
Abstract
Introduction
Li-Fraumeni syndrome (LFS) is a rare autosomal dominant hereditary cancer syndrome caused by mutations in the TP53 tumour suppressor gene on chromosome 17. 1 Various types of cancers such as sarcomas, premenopausal breast cancer, brain cancer, adrenocortical carcinomas, and leukaemia are seen in LFS. 2 Many other cancer types such as cancers of the colon, pancreas, stomach, kidney, endometrium, ovary, prostate, lung, and skin may also be found associated with LFS. 3 Families affected with LFS reportedly have a high inherited risk of developing a wide range of cancer across several generations. The incidence of cancers in LFS begins in early childhood and then peaks before the age of 30 years 1 The classic LFS is diagnosed when a person has all of the following criteria i.e., a sarcoma diagnosed before age 45, a first-degree relative, meaning a parent, sibling or child, with any cancer before age 45 and a first-degree relative or second-degree relative, meaning a grandparent, aunt/uncle, niece/nephew, or grandchild, with any cancer before age 45 or a sarcoma at any age. The Chompret criteria for clinical diagnosis of LFS are proposed recently to identify affected families beyond the Classic criteria. 4
Generally, an individual with suspected or diagnosed LFS, in his thirties has a 50% risk of developing cancer, and further this risk increases to 100% by the age of 70 years1,5 Due to the high risk of occurrence of multiple cancers, patients with LFS may have overbearing psychosocial problems.6,7 Some of these individuals might have lost a parent or any close relative, which could intensify their emotional distress. 8 We planned to interview them “face to face” using an interview schedule to explore their social impact related to LFS and how their lives are affected following the diagnosis in terms of their physical functioning, emotions, communication, self-esteem, and coping strategies.
Methods
A constructivist grounded theory approach was used to interview the families with at least one member having confirmed diagnosis of LFS. Individuals more than 18 years of age, having germline TP53 mutation or the caregiver of the confirmed patient, understanding Hindi or English and willing to participate in the study were eligible for this study. Data was collected using an in-depth interview with participants at Sarcoma clinic in the medical oncology department. The subjects were the individuals with LFS or the caregivers attending the outdoor patient department of the hospital. The data collection period was 4 months after the ethical approval of the institutional ethical committee. Written informed consent was obtained after assuring confidentiality and anonymity. A total of seven members belonging to families diagnosed with LFS were contacted in the study; of which one person refused to participate in the study. The purpose of the study was explained to the subjects and written informed consent was obtained from the subjects after ensuring confidentiality and anonymity.
Data was collected from August 2021 to November 2021. Data analysis was done along with the ongoing data collection, which helped to further shape the interview schedule and the subsequent data collection procedure. All interview recordings were transcribed verbatim. This required checking through each transcript against the taped recordings to ensure the accuracy of the content and that the translation of terms and/or words were consistently used throughout. The raw data were read several times to identify the emerging themes, which were grouped into categories independently developed by two researchers (PJ and SB). Themes were generated from the transcribed verbatims. Responses relevant to each category were examined and analyzed. The identified themes were compared and agreed upon by all the researchers for the common coding and categorization.
Results
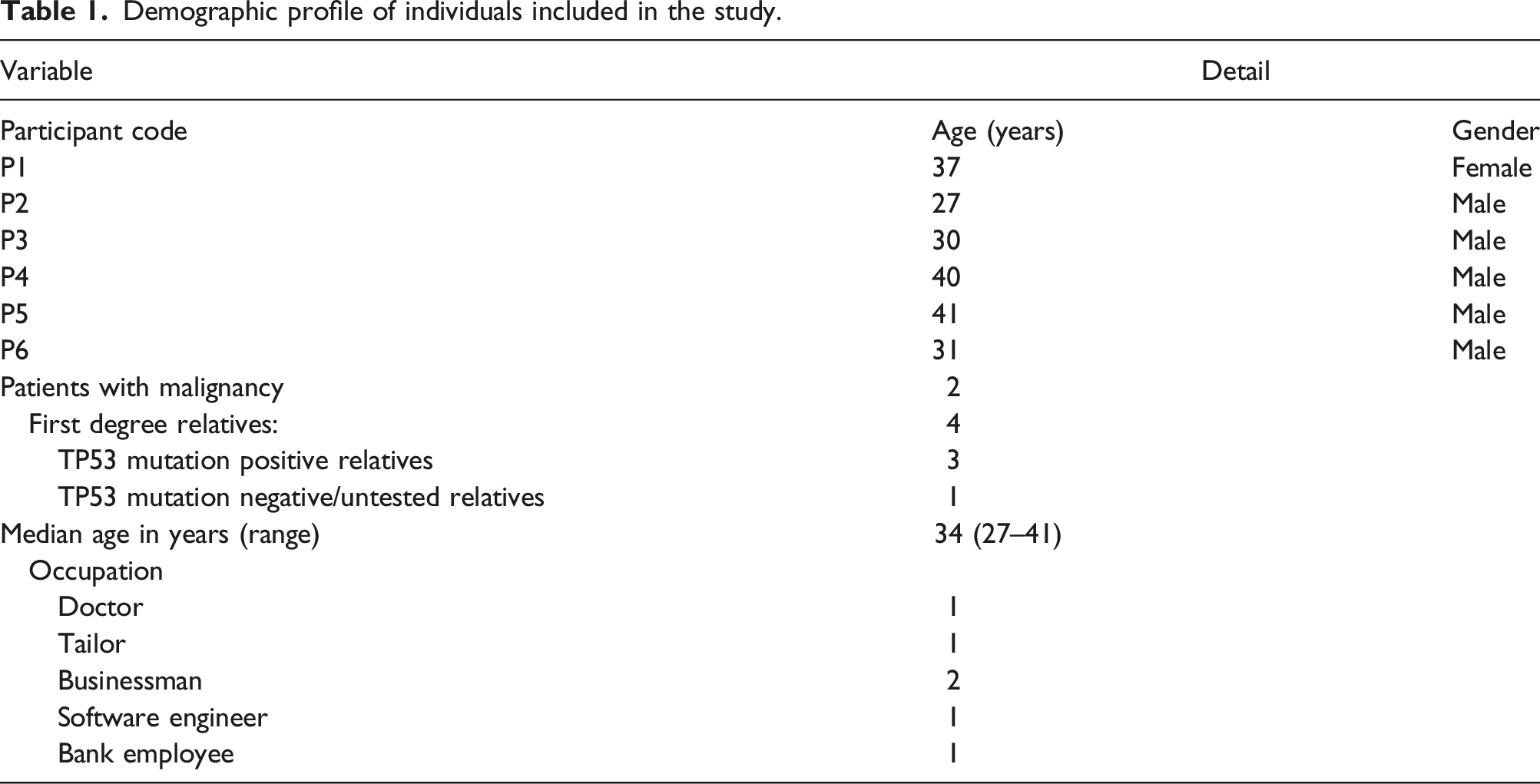
Demographic profile of individuals included in the study.
Summary of the themes and sub-themes of psychological issues encountered in the study.

Theme 1: Stressors
Sub-theme - The added burden of cancer in the family
Being diagnosed with LFS and taking care of a family member with the same disease is equally binding as it is a tumultuous task in the face of a new challenge. “I already have a cancer patient at home, then when it came to know that it's a familial kind of thing and there is a risk of other family members also getting a malignancy, that's something very troubling.” (P1) “The main concern was how to share this with other family members as my mother is already undergoing treatment.” (P3)
Sub-theme - Fear of rejection
Owing to the rarity of the disease and the misconceptions associated with it, participants reported the fear of rejection from their acquaintances. This adds to preconceived self-stigma. “Not really. I don’t discuss it with anyone. Neighbours suspect that something is wrong with the family.” (P2)
Sub-theme - The anxiety of disclosing results
The reaction of loved ones and fear of discussing the intensity of the illness further provoked anxiety in participants before disclosing the results to family members. Some of the families chose not to hold an open discussion because of avoiding an increase in the psychological burden of the affected. “We do not discuss it openly in the family. I fear, I do not know, how to discuss this with my family.” (P2) “The main shock was how to disclose the results to my family. That was my main concern.” (P3) “My wife does not know anything about it. I have not discussed this with my wife”. (P4)
Sub-theme - Anticipatory fear of being a possible carrier
Young adult participants chose not to get married or have children as they were fearful of passing on the genes to their offspring and hence continuing the cycle of grief and loss. “I am absolutely worried about being a possible carrier for my future generation and I am conscious of it.” (P3) “I don't have any plans of having children in the future. I have even told my wife to leave me if she wants.” (P3)
Sub-theme - Changes in activities of daily living
Normal routine life for the affected individuals has been scarred with the onset of the disease. The illness experience in itself demanded a lot of learning news and forgetting old things like paying regular visits to the physician and restricting some hobbies at the same time. “Already we are into this, we have to take a break from work, we have to go for a scan, we have to go for treatment.” (P1) “We could not sleep and did not eat well for many days.” (P2) “I like to play basketball; I am not playing this game now a day as it required more stretching of the arms.” (P3) “She has a suction pipe in her neck these days so we have to take extra care of her because of that suction pipe.” (P5) “I have less than adequate sleep than earlier. My mother is 66, and a homemaker. She is also having headaches, seeking help, she has all age-related issues and then I think there is a lot of tax on her…I need to be 100% to be able to give 100%.” (P6)
Sub-theme - Financial burden
Regular physician consultations, treatment and follow-ups make up for the major chunk of household costs leading one of the participants into the debt cycle and forcing the other to leave his job. “If you do your work only then we will be able to do all the other work. We have been taking debts and repaying them. Somehow, we are managing. God gives us one solution or the other. Sometimes, if I get some good work, I can earn a good amount of money. If I do not get any work to do, I will be back to square one.” (P5) “When I moved to India, I came up with the idea to take care of my family and will start my own work. I could not start. It is the worst two years for me. Once things get better, my workflow will start.” (P6)
Theme 2: Psychological reactions
Sub-theme - Hopelessness and helplessness
“When we came to know about this, we were a family then. So there is no use in thinking about these now.” (P1) “When my cancer triggered for the second time and third time, I felt a bit helpless as it reoccurred in less than a year even after receiving radiation and surgeries. It was a bit demoralizing”. (P3) “I wanted to see my child having relief. My son was asking us to kill him. How will parents feel, when the child asks parents to kill him?” (P4) “Nothing is going to happen ultimately. You know that and I know that too. There is no solution for this illness.” (P5) “Yesterday I was in the Max emergency, then went to Apollo. They told me no further higher doses can be given. At that time, I felt helpless… I have learnt to speak to my mother and siblings. Sometimes, I do not have the answer to their queries. At times, I feel very low while handling my family.” (P6)
Sub-theme - Denial
“I met the doctor. He told me about the disease probably being transmitted genetically. But we did not take it seriously.” (P2) “Initially, I had doubts since I was not symptomatic. I went for the re-checking of the biopsy sample”. (P3) “Who believes it? Parents do not believe it. They just pray to God day and night that no matter how but the child should be cured…I got the report checked two or three times.” (P5)
Sub-theme - Shock
“Everything was affected. The entire world was shattered. Everyone was affected in the family.” (P2) “I got the report through the mail. It was a shock for me, felt shattered at that time.” (P3) “I was shocked to know about cancer at that time.” (P4)
Sub-theme - Feeling victimized
“Yes, I felt it. But I know I cannot blame anyone for the present situation. How can I blame my mother? She, herself also suffered so much.” (P2) “What did I do? Why I am running so much? I did not do any harm to anyone. Why it is happening to me?” (P4)
Sub-theme - Anger
“I get aggressive sometimes. I should learn to live and control my emotions… I get aggressive, but I am trying to improve my behaviour.” (P6)
Sub-theme - Anxiety
“The result came around 1 PM. Since afternoon, I was anxious about what would be the report.” (P3) “When I was in Canada, I had severe anxiety. I was on medication. The anxiety was there because I was not here (with my parents).” (P6)
Sub-theme - Guilt
“The day I got to know about my child’s illness, I was a little upset.” (P4) “They live in Delhi. I have been away from Delhi for about 11 years. I have come back to India to take care of my ailing father. I feel guilty, I do not give them time.” (P6)
Sub-theme - Uncertainty about life and future
“The worry is about the treatment, the prognosis and the future. If there is a person with malignancies in the family, it is the uncertainty of the things which worries me.” (P1) “I am fearful and concerned about my family and its future.” (P2) “No…. but there is some uncertainty… it is a terminal illness.” (P3) “I do not know what his destiny is, or what God has planned for him.” (P4)
Theme 3: Behavioural responses
Unpleasant psychological experiences bring about a major shift in the individual’s behaviour. The concern for one’s health increases while simultaneously trying to access the best possible care.
Sub-theme - Social withdrawal
“I go less out... and I am less active in society. I am very pained all these months.” (P2) “And I did not let anybody show sympathy for me as well. Some people show sympathy. I closed that matter as well.” (P5) “I want to be by myself.” (P6)
Sub-theme - Increased concern about health
“I prefer home-cooked food. I avoid food from the restaurant.” (P3) “A little bit of change that I did was that we reduced the burden of her studies on her. Health first and everything else later.” (P5)
Sub-theme - Hiding information from affected
“My brother does not know much about the disease. He just knows that he is positive. He does not know much more than that. The meaning of positive he does not know very clearly.” (P2)
Sub-theme - Preparing family members for future
“I have to get my sister settled. I don’t know, whether my sister will be married or not. I am scared to talk to people around me.” (P2) “I want somebody who can speak to my mother to help her…I am preparing my mother for the worst now.” (P6)
Sub-theme - Striving for the best possible care
“I did not waste my time. It was 2 days before Diwali and got him operated on in December… I want to do as much as possible for him”. (P4) “To be honest my bandwidth 100% is with my family. Of course, I need to work, but do not think about it right now. He (my father) is not good. Yesterday was a very bad day for him. This is the end-of-life care for him. His health is going down day by day. He is currently bedridden and is on 100 mg of Morphine. He has issues... The idea is to reduce his suffering... (was trying to control his emotions).” (P6)
Theme 4: Coping strategies
Sub-theme - Emotional suppression
“You can say that I have been successful in controlling these thoughts.” (P1) “I felt tensed always. Even today, I don't feel normal and do not enjoy my life.” (P2) “I do not want to go into depression by knowing all about it (disease)… I have stopped thinking about it altogether. From the time I stopped thinking about it, the condition of my home has improved a lot.” (P5) “I am not thinking about it. It is said, I will cross the bridge when it comes to… The fact is that currently there is no room to currently hold the emotions. If I collapse, my mother will collapse.” (P6)
Sub-theme - Avoidance
“I do not know how much he knows about the disease. We don’t discuss it much in the family.” (P2)
Sub-theme - External support
Friends
“I followed my normal routine and just shared my feelings with my friends.” (P3) “My friend at that time supported me and asked me what are you thinking. Whatever happened, it happened. Look forward, look for the solution. My friends advised me not to think too much about it, but to get myself treated. My friends are always with me.” (P4) “My friend circle is good. They are all very helpful. Whenever I start falling, they support me.” (P5) “I meet my friends. I try to keep my mind away so that I give my 100% to somebody else. It helps me in coping up.” (P6)
Family members
“She (my wife) only encourages me to be more cautious about my health and seek proper treatment.” (P3) “My family (referring to extended family) is with me and always supports me.” (P4) “It is because of her (wife's) support that the mental pressure is not there. My burden regarding the household has also been reduced in the way that she is looking after everything.” (P5) “We are supporting each other. Me and my mother.” (P6)
Sub-theme - Faith in god
“If God wants her to live, your science will also fail and if he has decided otherwise, your science will be able to do nothing for her.” (P5) “If I do not have I will be grateful to God, almighty, but if I get it, I will follow the protocol.” (P6)
Sub-theme - Minimization
“If you keep your willpower strong, the illness will go away on its own. This is all about that. If you consider this as an illness, you will not be able to survive a single second.” (P5)
Sub-theme - Sharing experiences
“I am also active on blogs and find out ways to talk to people who know about the disease, better understanding is always necessary.” (P6)
Sub-theme - Faith and hope in treatment
“Tell me about gene therapy, which is a treatment for the disease.” (P2) “What I understand is it is a disease, so being worried about is there is of no use, we have to seek proper treatment.” (P3) “No mam we will not leave that (follow-up). We will follow up continuously.” (P5)
Theme 5 Perceived needs
Sub-theme - Need for information
“I was not aware of the disease. Only I came to know about it when the doctor told… Being informed about the disease will help to reduce unnecessary fear.” (P3) “I do not know much. The doctor told me that the disease is a genetic disease.” (P4) “It comes from genes. I don't know anything apart from this.” (P5) “If we have the protocols like when he has severe pain, I should know that he is to be taken to the emergency. Experts will take care of it but if I do not have protocols, then it becomes difficult, what should I do now?” (P6).
Discussion
Studies have reported better 5-year survival rate in the individuals who opted for screening and surveillance programs as compared to those who did not. 9 The advantage of using the screening regimen is that cancer can be detected early in asymptomatic individuals and they can be followed up and provided supportive care. 6 In a 2009 study, most individuals believed in the value of surveillance to find the tumour at an early stage and reported psychological benefits, including a better sense of control and security, when they participated in a regular surveillance program. 10
23% of the individuals undergoing genetic testing for LFS reportedly had clinically relevant distress,
11
which can be attributed to worry and the perceived risk of having cancer of higher levels.
12
The available literature on the disease suggests that approximately 80–93% of individuals with LFS have inherited it.13, 14 Further the prevalent history of cancer in the family members can add to the overall distress among them which was also found in the present study.
12
A new uncertainty about living with high multi-organ cancer risk was however introduced upon learning about their gene status.
15
In the interviewees, uncertainty about the life and future was a prominent sub-theme (n = 4, 66.6%) with subjects expressing concerns and fear about the terminal nature of the illness. Figure 1 describes the schema of experiences and developing coping mechanisms by the patients as well as their caregivers Thematic schema developed from experiences and coping strategies of LFS affected individuals and their caregivers.
Family members acted as a protective buffer by limiting to share of anxieties and other negative psychological experiences with the affected to negate the feelings of apprehension and emotional upheavals. 16 The treatment process, screenings and the uncertainty of disease progression further mental and physical fatigue leading to increased psychological burden among the affected population. 6 This forced most of the participants of this study to prepare their family members to live in a future sans the affected. 17 Constant self-doubt and anticipatory guilt disallow them from developing adult relationships with the opposite sex. 18
Friends and family act as protective padding when faced with all these stressors by allowing them to ventilate repressed and deeply held feelings. Spouses or best friends tended to be the most suitable confidantes along with close family members. 19 Good family and peer support, information about the illness and accountability for own health may hence, aid in adherence to screening programs, and treatment protocols and improve family and social life. 20 Among our interviewees, this included external support sought from friends and family by the subjects to deal with their concerns.
The increased psychological burden of the illness may be cushioned by effective counselling and dispersing of doubts by the treating healthcare professional to aid in the understanding of the disease. 21 The relevance of this need for providing information is reflected by 4 (66.6%) interviewees expressing the perceived need of greater information regarding LFS. The psychosocial morbidity of the disease can be alleviated by addressing the various social, emotional, physical and spiritual needs of the individuals. Healthcare professionals should disseminate vital information about the illness to the affected individuals and their caregivers and initiate and involve them in possible courses of action as part of the treatment. The present study is one of its kind in India that explored the lived-in experiences and the coping strategies of the individuals affected with LFS. The present study has some limitations. Due to rarity of the disease, we could contact only a few affected individuals. A significant number of individuals with the disease denied participation in the study and the family members of affected individuals were also not in favour of holding the interview. The lack of information seems to be a precursor to the denial of diagnosis. Their experience with the illness sheds light on the grey areas like guilt and helplessness that demand immediate attention.
Conclusion
LFS-affected individuals had a range of experiences with this rare and little-known disease. Their experience with the illness sheds light on the grey areas like guilt and helplessness that demand immediate attention. Future policies need to be developed in accordance with the identified perceived needs to guide the treatment and rising needs of LFS-affected individuals.
Footnotes
Authors contribution
Poonam Joshi and Shivani Bhandari wrote the first draft of the manuscript. Ajesh TK, Simran Kaur and Rachna Bhargava reviewed and edited the manuscript and approved the final version of the manuscript. Ghazal Tansir and Sameer Rastogi provided the clinical inputs and performed editing and formatting of the final manuscript draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Include full name of committee approving the research and if available mention reference number of that approval: Ethical approval for this study has been obtained from Institute Ethical Committee, All India Institute of Medical Sciences (AIIMS), New Delhi (Reference number: IEC-112/05.02.2021).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.