the expression of Rb and HER2 proteins. The trend of dysplasia severity after treatment between the groups was analysed by χ2 trend analysis. A P-value ≤ 0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 122 patients with precancerous gastric dysplasia were included in the study. Of these, 59 were randomized to receive conventional therapy alone and 63 also received treatment with ATRA. A further 23 patients were originally recruited but were excluded due to the presence of heterogeneous stages of gastric dysplasia on histological examination (10 in the ATRA group and 13 in the control group).
Patients with precancerous gastric dysplasia randomized to receive either conventional gastritis therapy alone (control group) or in combination with all-trans-retinoic acid (ATRA) treatment.

Data presented as n or mean ± SD.
Grade of gastric dysplasia and presence of intestinal metaplasia before and after either conventional gastritis therapy alone (control group) or in combination with all-trans-retinoic acid (ATRA) treatment.

Data presented as n patients.
aP < 0.05 compared with control group using Spearman's bivariate analysis.
The general condition of patients and symptoms of gastritis in most patients of both the ATRA treatment and the control group were improved after 12-weeks' treatment (data not shown).
During the course of treatment, no severe adverse effects were reported, although several patients in the ATRA group experienced mild abdominal discomfort, dry mouth and dry skin.
Effects on gastric dysplasia
In the ATRA group, 43 out of 63 patients (68%) with dysplasia showed improvement (Figure 1A and 1B), consisting of 22 effective and 21 highly effective results (Figure 2). In contrast, only 22 out of 59 (37%) patients in the control group showed improvement, consisting of 20 effective and two highly effective results (Figure 2). Differences in efficacy between the two groups were significant (Figure 2). However, IM was unaffected by treatment in either group (Table 2) and no regression of dysplasia to atrophic gastritis or IM was observed. No correlations were detected between the response to ATRA treatment and age, gender or the degree of dysplasia in either group (data not shown). Analysis of the dysplasia trend between the groups after treatment using χ2 trend analysis gave a P-value of 0.034.
Histopathology of paired gastric biopsies taken from three patients before (A, C and E) and after (B, D and F) treatment with conventional gastritis therapy plus all-trans-retinoic acid (ATRA). (A) Moderate dysplasia (haematoxylin and eosin, × 400 magnification); (B) mild dysplasia (haematoxylin and eosin, × 400 magnification); (C) immunohistochemistry with antibody to retinoblastoma protein (Rb) showing severe dysplasia and an Rb score of 0 (× 200 magnification); (D) immunohistochemistry with antibody to retinoblastoma protein (Rb) showing mild dysplasia and positive staining in the nuclei of the epithelial cells with an Rb score of 4 (× 200 magnification); (E) immunohistochemistry with antibody to HER2 protein showing severe dysplasia with strong staining for HER2 in the plasma membrane of the epithelial cells (× 400 magnification); (F) immunohistochemistry with antibody to HER2 protein showing mild dysplasia with weak staining for HER2 in the plasma membranes (× 400 magnification). The colour version of this figure is available online at www.sagepub.com. Efficacy rate of conventional gastritis therapy alone (control) or in combination with all-trans-retinoic acid (ATRA) in patients with precancerous gastric dysplasia. Numbers in parentheses are the number of ineffective, effective and highly effective results, respectively. *P < 0.01 comparing number of highly effective cases between the two groups using Ridit analysis; **P < 0.01 comparing overall efficacy rate between the two groups using Ridit analysis.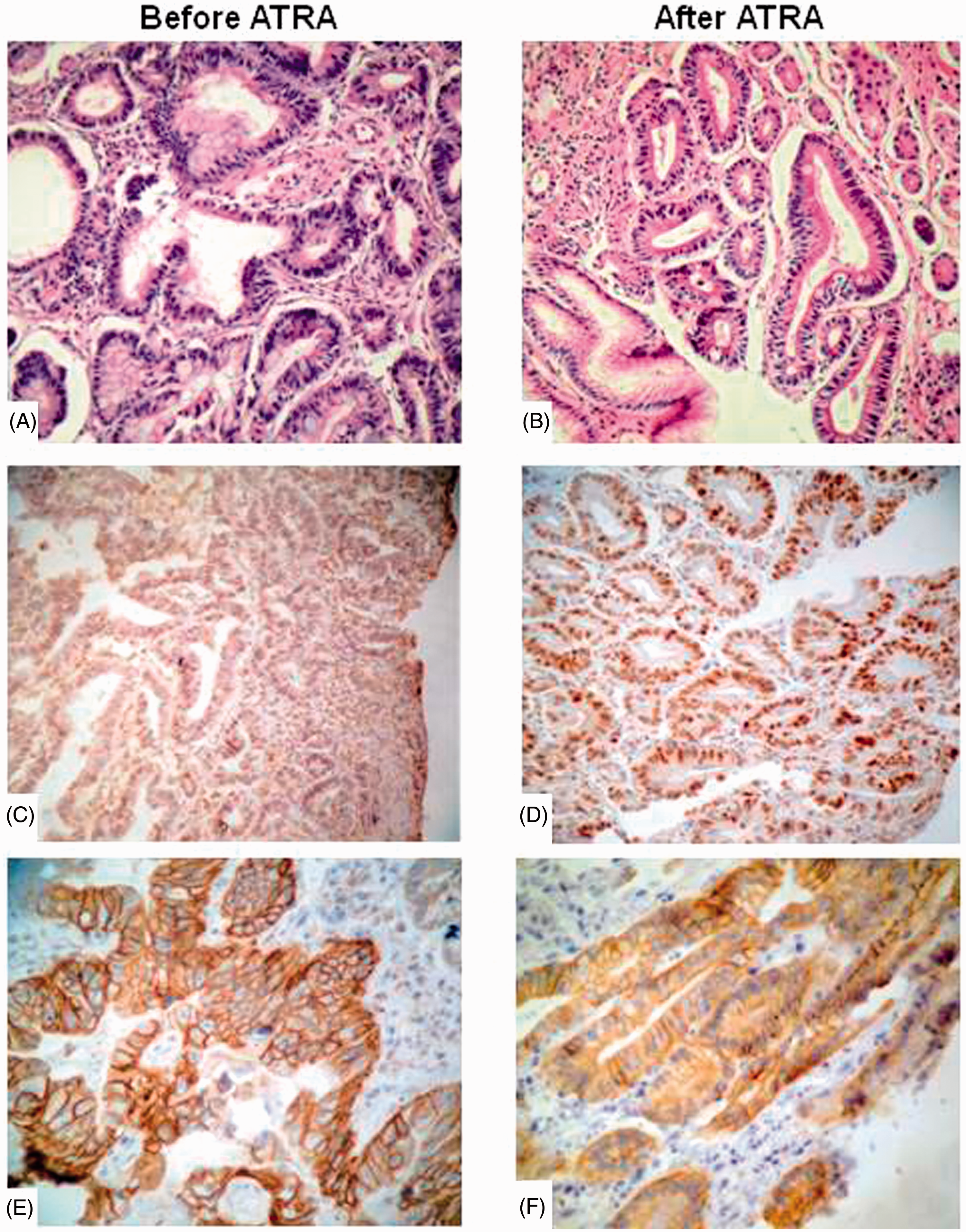

Expression of Rb
Expression of Rb was measured in 50 patients from each group and was compared in gastric mucosa in the ATRA and control groups, and in the same patients before and after ATRA treatment; immunohistochemistry could not be performed on all the patients due to technical problems. Rb would be expected to be expressed at a high level in the nuclei of gastric epithelium without dysplasia. 44 None of the severe dysplastic tissues tested (22 out of 100) was positive for Rb (Figure 1C). In general, the more dysplastic the mucosa, the lower the staining intensity. Patients who improved following ATRA treatment had increased levels of Rb straining in the nuclei of epithelial cells (Figure 1D).
Treatment with ATRA significantly increased Rb expression compared with before treatment and with controls (Figure 3). Interestingly, most patients (10 out of 12) with severe dysplasia and negative Rb expression showed restored Rb expression after ATRA treatment. The dysplasia grade was significantly negatively correlated with the Rb protein expression score (r = −0.32, P < 0.05).
Retinoblastoma protein levels in gastric mucosa before and after conventional gastritis therapy alone (control, n = 50) or in combination with all-trans-retinoic acid (ATRA, n = 50) in patients with precancerous gastric dysplasia. Numbers in parentheses are the numbers of patients with negative, positive and strong positive staining, respectively. *P < 0.05 using Mann–Whitney U-test.
Expression of HER2
Expression of HER2 was measured in 50 patients from each group and was compared in gastric mucosa in the ATRA and control groups and in the same patients before and after ATRA treatment; immunohistochemistry could not be performed on all the patients due to technical problems. HER2 protein was present in all severe dysplasia samples (22 out of 22) (Figure 1E) and in a few moderate dysplasia samples (five out of 71) in the plasma membrane of the epithelial cells. In general, both the number of positive cells and the staining intensity increased with disease progression from mild to severe dysplasia. Furthermore, ATRA treatment significantly decreased HER2 protein levels (Figure 4), even though a few samples still showed moderate dysplasia. The dysplasia grade was significantly positively correlated with HER2 protein expression (r = 0.48, P < 0.05). However, HER2 protein levels were not correlated with the presence of gastric IM (data not shown).
HER2 protein levels in gastric mucosa before and after conventional gastritis therapy alone (control, n = 50) or in combination with all-trans-retinoic acid (ATRA, n = 50) in patients with precancerous gastric dysplasia. Numbers in parentheses are the numbers of patients with negative, positive and strong positive staining, respectively. *P < 0.05 using Mann–Whitney U-test.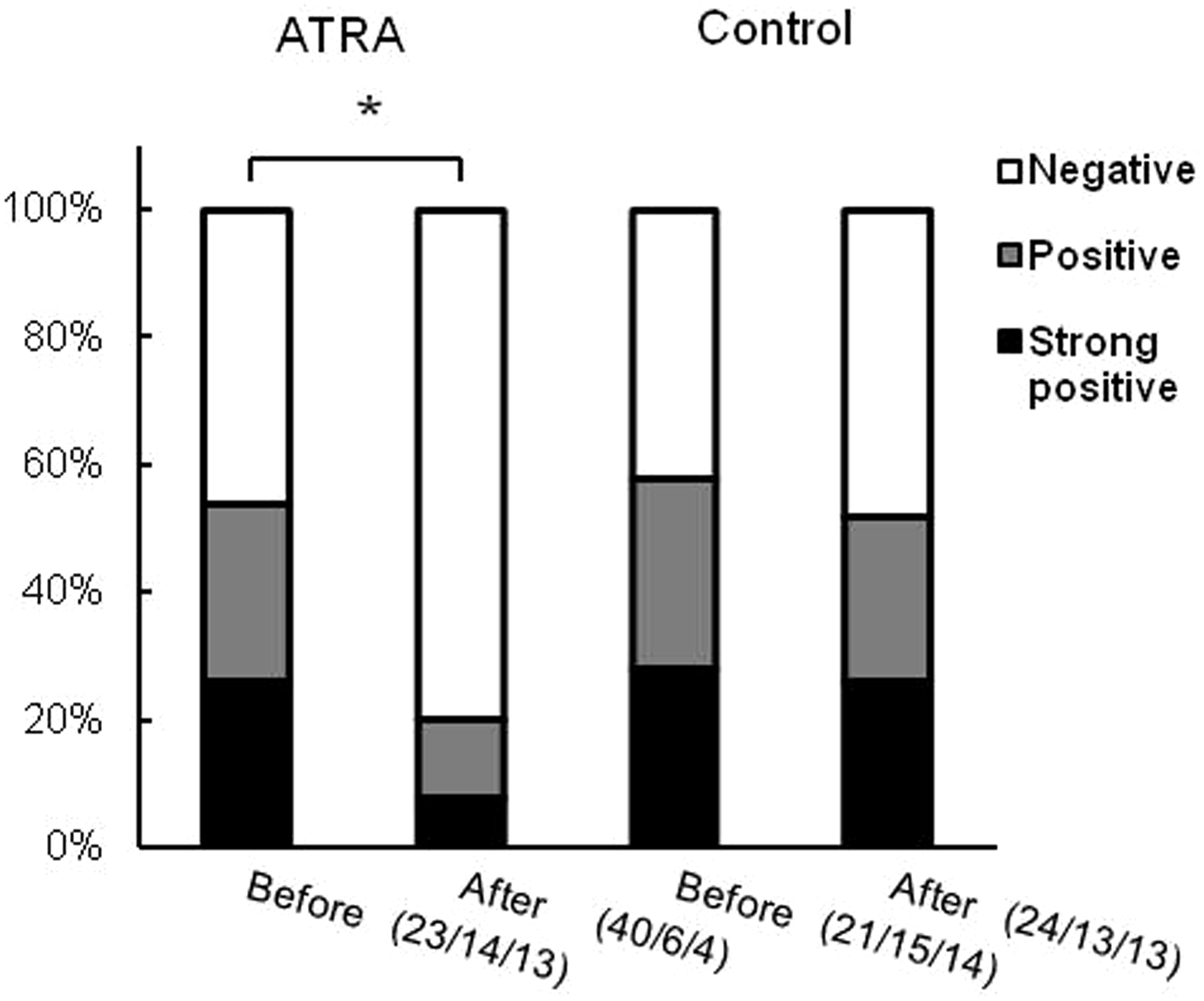
Discussion
The present study demonstrated that the addition of ATRA to conventional therapy improved the prognosis of gastric dysplasia, a precancerous lesion. In addition to morphological analysis, immunohistochemistry was used to quantify levels of the proteins Rb and HER2 as negative and positive markers, respectively, of neoplastic transformation. ATRA-treated samples were shown to have elevated Rb levels, which may contribute to the regression of gastric dysplasia. The Rb gene is a tumour suppressor gene that regulates G1/S phase transition. Rb gene expression has been shown to be decreased in gastric cardia carcinogenesis. 45 The present results support the suggestion that abnormal expression of the Rb gene may be involved in precancerous gastric lesions.
In contrast to Rb expression, HER2 expression was significantly decreased by ATRA treatment in the present study. It has been reported that expression of HER2 is significantly increased in gastric precancerous lesions and carcinoma, and is correlated with poor outcomes in gastric cancer.35,38,39 The humanized monoclonal anti-HER2 antibody trastuzumab has been successfully used for the treatment of HER2-overexpressing breast cancer. 35 In gastric cancer, anti-HER2 intervention also produced promising results in preclinical and clinical studies.35,38 ATRA has been shown to downregulate HER2 protein and mRNA expression in breast cancer cells, possibly through inhibition of the transcription factors activator protein-1 and -2 and specificity protein-1. 46 It is therefore possible that ATRA downregulates HER2 gene expression in gastric lesions. As in gastric cancer,38,39 the results of the present study support the role of HER2 expression as a prognostic marker for gastric dysplasia.
The effects of ATRA on tumour differentiation have been extensively studied.11,12,15,19–21 In human clinical trials, patients with gastric cancer treated with ATRA had a longer survival time compared with control patients. 28 It has been reported that ATRA induced cell-cycle arrest and apoptosis in a gastric carcinoma cell line. 47 It has been suggested that the effect of ATRA on gastric precancerous lesions in rats might be via suppression of proliferating cell nuclear antigen and Bcl-2 protein expression. 48 ATRA may also directly or indirectly inhibit tumour growth through the regulation of cellular and humoral immunity. 49
In addition to the effects of ATRA, improvement of gastric mucosal inflammation brought about by omeprazole and sucralfate may also have contributed to the reversal of gastric dysplasia in the present study, as there was a 37% recovery rate in the control group. It is likely that multiple factors are involved in the regression of gastric dysplasia. In the present study, ATRA treatment was not associated with improvement of IM. It is possible that different mechanisms are involved in these two types of gastric precancerous lesions. It is also possible that some patients were misdiagnosed, as the number of biopsies used was suboptimal 40 and the regression of IM or improvement of dysplasia to atrophic gastritis or other milder gastric lesions may have been missed.
In the present study, no patients reported any severe side-effects or had to terminate treatment before completion of the trial. However, several patients in the ATRA group experienced mild abdominal discomfort, dry mouth and dry skin. Adverse effects such as headache, nausea or vomiting, bone or joint pain and elevated alanine aminotransferase levels, which have been reported in ATRA therapy for APL, 50 did not occur. The lack of severe effects may have been due to the lower dose of ATRA used (18 mg/m2 body surface area per day) compared with the dose used in APL treatment and advanced gastric cancer (45 mg/m2 body surface area per day).28,50
Remission rates reported in the present study suggest that the addition of ATRA to conventional omeprazole and sucralfate therapy for gastritis can improve the prognosis of gastric dysplasia. In addition, ATRA treatment increased Rb expression and decreased HER2 expression in gastric mucosa. Due to the suboptimal number of biopsies and the small number of patients in each group in the present study, it will be important to conduct a larger clinical trial (with a minimum of five biopsies per patient) to validate the efficacy of adding ATRA therapy to conventional treatment for gastric dysplasia.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by a grant (no. 1001011A-4 to J Jin) from the Project of Luoyang Scientific Development, Henan Province, China and partially supported by a grant (no. 81370487 to Q Gao) from the National Natural Science Foundation of China.
Acknowledgements
We thank Drs Fong-Fong Chu, Ran Qi and Yufeng Wang for their help in reading and editing this manuscript. We also thank Dr Junhong Li from Luoyang Central Hospital of Zhengzhou University for his help in the pathological diagnosis of patients, and we thank Lecturer Xiaoyan Xia from Henan University of Science and Technology for her help with the statistical analyses.