
Abstract
The purpose of this study was to analyze the outcomes of extracranial GCT in children in a developing country and to assess prognostic factors. The data on 141 children (<18 years old) with extracranial GCT, confirmed histopathologically, collected over the past 9 years (from February 2013 to June 2022) were retrospectively studied. The patients underwent the same therapy with platinum-containing chemotherapy regimens. In the malignant GCT group, OS and EFS were 81.0 ± 4% and 73 ± 5%, respectively. OS and EFS in the teratoma group were 90 ± 5% and 85 ± 6%. In univariate analysis, parameters like stage of disease, tumor localization, AFP level ≥10,000 ng/mL, serum AFP kinetics and resection status were found to be statistically significant prognostic factors. In the multivariate analysis, the significant adverse factors were the resection status, initial AFP level ≥10,000 ng/mL and serum AFP kinetics slow down (p = .000). Good survival rates can be achieved in developing countries with adequate compliance with treatment protocols. The analysis demonstrates high efficacy of platinum-containing chemotherapy regimens. In our opinion, the protocol used in high-income countries can be implemented in low-income countries with the financial support from the government. The qualification of specialists is also important.
Introduction
Germ cell tumors (GCT) are a curable oncological pathology with the survival rate that has considerably improved and is now up to 90%.1–4 This group of heterogeneous neoplasms is unique in that their developmental potential is, in influence, determined by the latent potency state of their cells of origin, which are reprogrammed to totipotent or pluripotent stem cells. Oosterhuis and Looijenga in 2019 proposed a new broad classification of GCT according to their development potential. The classification considers seven types of GCT, each of which has different epidemiological and epigenomic features. Among them, two types are typical for children, type 0 and type I, and four for adults – types II–V. Type 0 tumors are characterized by parasitic twins which are almost always monozygotic, as a rule, fused in the abdomen, sacral region and retroperitoneum. They are diagnosed prenatally or at birth, consist of a yolk sac tumor and a malignant neoplasm of the somatic type. Type I tumors occur in newborns and infants under the age of 6 years and mainly consist of teratomas and yolk sac tumors. Type II tumors include both non-seminoma and seminoma ones and affect the population of adolescents and young adults. Type III tumors, which are represented by spermatocytic seminoma, occur in men over 40 years of age. Benign teratomas are classified as type IV tumors; they occur at reproductive age. While type V of the tumor consists of a complete cystic drift (a benign form of gestational trophoblastic disease), VI type occurs in people of over 60 years of age and resembles type 1 localized in atypical areas, such as soft tissues of the extremities.5,6
Mature and immature teratomas are almost always benign, regardless of localization. The prognosis may be unfavorable if they are not completely removed.5,7 However, in cases of even complete resection, there is a risk of recurrence in the form of a pure teratoma or with a malignant component, progression into yolk sac tumor.5,7–10 Immature teratomas also have the potential for malignant transformation and metastasis. 11 The main type of therapy is surgical treatment, in which complete resection plays an important role. Treatment of malignant variants of GCT involves not only surgery but also chemotherapy.
It is difficult to determine the true incidence of all GCT, as benign GCTs are not registered in the cancer database. Only according to the MAKEI protocol, patients with teratomas have been included in the register since 1983, and teratomas have been studied together with malignant types of GCTs. In children of under 15 years, the incidence of GCT is 3%, and it is considered a rare type of childhood cancer along with childhood rhabdomyosarcomas, osteosarcomas or retinoblastomas. 12 However, in adolescents aged 15–19 years, malignant GCTs were 14% of all neoplasms, 13 becoming the most common solid tumor and the second most common malignant neoplasm in this age group after Hodgkin’s lymphoma. 14
In 2013, our country approved a clinical protocol for the diagnosis and treatment of extracranial GCTs based on the MAKEI protocol developed by the German group of pediatric oncologists/hematologists (PE, PEI regimens).
The aim of this study was to assess the results of treatment and prognostic factors in patients with extracranial GCTs.
Patients and methods
Characteristics of patients
The analysis included 141 children with extracranial GCTs treated at the Scientific Center of Pediatrics and Pediatric Surgery in Almaty, Kazakhstan between February 2013 and June 2022. There are 2 centers that provide medical care to children with cancer in our country, and our center cares for patients from the southwestern regions of the country.
All the patients underwent a comprehensive examination, including diagnostic imaging (CT/MRI and sonography) and were tested for serum cancer markers (alpha-fetoprotein, human chorionic gonadotropin, lactate dehydrogenase). The first stage determined the possibility of the radical removal of the tumor. The necessity of chemotherapy was determined after the histological and immunohistochemical verification of the diagnosis. If tumor resection was not possible at the time of the diagnosis, resectability was re-evaluated after neoadjuvant chemotherapy. Subsequently, therapeutically induced changes were evaluated and adjuvant chemotherapy was performed. Patients with teratomas received surgical treatment only. In cases of tumor prevalence, impossibility of radical surgery and high levels of serum cancer markers, chemotherapy was prescribed as the first stage.
The tactics of “watch and wait” was selected for patients from the low-risk group after the operation. Patients at intermediate risk were assigned 2 courses of chemotherapy according to the PE and PEI regimens, depending on the status of resection. High-risk patients underwent 4 courses of chemotherapy, according to the PEI regimen.
Serum AFP kinetics was studied according to the nomogram proposed by N.D.Faseeva in 2018. 16 This nomogram was based on the half-elimination period and the predicted time of AFP level normalization. So, with the AFP level of 10,000 ng/mL at the onset, the values of M1 should be less than 80 ng/mL (blue line), with AFP equal to 500 ng/mL, M1 should be <15 ng/mL (green line).
Methods of statistical processing
Overall Survival (OS) and Event-Free Survival (EFS) were used as indicators to evaluate therapy outcomes according to the Kaplan-Mayer method. The onset of relapse, progression, and death from complications of treatment were taken as events. The statistical significance of differences in survival was calculated using the log-rank test. The differences were considered as significant at p < 0.05. Statistical analysis was carried out using SPSS Statistics 13.0 for Windows (SPSS, Inc, Chicago, IL., USA). The permission of the Institutional Review Board was obtained for the study (protocol No. 3 (80) from 27.02.2019). During data processing, all the information about patients was depersonalized.
Results
Patient characteristics
Characteristics of patients depending on the histological type and localization of the tumor.

Teratomas were morphologically verified in 45 patients (31.9%) and malignant GCTs in 96 patients (68.1%). 27 teratoma cases were mature teratomas, 15 were immature teratoma and in 3 cases there were immature teratomas with a malignant somatic component (microfocal area of neuroblastoma, squamous cell carcinoma, PNET).
In our study, there were no events in the mature teratoma group, but 6 (33.3%) out of 18 patients with immature teratomas experienced events, and a fatal outcome occurred in 4 patients. In all the cases, the tumors were located in the sacrococcygeal region and AFP levels were within the normal range for age. One child had a teratoma with a component of a malignant somatic tumor which was removed at the age of 1 month. After 6 months, a relapse occurred in the pelvis. Chemotherapy was prescribed, but the parents refused treatment and the patient subsequently died. The second patient with immature teratoma, G3, was operated radically at the age of 2 years 11 months. There was a relapse with the addition of a yolk sac tumor component, a lesion of the retroperitoneal space and multiple pulmonary metastases after 15 months. After 1 course of chemotherapy, the parents refused to continue treatment and the patient died. The third patient with immature teratoma, G2, was operated at the age of 2 years 6 months and the tumor was completely removed. After 13 months, a relapse occurred in the pelvis. Unfortunately, 4 courses of PEI chemotherapy were ineffective and the patient died due to the disease progression. The fourth patient with immature teratoma, G1, was operated at the age of 2 months, but the tumor was not removed completely. The level of AFP was within the reference range. In the postoperative period, a slow increase of serum AFP was detected. After 2 months, a continued growth of the residual tumor was diagnosed, followed by a sharp increase in the AFP levels and generalization of the process. The patient received 4 courses of PEI and 2 courses of PEB but showed no improvement and later died from the progression of the disease. The fifth patient with immature teratoma, G2, was operated at the age of 11 days. A relapse occurred after 13 months, with an increase in AFP levels. He received PEI chemotherapy, and a complete response was achieved; then, the patient was observed for 25 months without any signs of the disease. The sixth patient with immature teratoma, G2, had multiple pulmonary metastases and infiltration in the rectum. The tumor was completely resected and the patient received PEI chemotherapy №4. The number and size of pulmonary metastases decreased, but after 10 months, a continued growth of metastases in the lungs was diagnosed. The second line of therapy was administered according to TIP regimen №4 and helped stop further metastasizing. The patient is alive, and has been under observation for 10 months.
It can be seen that teratomas, in particular immature teratomas, despite their benign nature, exhibit an aggressive course and can be fatal for certain patients. In our study, the number of patients with immature teratoma and the number of events that occurred were higher. Radical surgery was considered to be the main treatment for these tumors. In one case, we applied chemotherapy to a stage 4 patient immediately after surgery and managed to stabilize the pulmonary metastases and prolong the life of the child. In other cases, chemotherapy was used to deal with relapses, continued growth of residual tumors and increased AFP levels. But, in our opinion, it is difficult to judge the effectiveness of chemotherapy in case of events, as some parents (2 out of 5) refused treatment, 2 patients did not respond to the therapy and only 1 patient had a positive effect.
There were 12 seminomatous GCTs verified (11 of them dysgerminomas, 1 with seminoma) and 84 non-seminomatous GCTs, out of which 41 cases were yolk sac tumors, 12 cases were mixed malignant GCTs, 2 cases were embryonal carcinomas and 15 cases were teratomas + yolk sac tumors. In 14 cases the histological type of the tumor was not established, since therapeutically induced grade IV pathomorphosis was achieved after neoadjuvant chemotherapy, although the AFP levels were high initially.
Cytogenetic examination revealed Klinefelter syndrome in a teenage boy with mediastinal GCT, Swyer syndrome in a teenage girl.
The 5-years OS rate of the patients was 84 ± 3%, EFS was 79 ± 4%. Fatal outcome occurred in 20 patients, and events were observed in 28 patients.
OS and EFS in the teratoma group were 90 ± 5% and 85 ± 6%, respectively. Events occurred in 6 patients with sacrococcygeal teratomas. All the patients had concentration of AFP and HCG was normal.
OS and EFS in the malignant types group were 81 ± 4% and 73 ± 5% (p = .141), respectively.
Fatal outcome occurred in 4 patients with teratomas and in 16 patients with malignant GCT.
To identify prognostic factors, teratomas were excluded from further analysis due to their benign nature.
Characteristics of patients with malignant types of GCT.
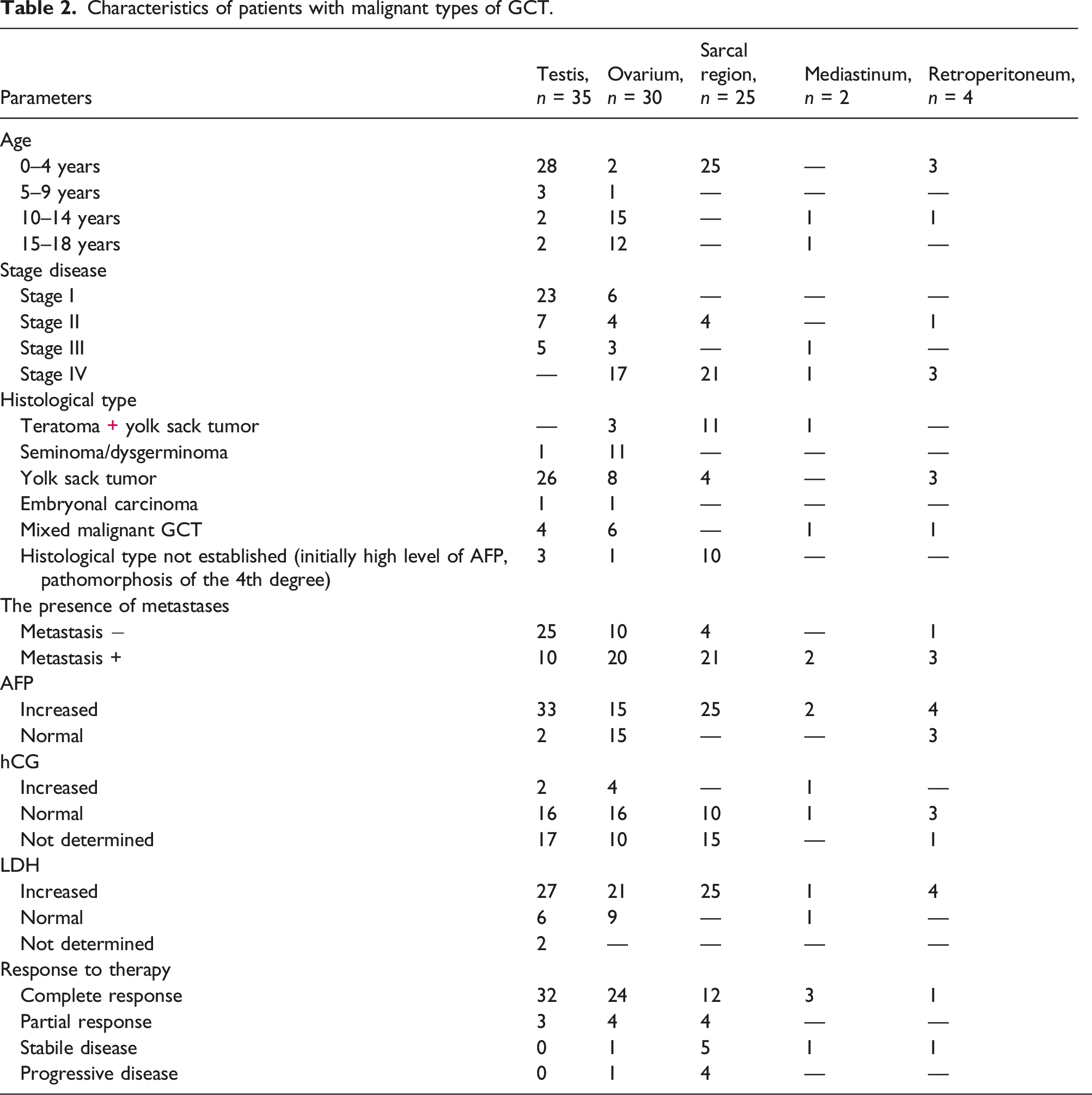
The average age of patients was 5 years 9 months (95% CI: 4.6–7.1), median 2.0, interquartile interval 12.
The number of male and female patients was almost equal, 47:49. The average age of male patients was 4 years 2 months (95% CI: 2.6–5.8), median 1.0, interquartile range 5. The average age of female patients was 7 years 5 months (95%CI: 5.7–9.3), median 8.0, interquartile range 13.
Fifty eight children (60.4%) were under the age of 4 years, 4 children (4.2%) were aged 5–9 years, 19 patients (19.8%) were 10–14 years old and 15 patients (15.6%) were aged 15–18 years. The first peak of morbidity occurred at the age of 5 years, the second peak at adolescence.
Univariate analysis
Parameters recommended by MaGIC were used to investigate the prognostic factors. 16
In 65 cases (67.7%), the tumor was localized in the gonads: in 30 patients (31.2%) the ovaries were affected, in 35 cases (36.5%) the testicles. In 31 patients (32.3%) extra-gonadal sites were affected: the sacrococcygeal region in 25 patients (26.0%), the mediastinum in 2 patients (2.1%), the retroperitoneum in 4 patients (4.2%). EFS in the gonadal tumor group was 85 ± 6%, and in the extragonadal tumor group it was 46 ± 10% (p < .001) (Figure 1). EFS depending on tumor localization (gonadal/extragonadal).
Based on the EFS analysis for each tumor location, the lowest survival rate was observed in patients with mediastinal and sacrococcygeal GCTs. 84% of cases (21 patients) with sacrococcygeal GCTs had internal tumors (types 3-4) according to the Altman classification (Figure 2) Altman/AAR classification: four surgical subtypes of tumors depending on the relative proportion of internal and external components of the tumor.
Patients with retroperitoneal and testicular GCTs had the best survival rates (p < .001).
In the group of patients younger than 11 years, EFS was 70 ± 7%, in the group older than 11 years it was 80 ± 8% (p = .341).
The stage of the disease was determined according to the FIGO classification for ovarian, Lugano for testicular, and TNM for extragonadal tumors. Localized disease (stages I-II) was detected in 46.8% of cases (45 patients), advanced disease (stages III-IV) in 53.2% (51 patients).
EFS in localized disease was 84 ± 7%, in advanced disease 63 ± 7% (p = .014), respectively.
Metastases were detected in 58.3% (56 patients). EFS in the group of patients without metastases was 82 ± 8%, whereas in patients with metastases it was 66.1 ± 7% (p = .061).
EFS were analyzed depending on the type of metastases. 29 patients had pulmonary metastases and their EFS was 63 ± 9.0%. In patients without pulmonary metastases EFS was 71 ± 9%. 12 patients had visceral metastases (p = .505), EFS in the group of patients with the presence of visceral metastases was 25± 21%, without visceral metastases - 71 ± 7% (p = .070).
When analyzed by morphological type, EFS in seminomatosus GCT group was 81 ± 12% and in non-seminomatosus GCT group it was 71 ± 6% (p = .643).
AFP was elevated in 79 patients (82.30%). EFS in the group of patients with normal AFP (0-10 ng/ml) was 87.4 ± 8.4%, while in the group with AFP 11-9999 ng/ml was 74.5 ± 8.4%, with AFP over 10,000 ng/mL EFS was 64.4 ± 8.4% (p = .021), respectively.
Serum AFP kinetics was studied according to the nomogram proposed by N.D.Faseeva in 2018
15
(Figure 3). In 45 patients (56.9%) AFP levels reduction on day 42 was higher than the proposed threshold, i,e, above the red line. EFS made up 57 ± 8% versus 88 ± 6% in the group with AFP levels below the threshold line (p < .001). Nomogram for diagnosing prolonged half-elimination and predicting AFP normalization time in patients with GCT.
15

For technical reasons due to impossibility of making the tests, hCG was measured only in 55.2% (53 patients). It was elevated in 7 patients. EFS in the group with elevated HCG levels was 81 ± 7% and 86 ± 13.0% in the group with normal HCG, respectively (p = .869).
LDH was increased in 81.2% (78 patients), in 2 patients it was not defined. EFS in the group with a normal LDH was 70 ± 21.0% (95% CI: 68.2%–102.7%), with a high LDH level it was 71 ± 6.0% (p = .241).
In terms of the extent of operation, complete resection was achieved in 63.5% of cases. Incomplete resection was most often made in patients with tumors in the sacrococcygeal region and ovary. EFS was 91.2 ± 3.8% in the complete resection group (R0), 42,5 ± 10,8% in the group with microscopic residual tumors (R1) and 33,3 ± 27,2% in the group with macroscopic residual tumors (R2) (p < .001) (Figure 4). EFS depending on the resection status.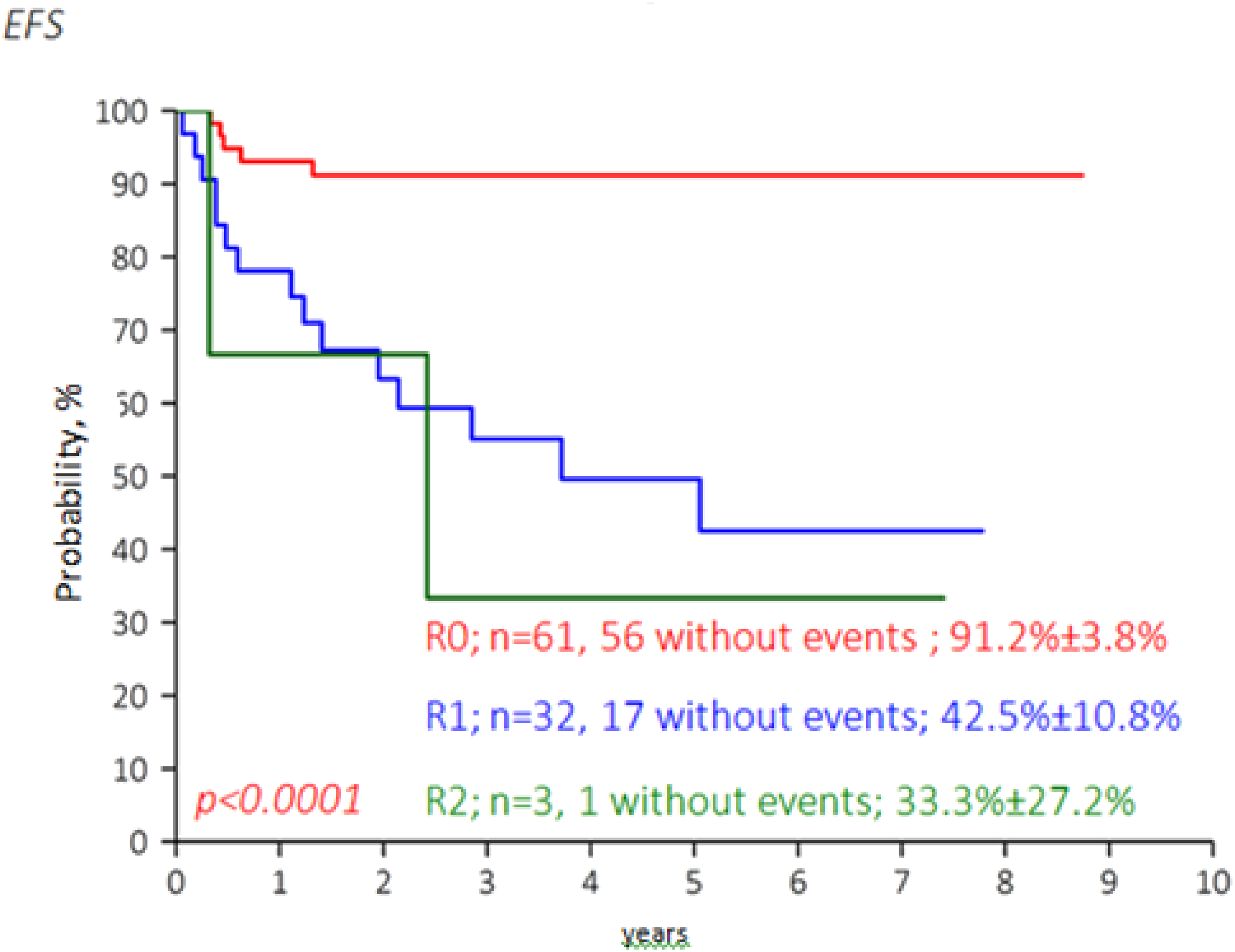
Multivariate analysis
In multivariate analysis, resection status, initial AFP level ≥ 10,000 ng/ml and serum AFP kinetics slow down (p = .000) were found to be significant factors. In patients with complete resection status the probability of occurrence of the event is 9.1 times lower than in patients with microscopic residual tumor, and 15.8 times lower than in patients with macroscopic residual tumor. In patients with an initial AFP level of more than 10,000 ng/ml, the risk of an adverse outcome is 3.9 times higher compared to the group with an AFP level of less than 10,000 ng/ml. Patients with delayed AFP kinetics are 3.2 times more likely to have an event compared to the group with a normal decrease in AFP levels.
Discussion
Before the development of multimodal therapy, treatment of children with malignant GCT was largely inefficient.16–18 The main breakthrough occurred in 1977 when H. L. Einhorn, D. Donohue used the cisplatin, vinblastine and bleomycin (PVB) regimen obtaining a 100% response and 64% survival rate in men with disseminated testicular GCT. 19 Through the use of platinum-containing regimens, polychemotherapy made it possible to achieve a 5-years survival rate in about 90% of children with extracranial GCTs.1–4 Today the choice of treatment is based on histological verification of the diagnosis, diagnostic imaging data and classical cancer markers.
In our study, the 5-years OS rate in patients was 84 ± 3% and EFS was 79 ± 4%. OS and EFS in the teratoma group were 90 ± 5% and 85 ± 5%, respectively. According to the Italian group of pediatric oncologists, OS and EFS in the teratoma group were 98.6% and 90.6%, respectively. 8 In their study, events occurred in 4.6% of cases in patients with mature teratomas and in 13% of cases with immature teratomas. The majority of patients were diagnosed with sacrococcygeal teratomas. Patients with incomplete surgery for immature teratomas were the group with the highest risk of relapse.
OS and EFS in the malignant GCT group were 81 ± 4% and 73 ± 5%, respectively. The analysis confirms the high efficiency of platinum-containing chemotherapy. The outcome of extracranial GCT in this study seemed to be favorable but still inferior to that of developed countries, where OS and EFS are above 95 and 90%, respectively. 20 Our survival rates are closer to recorded in developing countries.21–23
In our country, until 2013, children with oncological diseases, including GCT, were treated in the department of pediatric oncology at the adult oncological hospital and regional children’s hospitals, where there were not always the right specialists. Patients were mostly admitted with advanced stages of the disease. There were no standards treatment protocols, not always necessary drugs were available for use. The OS rate of patients with malignant GCTS was 68%.
Since 2013, a restructuring of the pediatric oncology service has been performing. All children with oncological diseases are treated in two republican multidisciplinary centers, a single clinical protocol for the treatment of GCT has been approved. Training courses on early diagnosis of malignant neoplasms are held in the regions regularly. As a result of the restructuring, we see positive dynamics in early diagnosis as well as efficiency of therapy.
In our univariate analysis, statistically significant prognostic factors were: advanced stage (p = .014), extragonadal localization (p < .001), AFP ≥10,00 ng/mL (p = .021), kinetics of serum AFP (p < .001) and resection status (p < .001).
At stage I, EFS was 90 ± 9%, at stage IV it was 58 ± 8% (p = .006).
The lowest EFS was found in patients with mediastinal and sacrococcygeal GCTs (p < .049). It should be noted that in 84% of cases, a tumor of the sacrococcygeal region with an internal component precluded surgical treatment at the first stage and subsequently there were difficulties in removing it after courses of chemotherapy. A recent meta-analysis showed that EFS in patients with sacrococcygeal GCTs ranges from 27 to 87%. 8 According to our data, EFS in this group of patients was below 40% due to the predominance of the internal variant of the tumor location and the incomplete resection.
Analysis of EFS by the morphological type of GCT did not produce statistically significant results due to the small number of patients with seminomas (p = .643).
The toxicity of chemotherapy manifested in 1 patient with a stage 4 malignant ovarian GCT after 1 course of chemotherapy and was followed by aplasia and renal failure.
In the multivariate analysis, resection status, initial AFP level ≥ 10,000 ng/ml and serum AFP kinetics slow down were found to be adverse factors. The volume of surgical intervention played a significant role in the outcome of therapy. As previously reported by researchers, marker kinetics during the first 6 weeks of chemotherapy provides important prognostic information and can be used for designing risk stratification classifications in combination with other risk factors.24,25
There were some limitations in this study that need to be mentioned. First, as it is common in retrospective studies, some data might be missed or incompleted. Second, the sample size in this cohort appears to be small; so some significant prognostic factors might be not salient.
Conclusion
The study aimed to evaluate the results of treatment of GCTs in children in developing countries and verify that good survival rates can be achieved in developing countries with adequate compliance with the protocol requirements. The analysis demonstrates high efficacy of platinum-containing chemotherapy regimens. In our opinion, the protocol used in high-income countries can be implemented in low-income countries with the financial support from the government. The restructuring of the pediatric oncology service together with the implementation of a single protocol treatment and the improvement of early diagnosis undoubtedly contributed to improving the survival rates of children with GCT in our country. The findings of this study may be useful for clinicians in other LMICs, for treatment children with this kind of cancer.
Footnotes
Acknowledgements
The authors gratefully acknowledge and thank other colleagues for their help in identifying all of the germ cell tumors that we report herein. Without their help, we would not have been able to complete this work: Olesya Pankova, Assel Muratova, Konstantin Khairov, Anna Machneva, Aigul Bekisheva.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded under scientific and technical program №. BR11065390 «Design and development of innovative technologies for early diagnostics and treatment of malignant diseases, taking into account modern approaches of genomics» (Targeted Financing from the Ministry of Healthcare of the Republic of Kazakhstan).
Ethical statement
Trial registration
Kazakhstan.
Contributorship
Symbat Saliyeva, Gaukhar Nurzhanova, Bakhram Zhumadullayev contributed to conception, data collection and analysis, and writing of the manuscript. Symbat Saliyeva, Riza Boranbayeva, Minira Bulegenova, Lyazat Manzhuova contributed to critical review of the manuscript. Symbat Saliyeva contributed to statistical analysis.