
Abstract
Spindle cell carcinoma (SpC), also known as metaplastic carcinoma—spindle cell type, is a subtype of metaplastic carcinoma. Metaplastic carcinomas of the breast are rare but are thought to be more aggressive than invasive ductal carcinomas. Due to their rarity, there are few randomized trials that can inform any standardized approaches to treatment. Treatment is instead extrapolated from other types of breast cancer or metaplastic carcinomas of different locations. Here we present the first known case report of a patient with spindle cell carcinoma of the breast successfully treated with a standard sarcoma neoadjuvant regimen of doxorubicin, ifosfamide, and mesna (AIM) that resulted in >99% necrosis of the tumor and negative margins at the time of resection.
Case report
A 42-year-old female with a large high-grade malignant spindle cell tumor of the right breast was transferred to our institution for further management. She had initially presented to a community hospital due to a rapidly enlarging right breast mass and had a two-core biopsy performed without complication. The pathology of both specimens revealed a malignant spindle cell neoplasm with a mitotic rate of 20 mitoses/10 HPF and approximately 30% necrosis present. There were no glandular structures or areas resembling phyllodes tumor seen on the biopsy. Immunohistochemical staining showed weak cytokeratin 14, p63 and GATA3 expression as well as strong staining for epidermal growth factor receptor (EGFR) (Figure 1). Immunostains for desmin and S100 were negative. It scored 9/9 on Scarff-Bloom-Richardson breast carcinoma grading (tubule formation 3, degree of pleomorphism 3, mitosis 3). Testing for breast biomarkers failed to reveal any estrogen and progesterone receptor expression or HER2 gene amplification. Based on the location in the breast along with weak keratin expression the diagnosis of high grade metaplastic carcinoma—spindle cell type was made.
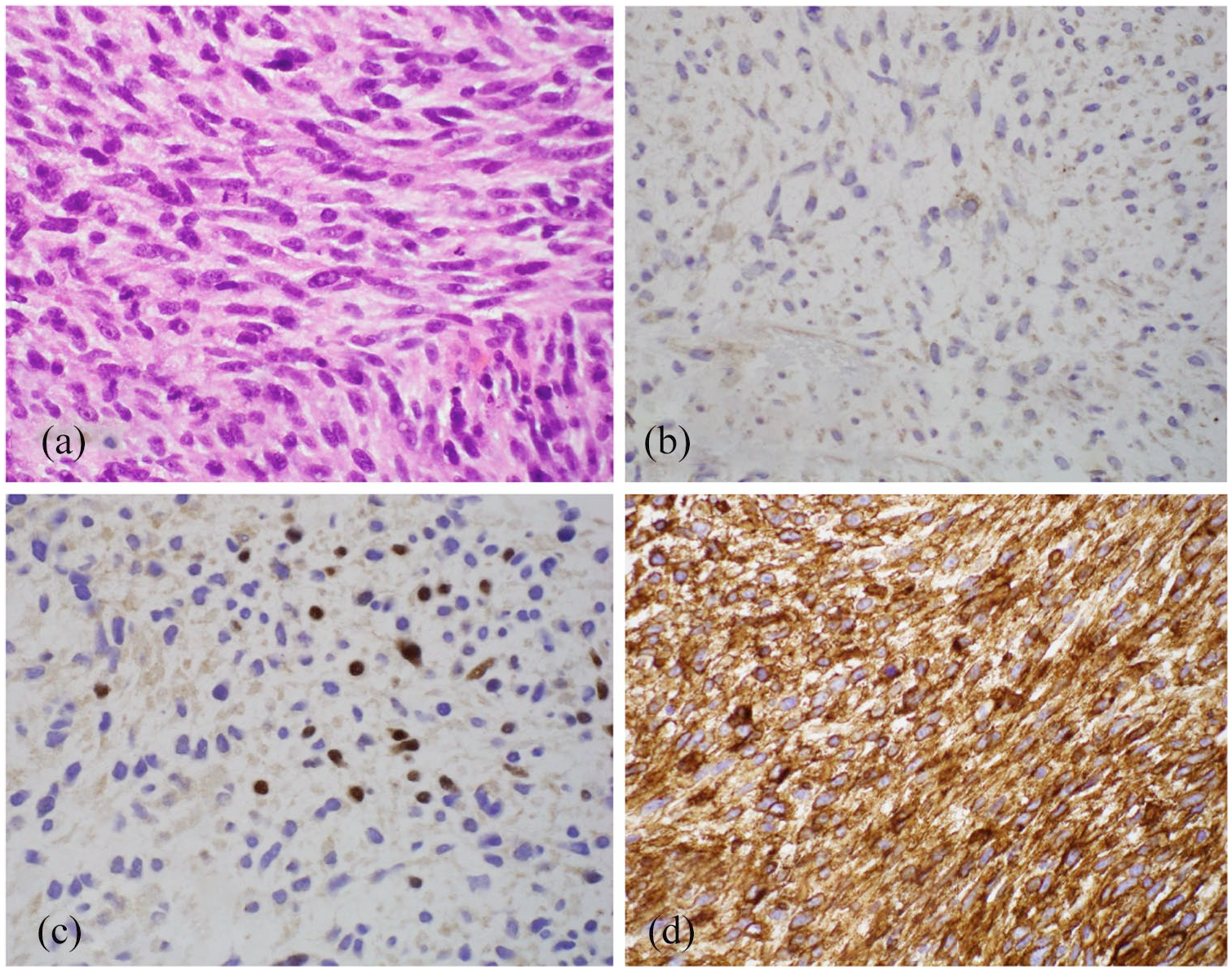
Immunohistochemistry of patient’s tumor: (a) H&E, (b) Cytokeratin 14, (c) P63, and (d) EGFR. 200×.
Staging CT scan noted a large right breast mass with associated skin thickening, consistent with the patient’s known breast neoplasm, and prominent subpectoral lymph nodes. The CT scan also revealed several hypoattenuating liver lesions, many of which appeared to be cystic consistent with simple cysts, with a few indeterminate smaller lesions. These have remained stable on follow up CT scans, the last being about 18 months since the initial study.
The patient received three cycles of neoadjuvant AIM between March 2018 and May 2018. Treatment was complicated by neutropenic fever of 38.5° with an absolute neutrophil count (ANC) of 0.09 after cycle 1. Post-treatment CT of the chest showed grossly stable appearance of the large right breast mass and did not indicate treatment effect. She underwent chest wall resection to include the right breast with immediate rotational flap reconstruction. The resected mass measured 16 × 14 × 12 cm with margins free of tumor. The tissue pathology showed malignant spindle cell neoplasm with marked therapy effect consisting of >99% necrosis with rare scattered tumor cells present (Figure 2).

Patient’s tumor after three cycles of neoadjuvant AIM and surgical resection. Rare viable tumor cell amid extensive necrosis. H&E. 200×.
She received two additional cycles of AIM and radiation therapy (50 Gy in 25 fractions and 6 Gy boost) as adjuvant therapy. Her adjuvant treatment course was complicated by G3 dermatitis, which limited her treatment to 6 Gy boost from the originally intended 10 Gy. Twenty-four months after initiation of her neoadjuvant AIM chemotherapy the patient is alive and well with no evidence of residual tumor or disease recurrence.
Discussion
Spindle cell carcinoma of the breast is a subtype of rare, and histologically heterogeneous breast neoplasms known as metaplastic carcinomas. Metaplastic carcinomas are morphologically heterogeneous and comprise low- and high-grade tumors. The current World Health Organization (WHO) classification system for these tumors includes low-grade adenosquamous carcinoma, fibromatosis-like metaplastic carcinoma, squamous cell carcinoma, spindle cell carcinoma, and carcinoma with mesenchymal differentiation. 1 With the exception of low-grade adenosquamous and fibromatosis-like variants, metaplastic carcinomas are typically aggressive, chemoresistant, and have a high propensity for metastasis.2,3 In one study, metaplastic carcinomas of the breast when compared to poorly differentiated ductal carcinomas had higher rates of developing metastatic disease (21.6% vs 18.1%), locoregional recurrence (5.4% vs 2.8%), and death from disease progression (29.7% vs 4.2%). 2
This case was unique in several respects. This patient had a malignant spindle cell neoplasm with the differential diagnosis including metaplastic carcinoma—spindle cell type, phyllodes tumors, and primary undifferentiated sarcoma of the breast. Phyllodes tumors are composed of connective tissue stroma and epithelial elements, with the most aggressive being malignant phyllodes tumors (MPH), which typically demonstrate stromal components exhibiting a sarcoma-like pattern. 4 However, the absence of glandular structures provided evidence against a phyllodes tumor. Primary breast sarcomas are rare, accounting for <5% of all soft tissue sarcomas and <1% of all breast malignancies.5,6,7 Primary breast sarcomas often present as a unilateral, painless, well-defined mass, such as our patient. Notably, they tend to be larger than epithelial breast cancers with rapid increase in size. Among the subsets of undifferentiated soft tissue sarcomas is the spindle cell variant, which our case resembled histologically. However, the weak cytokeratin expression of CK14 and P63 as seen in this case favored the diagnosis of metaplastic carcinoma—spindle cell type over spindle cell sarcoma. Weak keratin expression (CK14 and P63) has been observed previously in spindle cell carcinoma. 8,9
Ours is the first reported case of spindle cell carcinoma that was treated with AIM neoadjuvant therapy, a sarcoma based regimen. Due to the rarity of metaplastic breast cancer and the heterogeneity of disease presentation, a standardized approach is lacking. Instead, treatment is extrapolated from other types of breast cancer or metaplastic carcinomas of different locations.10,11,12 Treatment can be modeled from those of breast sarcoma, as there is some data suggesting that metaplastic tumors with predominantly sarcomatous appearance are likely to behave as sarcomas. 13 However, because primary breast sarcomas are also rare, the treatment is then extrapolated from soft tissue sarcomas of other locations (most often those of the extremity and chest wall). 5 Data on the use of neoadjuvant chemotherapy, either for sarcoma or for metaplastic carcinoma, is even more sparse and treatment decisions are made on a case-by-case basis. Because negative surgical margins in sarcoma are crucial for local control and increased survival, preoperative systemic treatment is considered for large or locally advanced sarcomas. 14 The preoperative treatment for these large and high-risk sarcomas is usually neoadjuvant chemotherapy (with or without radiation), usually with doxorubicin and an alkylator. The pathological complete response (pCR) after neoadjuvant therapy was described in several studies that utilized carcinoma-type chemotherapy in metaplastic breast cancer (with inclusion of a taxane) regimens, but most systemic treatment regimens were poorly described.15–17
In one study, 29 metaplastic breast carcinomas underwent neoadjuvant chemotherapy with an overall pathological complete response rate of 17% using mostly standard breast cancer agents such as doxorubicin, cyclophosphamide, and taxanes. 17 However, only one of these patients with a complete response was classified as having a pure spindle cell type carcinoma. Given the overall poor activity of standard breast regimens against this rare tumor type and the poorly described regimen in this study of metaplastic breast carcinomas, the decision was made to treat with a more traditional sarcoma regimen that would not exclude a backbone consisting of an alkylator and doxorubicin. Therefore, our choice of AIM therapy seemed to be the most appropriate for this rare tumor.
Current limited data regarding the efficacy of neoadjuvant regimens hint at the potential for additional research and improvements in how we treat metaplastic breast cancer. For example, in the retrospective analysis of patients treated with neoadjuvant chemotherapy with anthracyclines and taxanes, those with metaplastic breast cancer perform worse than those with triple negative breast cancer. Given this, there are increasing consideration for use of immunotherapies and targeted agents to optimize both pathologic complete response (pCR) and resection rates. 18
The post-treatment CT of the thorax had only showed stable disease of the breast after three cycles of chemotherapy and thus was not indicative of a treatment effect (Figure 3). Due to the large size of the mass, the whole mass could not be included in the field of imaging. However, based on the available images and as measured and shown on the images, the tumor did not change significantly in size. While dedicated breast imaging such as MRI with contrast could have better delineated areas of necrosis by evaluating for total tumor glycolysis, this was unfortunately not done. It was only after resection of tumor that the extensive treatment effect was observed. This discrepancy between Response Evaluation Criteria in Solid Tumors (RECIST) criteria and histopathologic response to neoadjuvant therapy has been described in sarcoma. 19 This may further suggest that metaplastic carcinoma—spindle cell type of the breast closely resembles the behavior of primary breast sarcoma, with excellent response to neoadjuvant therapy intended for sarcomas without radiological response. In our patient, the use of AIM chemotherapy was sufficient to cause almost complete necrosis of the tumor prior to resection. Presently, she remains disease free 2 years after her treatment.

CT Thorax of the patient, coronal and transverse view: (a) initial staging and (b) re-staging after three cycles of neoadjuvant AIM chemotherapy.
Conclusion
Metaplastic carcinoma—spindle cell type is a very rare tumor with little research on its management. The patient in this case had a large tumor spanning >15 cm and had to undergo three cycles of neoadjuvant AIM therapy. Although the neoadjuvant therapy was intended to shrink the tumor size, the CT imaging failed to show tumor shrinkage. It was only after tumor resection, that the exceptional response to chemotherapy was noted. Given our experience, the use of chemotherapy utilizing AIM could be considered for some patients presenting with spindle cell carcinoma of the breast.
Footnotes
Author Contributions
AC reviewed the patient information, researched literature, and wrote the manuscript. PMC and SC reviewed the pathologic information, made the diagnosis, and provided images for the manuscript. KML was involved in patient care during treatment period, and helped get informed consent. WWT was involved in patient care during treatment period, performed the resection of the tumor after neoadjuvant therapy. DBP reviewed the radiographic information and provided images for the manuscript. JH is the oncologist treating the patient; he reviewed the patient information, served as a mentor/advisor and helped put the paper together. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this article because this was an anonymous case report with consent for publication granted by the patient.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymous information to be published in this article.