
Abstract
Introduction
Spindle cell carcinoma (SCC), also called sarcomatoid carcinoma or carcinosarcoma, represents a rare variant of squamous cell carcinoma that may involve multiple organs, including the larynx. It is a mixed tumor, composed of both malignant epithelial and mesenchymal elements. As the larynx appears to be an unusual site, we report a case of treated SCC laryngeal as well as a literature review of such tumor.
Observation
A 72-year-old male, with 2 months’ history of a progressive worsening dysphonia, was examined. The patient examination showed no cervical adenopathy, while direct laryngoscopy detected a voluminous budding formation of the anterior commissure. A biopsy was performed, in which an undifferentiated carcinoma was identified. The computed tomography (CT) confirmed the existence of a glottic tumor, which completely obstructs the lumen of the larynx. No metastasis were noticed elsewhere on the PET-CT. The tumor was then classified as T3 N0 M0. The patient underwent a total laryngectomy, thyroidectomy and neck dissection. The definitive histopathological analysis confirmed the diagnosis of SCC of the larynx with negative surgical margins. Afterward, the patient underwent adjuvant radiotherapy (RT) on the tumor bed.
Conclusion
Primary laryngeal SCC is a very rare malignancy with a tendency to occur with controlateral lymph node metastasis at an early stage of the disease. Combining surgery and postoperative RT is recommended due to its aggressive profile.
Introduction
Spindle cell carcinoma (SCC), also called sarcomatoid carcinoma or carcinosarcoma, represents a rare variant of squamous cell carcinoma, accounting for less than 1% of all laryngeal malignancies, in adults. 1 The diagnosis depends on the histopathology. Its prognosis varies depending on the age, gender, physical condition, anatomical location and histological type. However, given the few reported cases, analysis of the prognostic factors is poor, 2 as well as evaluation of the clinical and pathological characteristics. Therefore, no standard treatment was established.
Observation
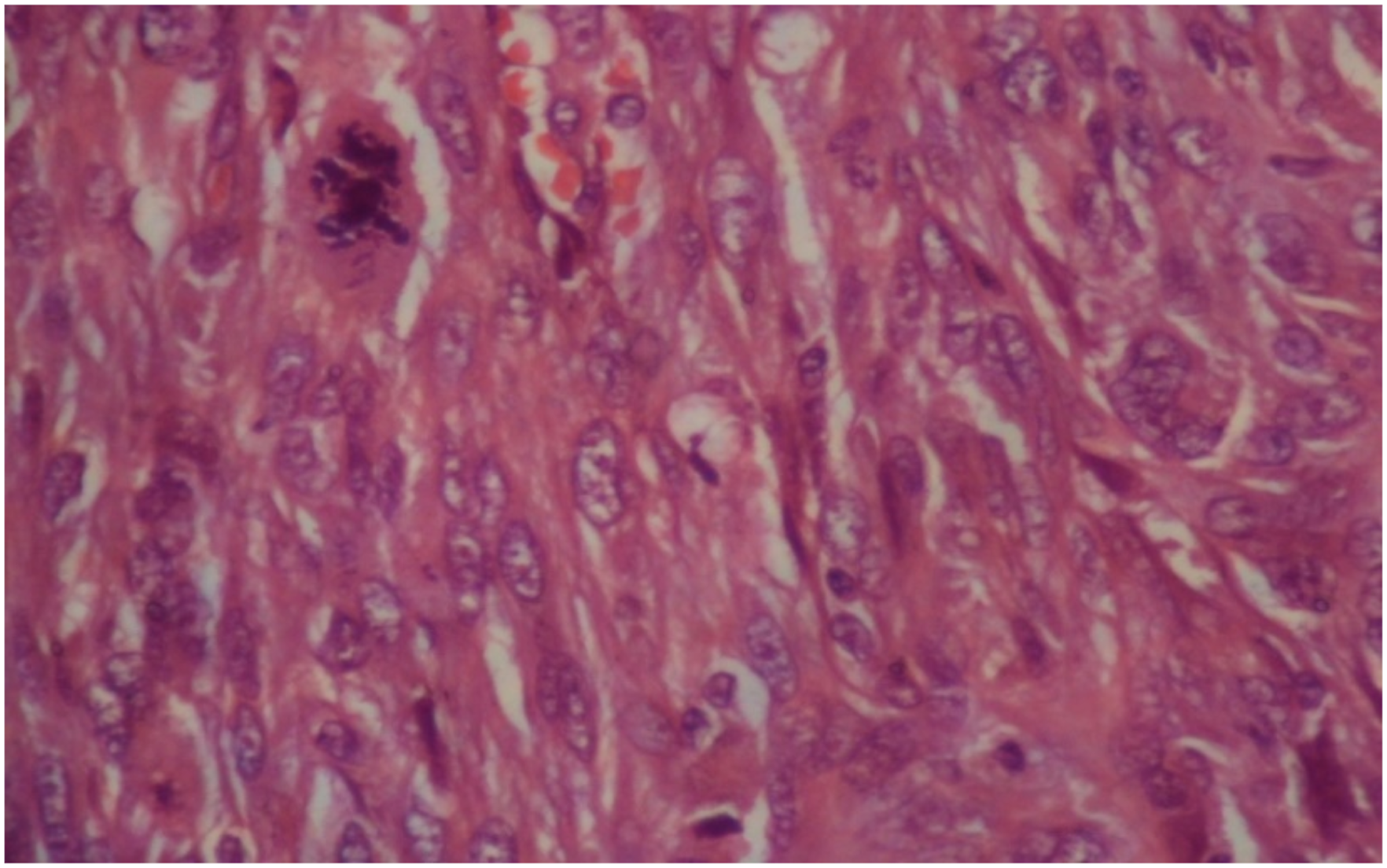
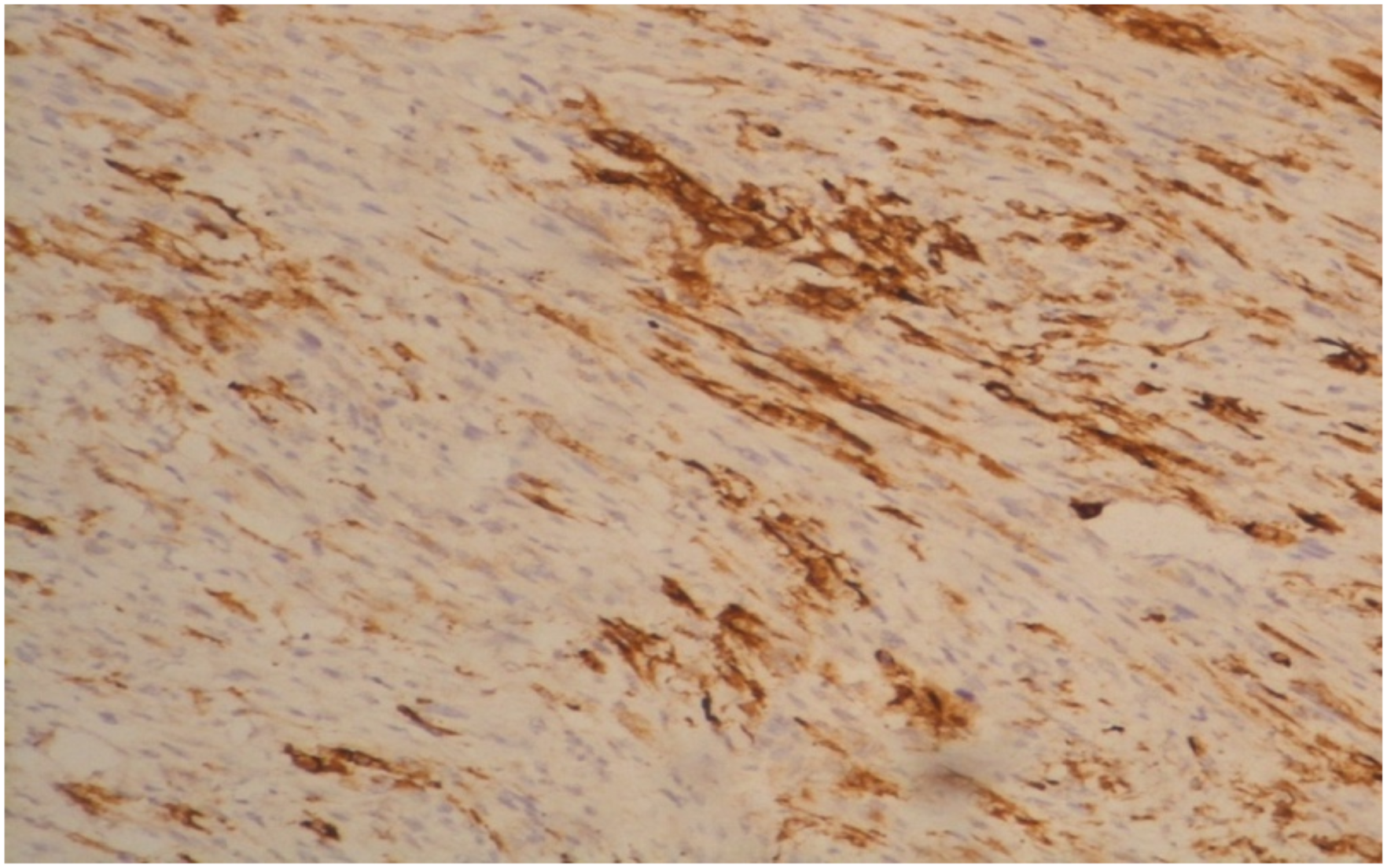
A 72-year-old male with chronic obstructive pulmonary disease history, hypertension and worsening dysphonia but no neoplasia in the family, came consulting. He is a 10 pack year cigarette smoker. Upon examination of the head and neck region, no cervical adenopathy was observed. Direct laryngoscopy revealed a large budding formation of the anterior commissure. The CT confirmed the existence of an obstructive voluminous glottic tumor along the 3 areas of the larynx. Biopsy of the tumor was performed, and microscopic analysis identified the tumor as an undifferentiated carcinoma. No metastasis was noticed elsewhere on the PET-CT. Thus, we classified it as a T3N0M0, according to the TNM 8th edition. Following a multidisciplinary team review, the patient was deemed eligible for surgery and underwent total laryngectomy, thyroidectomy and neck dissection. Gross description identified a tumor that measured 6 × 4 × 5.5 cm. Histopathological analysis showed a biphasic proliferation with carcinomatous and sarcomatous element juxtaposed. Sarcomatous elements were predominant composed of spindle and pleomorphic cells (Figure 1). Abnormal mitosis were identified (Figure 2). Carcinomatous elements were composed of cords and cell islands in a fibrous stroma (Figure 3). These component was highlighted with pancytokeratin by immunohistochemistry study (Figure 4). No Angiolymphatic invasion were found. This biphasic proliferation infiltrated the glottis mucosa without reaching the muscular plane and the cartilage. The surgical resection margins were negative and no lymph node metastasis was found. Eight weeks later, he received 66 Gy of post-operative three dimensional-RT. This low magnification photomicrograph (HEx100) shows spindel cell proliferation with numerous mitosis (arrows). This high magnification photomicrograph (HEx400) shows abnormal mitosis and pléomorphism. This low magnification photomicrograph (pan-CKx100) shows focal stain with cytokeratin highlighting the epithelial component. This low magnification photomicrograph (HEx100) shows cord and cell island representing the epithelial component. JPG

Discussion
SCC is a mixed tumor composed of both epithelial and mesenchymal components, presenting a biphasic aspect.1–3 It was reported in 1951 by Kirklin et al. and called “Spindle cell squamous carcinoma” by Virchow, in 1864. King Jr Was the first to use the term “true mixed malignancy”, in 1976.4,5 The larynx appears to be an unusual site, as only few cases are found in the literature. It represents only 2%–3% of head and neck cancers 6 and less than 1% of all laryngeal malignancies in adults. It occurs mainly in adults, aged between 50 and 79, with a male-female ratio of 13:1. 1 The major risk factors described for laryngeal SCC are alcohol dependence, smoking, and previous irradiation. 7 The symptoms depend on the initial site of the tumor and the involvement of adjacent structures. Patients often experience hoarseness at an early stage with dyspnea at an advanced stage. If the tumor infiltrates the lower pharynx, dysphagia may occur. Endoscopic examination of the larynx, CT, or MRI examination, efficiently evaluate the tumor size and the invasion level. Metastatic lymph nodes of the neck are better appreciated by ultrasound. 7 The PET-CT is used to detect distant metastases.1,7 The diagnosis of laryngeal SCC requires histopathological examination. Immunohistochemistry is not necessary to establish the diagnosis but can be useful to demonstrate heterologous differentiation. The cytokeratin (CK) is positive in the epithelial component and negative in the mesenchymal component, 7 while the vimentin is positive in the mesenchymal component.
The standard laryngeal carcinoma classification is based on tumor size, lymph node invasion, and metastasis (TNM), following the classification scheme of the American Joint Committee on Cancer Staging (AJCC), used in the same way for stage. Most publications on SCC are case series reports. Consequently, no standard protocol of treatment has been established.8–11 The main treatment is surgical resection: complete surgical excision with regional lymphadenectomy. The place of RT is, currently, still a controversial issue. 2
A 13-case study by Yang Zhang et al. strongly recommended a treatment combining surgery and RT in SCC of the larynx (starting from the 2nd stage of TNM). After a follow-up with a mean of 31 months, the seven patients who did receive postoperative RT, at a dose of 66 to 80 Gy, survived with no recurrence. Two patients did not accept adjuvant RT. Those who didn’t have adjuvant RT, died from recurrence, 5 to13 months after the surgery. 12 On the other hand, Ballo et al. suggested that radiation therapy may be used as a single treatment and can be effective for selected patients. 13
Furthermore, a literature review involving 59 patients with laryngeal sarcoma, and mainly treated by surgery (total laryngectomy with thyroidectomy), followed by external RT, along with only 8 cases treated by RT alone, concluded that general survival outcome was better when combining both surgery and RT, as compared to exclusive RT. Moreover, radiation therapy may be an alternative option instead of surgery, in selected patients. 14
In the Philadelphian clinicopathological study about 187 cases, all patients were managed by surgery. The treatment included excision biopsy alone (n: 24 patients), excision biopsy followed shortly by definitive operation (n: 66), and operation followed by adjuvant radiation therapy in 51.9 % of all patients (n:97). The operations included vocal cord stripping, partial laryngectomy, hemilaryngectomy, supraglottic laryngectomy, or laryngectomy with or without lymph node dissection (partial, modified, or radical neck dissection). The radiation treatment involved external beam irradiation of the larynx and neck, with a median dose of 60 Gy (2-72 Gy); it was used alone (after an initial “diagnostic biopsy”) or in conjunction with a salvage procedure (additional surgery after failure to control the tumor). 15 Overall, patients who were managed by surgery alone had a better outcome than patients managed with surgery and postoperative radiation (mean 7.7 years vs mean 6.7 years of follow-up, respectively). Similarly, a lower percentage of patients died from the disease in the surgery group (18.9%), as compared to the surgery and radiation group (42.3%), although there was a longer survival of patients in the radiation group (3.6 years) than in the surgery group (1.9 years). 15
Whereas laryngeal sarcoma is associated with favorable survival, poor prognosis depends significantly on tumor T-stage and location, which are the two most important factors followed by vocal cord movement, anterior history of head and neck radiation therapy and necrosis.15,16 A systematic review published in 2020, included 300 cases of which 240 patients undergoing surgery (total laryngectomy, preservation surgery), 64 patients receiving 60 Gy (33.5–75 Gy) of adjuvant RT, and 12 receiving exclusive RT. Median progression-free survival (PFS) was 48 months, and 224 months of overall survival (OS) were noted in the entire cohort. Poorer PFS was relatively associated with tumor growth in size, cartilage invasion, and positive margins. Authors ended-up suggesting that adjuvant RT may be justified in patients with high-risk factors: tumor size > 3 cm, cartilage invasion, local or distant metastasis. 16
Conclusions
Primary laryngeal SCC is an extremely uncommon malignancy. Although there are no established care standards, surgery is described as the best form of therapy in the literature; adjuvant radiation therapy being an alternative with debatable efficiency.
Footnotes
Author contributions
All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.