
Abstract
Objectives:
Frontline healthcare workers encountered a heightened susceptibility to negative psychological symptoms and behavioral shifts in light of the coronavirus disease 2019 pandemic. This study determined the coping strategies adopted by frontline healthcare workers in Ghana as well as assessed any differences based on demographics, job title, and ranking in four coronavirus disease 2019-designated centers in the Greater Accra region of Ghana.
Methods:
Using a hospital-based, mixed-method approach, the study was conducted between May 2021 and September 2021. A total of 94 frontline healthcare workers were randomly sampled and given a self-administered questionnaire, while 13 healthcare workers took in-depth interviews. Data from the survey were analyzed using both IBM SPSS and IBM AMOS and the interview data were transcribed verbatim and coded using thematic analysis.
Results:
The study revealed that coronavirus disease 2019 has affected the psycho-social life of frontline healthcare workers mainly in the form of depression, anxiety, and stress. The three main coping strategies adopted by frontline healthcare workers include personal preventative measures (most dominant), seeking external expert support, and obtaining institutional support. While healthcare workers within the age group 30–39 years were found most compliant with the adoption of personal preventive measures and those below 30 years were found least compliant.
Conclusion:
This study concludes that frontline healthcare workers have been affected by a considerable level of anxiety, stress, and depression during the coronavirus disease 2019 pandemic. The study recommends a robust psychological support system at various levels of health care and an Employee Assistance Program with access to a 24-h hotline counseling service for frontline healthcare workers, continuous personal protective equipment provision, regular evidence-based updates on the management of coronavirus disease 2019 patients, and increased commitment from the government in addressing the medical needs of infected frontline healthcare workers.
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 was first identified in December 2019 at a seafood market in Wuhan, Hubei Province, China.1–3 Further analysis of the virus revealed that it can be transmitted from person to person. 4 On January 31, 2020, the World Health Organization (WHO) declared the COVID-19 outbreak as a public health emergency of international concern, and on March 11, 2020, it classified it as a pandemic. 5 In addition, the WHO announced the implementation of social distancing measures to help control the spread of the pandemic. The emergence of the COVID-19 pandemic took the world by surprise, and its consequences have been devastating, surpassing what many could have imagined in the modern era.
As of March 12, 2023, there have been more than 760 million confirmed cases and over 6.8 million reported deaths worldwide. 6 In Ghana, the first two cases of COVID-19 were noted on March 12, 2020, in Accra and were both imported. 7 According to the Ministry of Health (MOH) and the Ghana Health Service, the infection progressively spread to the rest of the country over the next 6 months and as of March 20, 2023, there were 171,412 confirmed cases and over 1460 deaths from COVID-19 in Ghana. 8 The confirmed cases and death from COVID-19 in Ghana have been relatively lower compared to the global average.
Healthcare workers were considered essential workers or key frontline workers and included medical doctors, nurses, laboratory scientists, public health workers, paramedics, ambulance drivers, and hospital environmental workers. Encumbered with challenges such as lack of personal protective equipment (PPE), lack of intensive care units (ICUs), and bed capacity in various hospitals as well as limited psychological support for the healthcare workers as noted in several studies; the urgent need arises to address such concerns to prevent professional burnout and mental health disorders as the pandemic ravages on in the country and the world at large.9–12
With the unprecedented devastating impact of the COVID-19 pandemic globally, healthcare workers at the frontline in response to this pandemic are faced with an increased risk of adverse psychological symptoms and behavioral changes. 13
Internationally, some studies mainly from Wuhan, China identified the COVID-19 pandemic as an increased risk of moderate to severe mental health disorders such as stress, anxiety, and depression among frontline healthcare workers and the populace.14–17 In the United States, UK, and Portugal, similar studies also identified COVID-19 as a workplace hazard for healthcare workers who manifested moderate to severe levels of stress, anxiety, and depressive symptoms.13,18–20 A study in South Africa among frontline nurses indicated that more than four in every ten nurses exhibited symptoms of high levels of posttraumatic disorder during screening. 21 In Ghana, 22 fear, anxiety, stress, and depression are the main mental health effects of the pandemic on health workers, with 40% experiencing fear and about 28% experiencing anxiety. 17
With the huge burden of COVID-19 and its attendant mental health disorders among healthcare workers, there is scarce existing information on the coping strategies healthcare workers employ in managing psychological stressors and burnout during the COVID-19 pandemic in Africa. The data are even scarcer in Sub-Saharan Africa and more limited information on the psychological impact of COVID-19 on the mental health of people during the COVID-19 pandemic in Ghana.22,23 Such information is particularly crucial amid the enigma of a pandemic of such unmatched proportion.
With the increasing psychological burden of the COVID-19 pandemic among the populace and healthcare professionals, the call for reinforced mental health support has been heightened from all quarters—national and international alike.10,12
With limited data on the psychological effects of COVID-19 on healthcare workers and associated coping strategies in Ghana, this study seeks to assess coping strategies employed by frontline healthcare workers who work specifically in COVID-19-designated facilities in Ghana’s capital city, Accra which has recorded the highest burden on COVID-19 cases since the pandemic began. Identifying the current coping strategies being employed by frontline workers will help inform the formulation of policies and the development of mental health support structures for healthcare workers.
Systematic reviews done explored the psychological impacts of COVID-19 on health workers worldwide and found data on psychological issues such as anxiety, depression, and stress as the highest prevailing mental health issues among healthcare workers globally.24,25 In some settings, single doctors, nurses, and healthcare workers working in the emergency rooms were found to have a greater predisposition to mental health problems.26–28 In Wuhan specifically, factors that were associated with mental health disorders among health workers included increased workload, lack of sleep, fear, and discrimination. 29
A cross-sectional survey conducted in the Ashanti region of Ghana in 2020 found that out of 272 healthcare workers in three COVID-19 health facilities, 21.1%, 27.8%, and 8.2% had depression, anxiety, and stress, respectively. 22 Major contributing factors noted in multiple studies indicated that the lack of PPE, increased risk of exposure to infection to family and friends, reduced social support due to lockdown, and restrictions as well as poor adherence to COVID-19 protocol by the general public were stressors to many healthcare workers.22,24,30 In addition, overburdening of the healthcare systems due to the increased caseload of COVID-19, lack of bed space in ICUs, and lack of oxygen were also some psychological stressors among first responders and frontline health workers.31,32
Coping strategies are strategies that drive the thoughts and behaviors used to control stressful occurrences that are internal and external. Coping strategies ruminate from conscious and voluntary efforts or acts and differ from defense mechanisms which are unconscious or subconscious adaptive responses, though both help to manage stress. 33 A study done in Indonesia found that family support was the main factor that motivates healthcare workers to provide healthcare services during the COVID-19 outbreak. 34 Other studies have highlighted seeking social support and altruism as major factors fueling resilience and reducing professional burnout among healthcare workers in COVID-19 isolation centers.31,32,35
According to the WHO, work-related stress is a reaction that people may have when confronted with work expectations and pressures that are not suited to their knowledge and capacities and that test their ability to cope. 36 On the other hand, depression is a widespread mental condition that differs from normal mood changes and short-term emotional reactions to ordinary stressors. Anxiety is a feeling of tension, disturbed thoughts, and bodily changes such as higher blood pressure.
Several studies have established evidence of psychological health problems such as fear, depression, anxiety, and burnout among frontline health professionals in COVID-19 isolation centers around the world.24,31,32,34,37 These mental health issues are complicated by the increasing caseload of COVID-19 cases, strained health systems, and resources, and lack of PPE among others.26,28,38 In addition, it is crucial to understand the spectrum of coping strategies and how successful these coping strategies are toward achieving resilience, a better attitude to work, increased efficiency, and ultimately, improved patient outcomes in COVID-19-designated health facilities in Accra, Ghana.
As far as our current knowledge extends, there has been no empirical investigation conducted employing a mixed-method research approach to examine coping strategies utilized by frontline healthcare workers in COVID-19-designated centers within a developing country. Existing studies focusing on developing countries, particularly in Africa, have predominantly employed either a quantitative approach 39 or a qualitative approach. 40 In addition, the majority of empirical studies have been conducted within a hospital setting,39–41 while the present study specifically includes an infectious disease center designated for the COVID-19 treatment. Consequently, this study contributes valuable insights into the existing literature on developing countries, which is currently lacking in this area.
Methods
The study employed a hospital-based, cross-sectional study using a mixed-method research design to investigate the coping strategies adopted by frontline health workers in four COVID-19-designated health facilities in Accra. The study was undertaken between May 2021 and September 2021. A mixed-method research design was chosen because it integrates both the qualitative and quantitative research design and data. Qualitative data were derived from an interview guide which is open ended, with no predefined replies, whereas the quantitative data were typically closed ended.
Although there are several designs in the mixed-methods field, 42 primarily, there are three types of mixed-method approaches namely, convergent parallel, explanatory sequential, and exploratory sequential mixed methods. In explanatory sequential mixed methods, the researcher first does quantitative research, analyses the data, and then uses qualitative research to describe them in further depth. The exploratory type is however the inverse. The researcher begins with a qualitative research phase in which he or she investigates the perspectives of participants. The knowledge gleaned from the data is then utilized to construct a second, quantitative phase. In this study, the mixed-method type used was the convergent parallel mixed approach. Here, the authors combined the quantitative and qualitative data to offer a thorough overview of the research topic. The authors gathered both types of data at around the same time and then incorporate the information into the interpretation of the overall findings. In this study, contradictions or incongruent findings are explained or investigated further. 42
When qualitative and quantitative methodologies are combined, they give a more thorough knowledge of a study topic than either strategy alone. Mixed-method design was employed because it provides a diverse point of view of the study. The mixed method was used so that the qualitative findings were expected to confirm the quantitative findings. By integrating quantitative and qualitative methods, the potential weaknesses of each approach can be addressed, resulting in an effective methodology that incorporates triangulation as an integral part of the process.
Study areas
Four health facilities were involved in the study namely, the Greater Accra Regional Hospital (GARH), 37 Military Hospital, Ghana Infectious Disease Centre (GIDC), and Nyaho Medical Center (NMC). The GARH is situated in Accra, the capital city of Ghana. It currently has one of the foremost isolation centers under the Ghana Health Service during the COVID-19 pandemic; the isolation center has about 32 beds with round-the-clock medical care and attention of medical doctors (physicians, medical officers, anesthesiologists), physician assistants, nurses, pharmacists, and among others. The 37 Military Hospital (37MH) is a specialist hospital also located in Accra. It is the largest military hospital in Ghana and, currently, has about 400 beds with a 24-h accident and emergency department and pharmacy and radiograph units. The hospital is also used as a teaching hospital for postgraduate medical students. 37MH also acts as a COVID-19 isolation center for COVID-19 patients in Accra and beyond.
GIDC is a newly built ultra-modern ICU for critically ill COVID-19 patients requiring mechanical ventilation. It was recently built by the government of Ghana with support from other NGOs to help manage the severe COVID-19 cases in the country. It provides a 30-bed capacity for severely ill COVID-19 patients manned by intensive care internists and anesthetists with support from medical officers, nursing staff, and other staff. NMC was established in March 1970 and is one of the largest private health facilities in Ghana. NMC currently serves as one of the isolation centers for COVID-19 disease in Accra.
Study population
The study population consisted of all clinical staff working in these four COVID-19-designated isolation centers. The clinical staff are those directly involved in the management of patients with COVID-19 infection, and they include medical doctors of all cadres (from house officers to specialist physicians and anesthesiologists) as well as nursing staff, physician assistants, pharmacists, laboratory scientists, paramedics, and environmental staff. For a clinical staff to be included in the survey, he or she must be at the forefront of the management of COVID-19 patients and must be present at the health facility within the period of the survey. Nonclinical workers such as the administrative staff of the hospital were excluded from this study.
Sampling technique and sample size
Participants were randomly selected from the four COVID-19-designated facilities in the capital city, Accra. Healthcare workers from the hospital COVID-19 management team were administered a questionnaire assessing coping strategies in the pandemic using a simple random sampling method to derive the quantitative data. For the qualitative study, 13 healthcare workers who gave written informed consent were selected through a random purposeful sampling strategy and undertook an in-depth interview using an interview guide which was then transcribed and coded. Themes were derived from the data. We compiled a list of all the COVID-19 healthcare staff in the facilities and gave them numbers. We randomly selected the participants and interviewed them till we reached saturation point (where the information was similar). The sample size for the quantitative study was estimated using Cochran’s formula:
where Z is the reliability coefficient = 1.96 at a 95% confidence interval; p is the proportion of health workers with psychological effects such as depression from the outbreak of COVID-19; q is (1 − p); and d is the desired precision.
Assuming a 35% prevalence of depression among health workers from a previous study 43 and a precision of 10%, a sample size of 87 was estimated. The overall sample size came to 100 with an upward adjustment of 10% to account for non-response rates. Cochran’s formula was used since the population of healthcare workers is infinite as more staff are engaged on locum and that a fraction of the population that exhibits the attributes of psychological effect is known. 44
Instrumentation
The questionnaire was designed in English since all the respondents have some level of education. The questionnaire was segmented into five sections (Sections A, B, C, D, and E). Section A focused on the sociodemographic characteristics of the respondents which solicited information on the age, sex, marital status, educational background, religion, job title/rank, number of years of working, and hospital of affiliation. Sections B, C, D, and E are 5-Likert scale capturing the fear of COVID-19, modified depression, anxiety and stress, mitigating factors, and coping strategies, respectively. The interview guide was made up of 11 set of questions which included coping strategies employed, psychosocial support, and management of COVID-19. The interview was taken within 10 min. To enhance the credibility of the findings, the participant transcripts were returned to each individual for verification, correction, and further elaboration on any opinions they expressed during the interviews.
Pilot study
A pilot study was done to assess the ease of acceptability and administration of the online questionnaire. The pilot survey tested the correctness of the instructions to be measured by whether all the respondents in the pilot sample were able to follow the directions as indicated. It also provided enhanced information such as whether the survey was useful in fulfilling the objectives of the study as well as other measures such as duration of answering the questionnaire, feasibility, cost, and compliance to instructions in the survey. This pilot study was conducted among health workers in a COVID-19-designated area in Korle-Bu Teaching Hospital (KBTH) to reduce bias. After eligibility criteria were confirmed and written informed consent was obtained, participants were administered a questionnaire. The questionnaire was administered to a sample of 20 frontline health workers in the KBTH. All participants who failed to complete the survey after two follow-up checks were recorded as non-respondents.
Data analysis
The questionnaire screening resulted in 94 usable questionnaires, resulting in a 94% response rate. Since the response rate was high, non-response bias was not calculated. The 94 usable questionnaires were coded into the IBM SPSS version 27 software by the first author. Each of the 24 items in the 5-point Likert Scale was tested for normality in line with recommendations from the previous study. 45 Data on types of coping strategies were analyzed using percentages, the differences in percentages between genders, age groups, job titles, and ranking.
Descriptive analysis was done using frequencies and charts to represent the variables of interest. A p-value of 0.05 and 95% confidence intervals were used as a benchmark for significant differences. One-way ANOVA was conducted for the association between the categorical explanatory variables such as sex, age, marital status, number of dependents, job description, study hospital, and religion and the categorical outcome variables of depression, anxiety, stress, and fear of COVID-19 scores. For the qualitative section, in analyzing data on the impact of COVID-19 on the professional and psycho-social life of frontline health workers, the responses of the participants were analyzed narratively.
The 24-item 5-point Likert Scale was subjected to exploratory factor analysis using the principal component analysis (see Table 2) method to know the factor structure of the coping strategies adopted by the participants during the pandemic. 45 The analysis was performed with the extraction of Eigenvalues greater than 1 and Varimax Rotation. 46
The psychometric properties of the five factors (scales) which include the fear of COVID-19, depression, anxiety and stress, personal preventative measures, external expert support, and institutional support were assessed through a process of confirmatory factor analysis. The purpose of the confirmatory factor analysis is to assess the psychometric properties of the extracted scales/factors from exploratory factor analyses. 47 Consequently, it acts as a form of validation/verification for the factors extracted. The validation process involves the test of model fit indices, convergent validity, and discriminant validity. The model was validated using IBM AMOS structural equation modeling version 23 (see Appendix).
COVID-19 protocol adherence
The emergence and spread of COVID-19 disease have affected and continue to affect various aspects of life particularly health, not excluding research. Measures put in place to reduce the risk of participants and study teams contracting COVID-19 include alcohol-based hand sanitizers being made available for intermittent use at the study site. There was strict adherence to social distancing keeping at least 6 ft or as set in study facilities. Adequate PPE was made available to study team members. All researchers had adequate protection by practicing good personal hygiene through regular hand washing, the use of sanitizers, protective gloves, and wearing face masks.
Results
The data were validated through the assessment of outliers and normality. All the skewness for the 24 items falls within the range of −1.5 to 1.6. Also, all the kurtosis items were below 2.7; therefore, the data present no significant outliers and also assume multivariate normality. 45
Demographic data
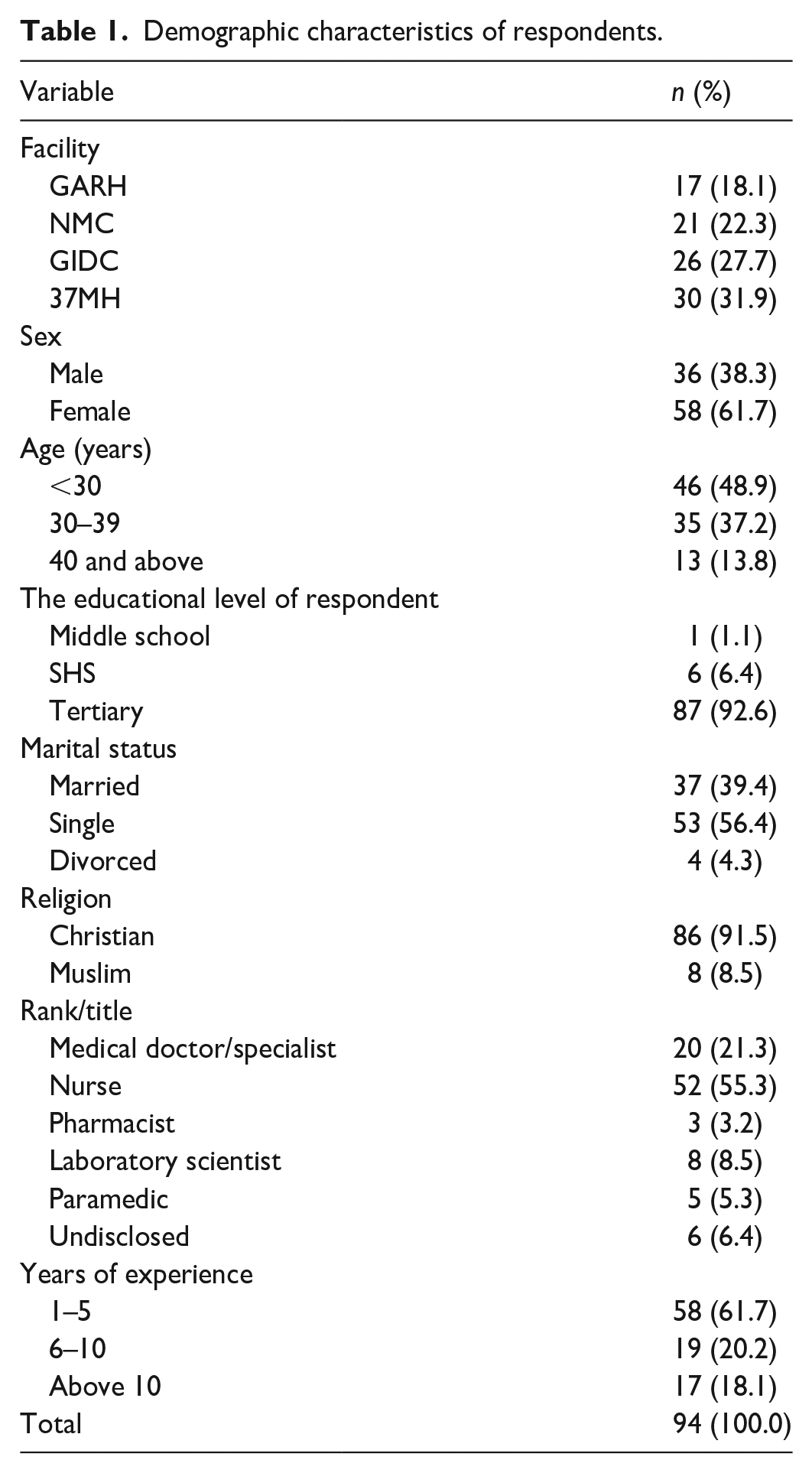
Of the 94 respondents in the survey, the majority were frontline health personnel from 37MH (n = 30, 31.9%), followed by the GIDC (n = 26, 27.7%), NMC (n = 21, 22.3%), and GARH (n = 17, 18.1%). The majority of the respondents were female (n = 58, 61.7%) and the rest were males (n = 36, 38.3%). Almost half of the respondents were under 30 years (n = 46, 48.9%), and the rest were between 30 and 39 years (n = 35, 37.2%) and 40 years and above (n = 13, 13.8%). Almost all the respondents had tertiary education (n = 87, 92.6%), with just a few of them having SHS (n = 6, 6.4%) and middle school education (n = 1, 1.1%). Most of the respondents were single (n = 53, 56.4%), closely followed by those who were married (n = 37, 39.4%), and those who were divorced (n = 4, 4.3%). Nine in ten respondents were Christians (n = 86, 91.5%), whereas the rest were Muslims (n = 8, 8.5%). The main ranks represented in the study include nurses (n = 52, 55.3%), medical doctors/specialists (n = 20, 21.3%), laboratory scientists (n = 8, 8.5%), paramedics (n = 5, 5.3%), and pharmacists (n = 3, 3.2%). Three in five respondents had a maximum of 5 years of experience (n = 58, 61.7%), followed by 6–10 years of experience (n = 19, 20.2%), and above 10 years of experience (n = 17, 18.1%). See Table 1 for details.
Demographic characteristics of respondents.
In the qualitative study, 13 healthcare workers were interviewed (see Table 2). Three of whom were medical doctors and 10 were nurses. Out of the 13 participants in the interview, 4 were chosen randomly from GARH, 5 from GIDC, and 4 from 37MH. Also, six of the participants were males and seven were females. Mean work experience averaged 4 years for medical doctors and 15 years for the nurses interviewed. All health workers were directly involved in the management of critically ill COVID-19 patients in the isolation centers.
Demographic data of respondents to the interview.

The result of the principal component analysis is presented in Table 3. The analysis produced five factors explaining a total variance of 66%. A Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy value of 0.749 shows that the sample size is adequate for factor analysis. Also, Bartlett’s test of sphericity of chi-square of 665 and p < 0.001 was obtained implying that the variables correlate well. Factor 1 relates to the “fear of COVID-19.” Factor 2 relates to “personal preventative measures” such as following COVID protocols such as hand washing, sanitizing, observing social distancing, taking zinc and vitamin C supplements, and living a healthy lifestyle. Factor 3 relates to “depression, anxiety, and stress” such as feeling scared without good reason, having nothing to look forward to, and finding it difficult to relax. Factor 4 relates to “seeking external expert support” such as talking to religious leaders, praying more, seeking help from psychologists, and avoiding media news about COVID-19. The final factor relates to “mitigating factors/institutional support” such as the provision of PPEs by the hospital, government tax waivers, insurance, and support from their facilities should they get infected.
Principal component analysis.


Source. Field data (2021).
Extraction method: principal component analysis. Rotation method: varimax with Kaiser normalization. KMO = 0.749; Barlett’s test chi-square = 665.38, df = 153, p = .000; total variance explained = 66%.
Shaded region indicates large positive factor loadings.
The reliability analysis of the extracted factors using Cronbach’s coefficients alpha was computed. All five factors meet the minimum threshold of 0.60 for exploratory study. The measurement model showed satisfactory model fit indices. This is because the χ2/df ratio of 1.46 was lower than 5, the root mean square error of approximation value of 0.070 was lower than 0.08, and the comparative fit index of 0.90 matched the recommended threshold of 0.90.47,48
Convergent validity was obtained by assessing both composite reliability and average variance extracted. Convergent validity has been met due to the fact that the model had acceptable fit indices. Furthermore, all the composite reliabilities were above 0.60 and the average variance extracted estimates was higher than 0.30 (see Table 4). In addition to convergent validity, the study also assessed discriminant validity which was met as evidenced by the fact the inter-construct correlation values were all lower than the square root of the average variance extracted estimates.49,50
Psychometric properties and testing.
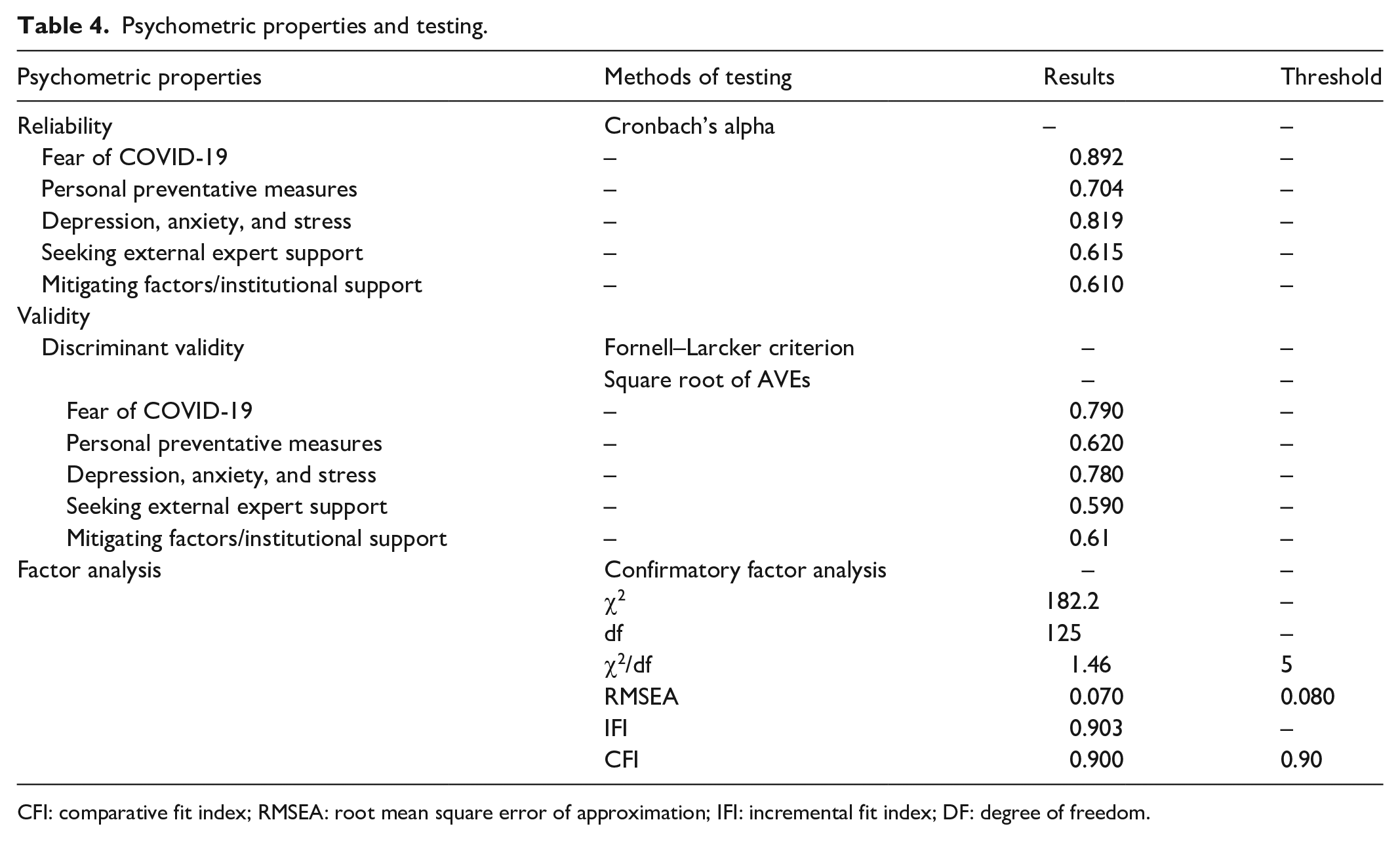
CFI: comparative fit index; RMSEA: root mean square error of approximation; IFI: incremental fit index; DF: degree of freedom.
The effect of COVID-19 on the professional and psycho-social life of frontline healthcare workers
A structural equation modeling was performed using IBM AMOS version 23, by examining the effects of the fear of COVID-19, taking personal preventative measures, seeking external export support, and having institutional support on the psycho-social life of frontline health workers measured in the form of depression, anxiety, and stress (see Appendix).
The findings showed that the fear of COVID-19 has a significant positive effect on depression, anxiety, and stress (β = 54, t = 6.3, p < 0.001). This implies that depression, anxiety, and stress levels of frontline health personnel may have been exacerbated by the fear of COVID-19.
This corroborates the findings from the interview. Sharing their experiences at the COVID-19 isolation centers, some of the frontline health workers reiterated their fear of contracting COVID-19, the discomfort of wearing PPEs for long periods and being overwhelmed with work during the third wave of disease as major psychological stressors. One of them stated that:
The number of patients is a real source of stress. We were understaffed and some were afraid of contracting the disease. When patients are at full capacity, we are stressed psychologically. Also, the wearing of the PPE is not easy. When you are fully gowned, you sometimes suffocate so you have to rush out and pull it off even when you are not done with your task. (GARH, Male, Medical Specialist)
Another highlighted the sense of depression, helplessness, and fear of managing patients with COVID-19:
. . . emotionally, there are some of the deaths you wish you can do more but there is nothing you can do. Sometimes you see people dying and you can’t do anything more. It emotionally affects us as I can’t sleep at night. Seeing some people, you wish you could have saved. Most also delay before coming so they get here and they are already in a critical state which can be depressing. I was also afraid of getting COVID-19. When I was first posted here I wondered why because no one wanted to come there. Other nurses and doctors from other departments don’t even want to come inside the ward because of fear of contracting the COVID-19 disease. (37MH, Female, Nurse)
The study found a positive significant relationship between the tendency to seek external expert support and depression, anxiety, and stress levels of health workers (β = 0.16, t = 1.91, p < 0.10). This implies that health workers who may have been seeking more support from religious leaders, praying more, and seeking the support of psychologists may have been personnel that exhibited more signs of depression, anxiety, and stress. Also, the adoption of personal preventative measures such as hand washing, sanitizing, observing social distancing, taking zinc and vitamin C supplements, and living a healthy lifestyle by health personnel has a negative effect on depression, anxiety, and stress, although the relationship was not statistically significant (β = −0.12, t = 1.41, p > 0.10). The effect of institutional support did not have a significant influence on the levels of depression, anxiety, and stress (β = 0.05, t = 0.55, p > 0.10).
Coping strategies on the psychological effects of COVID-19
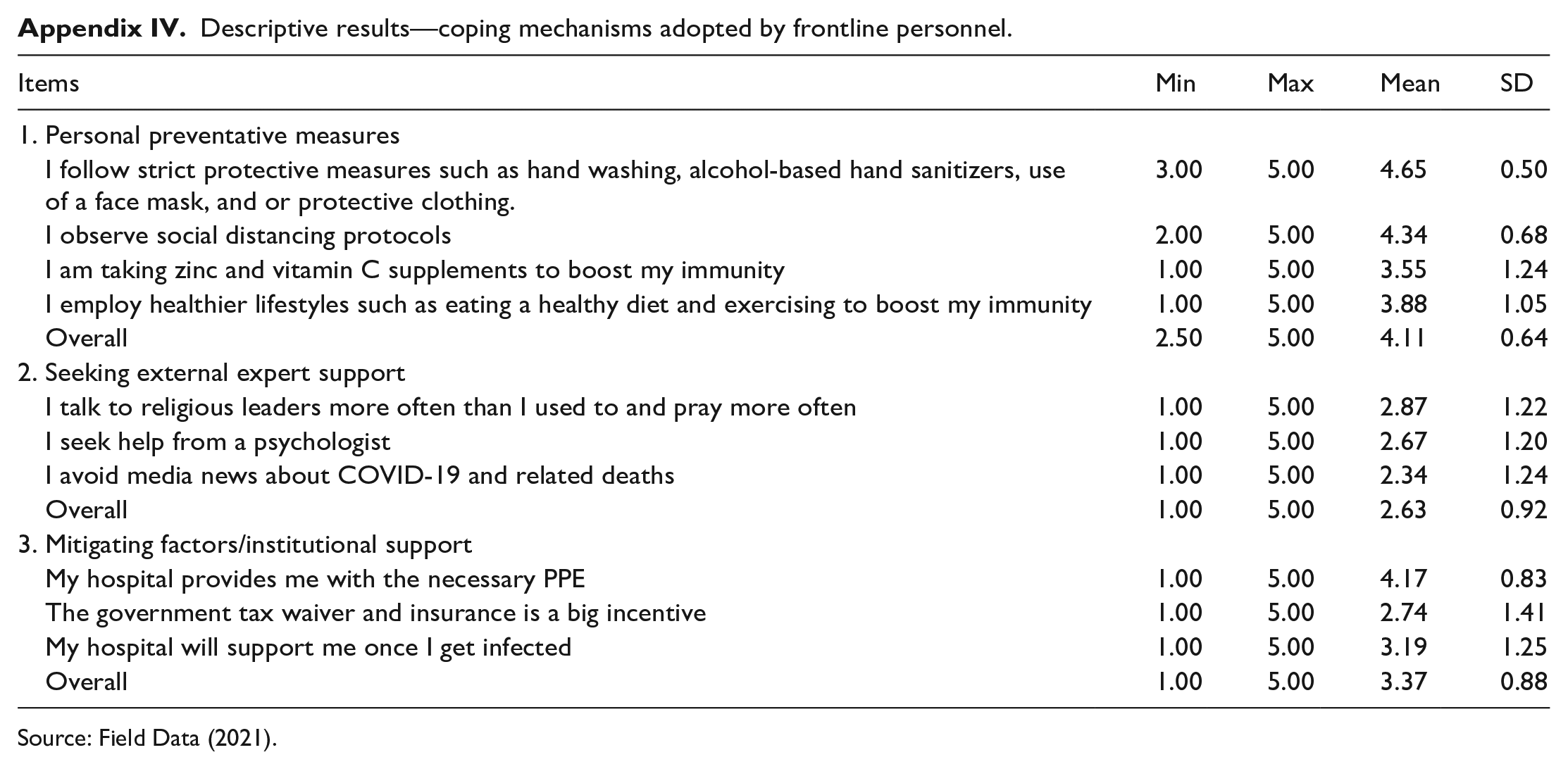
The three main coping strategies adopted by the frontline personnel include personal preventative measures, seeking external expert support, and obtaining institutional support. Comparatively, the most dominant strategy adopted was the use of personal preventative measures (mean = 4.11), followed by institutional support (mean = 3.37) and seeking external expert support (mean = 2.63) in descending order of importance. Interviews with frontline health also brought to the fore other coping strategies adopted that were helpful in managing COVID-19 patients. Some of these were social interaction with other colleagues, staff support, and playing games. Two responses from in-depth interviews reiterated this:
Work colleagues help relieve stress and fear, as we laugh and make jokes, it helps to reduce the stress. When you have a colleague that is joyful and you guys get along well, it helps you manage your stress. (GIDC, Male, Medical Specialist) My team is very strong, so we fall on each other when the one is weak or down. We try to support each other and then once a while we try to organize a lunch for ourselves. (37MH, Female, Nurse)
Personal preventative measures adoption
The most dominant personal preventative measures adopted by the frontline personnel were following strict protective measures such as hand washing, alcohol-based hand sanitizers, use of face masks, and or protective clothing (mean = 4.65). This is followed by the observance of social distancing (mean = 4.34), the adoption of healthier lifestyles such as eating a healthy diet and exercising to boost immunity (mean = 3.88), and taking zinc and vitamin C supplements to boost immunity (mean = 3.55) in descending order of importance.
Seeking external expert support
The most dominant external expert support measures adopted by the frontline personnel were praying more and talking to religious leaders (mean = 2.87). This is followed by talking to psychologists (mean = 2.67) and avoiding negative COVID-19 media news (mean = 2.34).
Mitigating factors/institutional support
The most dominant of the institutional support measures adopted was the fact that the hospital provides them with the necessary PPE (mean = 4.17). This is followed by the fact that the hospital will support them if they get infected (mean = 3.19), with the government’s tax waiver and insurance being their least motivator (mean = 2.74).
During the qualitative interviews, most frontline health workers recommended an incentive package as well as structured mandatory psychological support for health workers. One stated:
Talking of remuneration, there should be a package such that even if you also fall sick due to the job, you won’t regret it. Counseling and other psychological support will help but we don’t have anything of that sort here. The patients have a clinical psychologist, but the staff doesn’t. It is not compulsory but if staff wants one, there is no system for that. (GARH, Male, Medical Doctor)
Differences in coping strategies based on demographics, job title, and ranking
To assess the perceived differences in coping strategies employed by frontline personnel based on demographics, and job title, a variety of statistical tools including one-way ANOVA and t-test were employed since the questionnaire items assume normal distribution. Perceived differences in coping strategies due to gender, age, and job title are presented in Tables 4–6, respectively.
Differences in coping mechanisms due to gender—mean comparison using independent samples t-test.

Source: Field Data (2021).
p < 0.001. **p < 0.01. *p < 0.05.
Differences in coping mechanisms due to age group—one-way ANOVA.
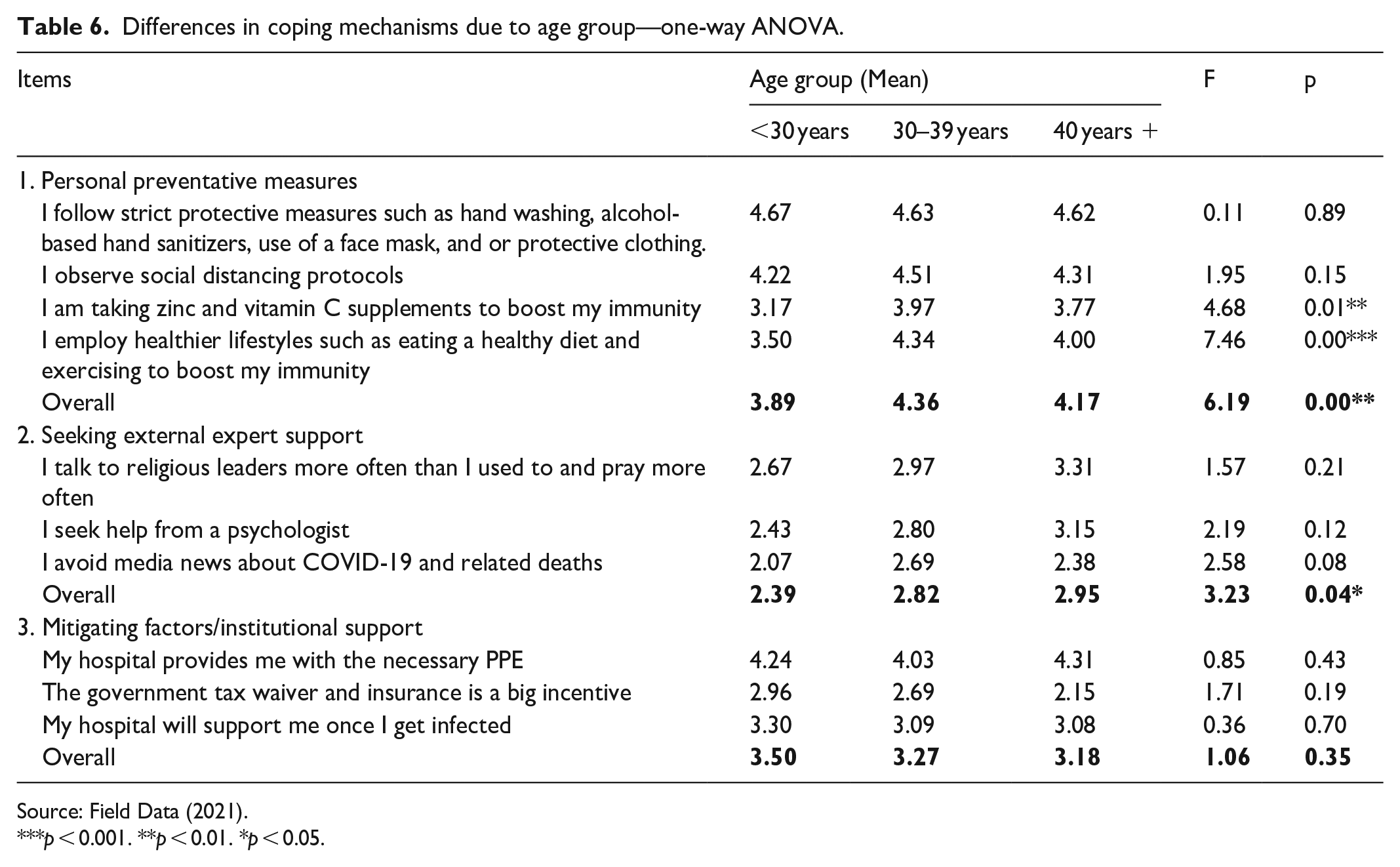
Source: Field Data (2021).
p < 0.001. **p < 0.01. *p < 0.05.
Gender differences
There was no significant difference between male and female frontline personnel regarding the adoption of personal preventative measures as well as seeking external support (p > 0.05).
There was however a significant difference between males and females in their perception of the government’s tax waiver and insurance for frontline personnel (t = −1.96, p < 0.05) and perception as to whether or not their facilities will support them should they get infected. Specifically, females (mean = 2.97) trust more the government’s tax waiver and insurance policy for frontline personnel than males (mean = 2.39). Also, females (mean = 3.43) trust their facilities to take care of them should they get infected more than males (mean = 2.81). See Table 4 for details.
Age group differences
There was a significant difference between the age groups in the adoption of overall personnel preventative measures (F = 6.19, p < 0.01). Specifically, participants within the age group 30–39 years (mean = 4.36) were the most serious when it comes to the adoption of personal preventative measures, followed by those above 40 years (mean = 4.17) and those below 30 years (mean = 3.89). It was noted that participants within the age group 30–39 years were the most compliant in taking zinc and vitamin C supplements and adopting healthy lifestyles, followed by those above 40 years and those below 30 years.
When it comes to seeking external expert support such as religious leaders, praying and seeking help from psychologists, and avoiding negative media COVID-19 news, those above 40 years were forerunners, closely followed by those between 30 and 39 years and those below 30 years, respectively (F = 3.23, p < 0.05). See Table 5 for details.
Job rank differences
The job ranking was categorized into three: medical doctors/specialists, nurses, and others (pharmacists, laboratory scientists, etc.). The results of the mean difference test for job rank using one-way ANOVA are presented in Table 6.
There was a significant difference between the job ranks in the adoption of overall personnel preventative measures (F = 5.80, p < 0.01). Specifically, nurses (mean = 4.24) were the most compliant in the adoption of personal preventative measures, followed by other ranks (mean = 4.17) and medical doctors/specialists (mean = 3.70). In individually specific assessments, nurses (mean = 3.85) were also noted to be the most compliant in taking zinc and vitamin C supplements, followed by other ranks (mean = 3.82) and medical doctors/specialists (mean = 2.50). In terms of support of health facilities, other ranks (mean = 3.77) and medical doctors/specialists (mean = 3.35) trust their facilities to take care of them should they get infected more than nurses (mean = 2.88) (see Table 7).
Differences in coping mechanisms due to rank—one-way ANOVA.

Source: Field Data (2021).
p < 0.001. **p < 0.01. *p < 0.05.
Discussion
Health system constraints, an already existing major socioeconomic challenge in low- and middle-income countries like Ghana, have been compounded by the occurrence of the evolving global COVID-19 pandemic and have had devastating effects on the health and economy of almost all countries around the world. This study confirms that the psychological impact of COVID-19 on frontline health workers is significant with depression, anxiety, and stress experienced by a considerable proportion of frontline health workers; this is often exacerbated by the fear of contracting and spreading COVID-19 to family and friends. This has been alluded to by other studies done around the world,31,51–53 also adding context and cultural factors as contributing to the mitigation of the severity of psychological challenges faced by health workers.54,55 This study also indicated that health workers seeking external support for psychological problems (religious prayers, psychological counseling) were more likely to have depression, anxiety, and stress and hence drawing the inference of inadequate psychological support system and/or impact in place for frontline health workers who voluntarily seek support for mental health challenges they face in Accra.
The three main coping strategies adopted by the frontline personnel included the institution of personal preventative measures, seeking external expert support, and obtaining institutional support. The availability and adequacy of PPE were the most expressively stated by health workers as a dominant coping strategies, hence was protective when present and a risk factor for increased stress and anxiety when absent. Other adaptive measures which emerged from the qualitative study highlighted better patient outcomes and gratitude from patients’ relatives providing a sense of fulfillment and easing tension and stress associated with managing COVID-19 patients in a constrained health system. This is contrary to existing studies, which found that the adoption of personal protective measures and a healthy lifestyle did not have a significant effect on the levels of depression, anxiety, and stress among frontline health workers.31,52
The study also assessed a differential adaptation of protective measures among the varying cadres of health workers. Nurses were the most compliant in the adoption of personal preventive measures than medical doctors/specialists and other ranks, partly because nurses had the least trust in their facilities’ ability and willingness to cater to their medical needs should they get infected with COVID-19 infection. There was no differential adaptation between gender in this study, unlike other studies56,57 where females were found more cautious in instituting personal protective measures. The results of empirical studies do not align with the findings regarding the similarities in adaptation between male and female frontline healthcare workers. This provides valuable insights into the perspective of developing countries. Individuals aged above the age of 30 years were found more adherent to COVID-19 protocols than those below the age of 30 years. This can partly be explained by the prior circulating knowledge that the alpha variant of the COVID-19 virus had less severity in the younger populace than the older populace; the old with comorbidities developed the severe disease when infected.
Limitations
Nonclinical staff such as social workers and hospital maintenance staff who do not directly manage COVID-19 patients were excluded from the study. Only health workers at the post in COVID-19-designated health facilities during the study period were sampled; those not at the post but may have other mental health concerns and insights were not sampled. All study sites were clustered in the Greater Accra region where the majority of the caseload of COVID-19 in the country was noted. Health workers in the other 15 regions may have differing opinions and psychological concerns based on caseloads, support, and point in the epidemic curve. Also, the qualitative study conveniently selected only doctors and nurses leaving out other frontline members, thus did not include the maximum variations in the sampling. The population of frontline healthcare workers was unknown; thus, the percent population of the pilot test of the questionnaire and interview guide was not determined.
Conclusion and recommendations
This study concludes that frontline health professionals have been affected by a considerable level of anxiety, stress, and depression during the COVID-19 pandemic. The COVID-19 pandemic has disrupted the psychological health of healthcare workers due to the increasing demand for health care in an already constrained health system. This study emphasizes the need for high-quality, evidence-based mental health interventions for the psychological well-being of healthcare workers during this COVID-19 pandemic. This study additionally reiterates the need for support systems for coping strategies that may assist to reduce stress, anxiety, and depression among healthcare workers in Ghana.
Recommendations
A robust psychological support system at various levels of health care (options for in-person and digitally based systems such as via telemedicine or 24-h telephone counseling support) must be put in place to make psychological support for frontline health workers available and easily accessible to bolster mental health outcomes among healthcare workers amid the COVID-19 pandemic. The Ghana Health Service should establish an Employee Assistance Program that will offer confidential mental health and well-being support services to frontline health workers. The study also recommends the MOH in Ghana develop policies that prioritize the well-being of healthcare workers, including strategies to manage workload, regular breaks, and adequate time off. The policy must include an implementation of shift rotation systems to prevent burnout and consider providing incentives such as hazard pay, bonuses, and recognition for their dedication and hard work.
Continuous reinforcement of efforts such as staff support, provision of PPE to health facilities, and regional and national COVID-19 health teams will go a long in improving the morale of health workers in the fight against COVID-19. Regular evidence-based updates on COVID-19 must be provided to health workers through training and retraining as well as other digital platforms, to arm them with information to aid in managing COVID-19 patients as well as maintaining their physical, mental, and social well-being.
There must be an improved financial commitment by the government in catering to the medical needs of frontline health workers who get infected with COVID-19 to boost trust and morale among health workers. Also, there needs to be increased focus on organizational-level interventions that improve the work environment and provide an easily accessible psychological support system for frontline health workers clinical and nonclinical alike to boost mental health outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231197398 – Supplemental material for A cross-sectional study on coping strategies of frontline healthcare workers amid the COVID-19 pandemic in a developing country
Supplemental material, sj-docx-1-smo-10.1177_20503121231197398 for A cross-sectional study on coping strategies of frontline healthcare workers amid the COVID-19 pandemic in a developing country by Isaac Akanko, Patience Aseweh Abor and Carlos Kokuvi Tetteh in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231197398 – Supplemental material for A cross-sectional study on coping strategies of frontline healthcare workers amid the COVID-19 pandemic in a developing country
Supplemental material, sj-docx-2-smo-10.1177_20503121231197398 for A cross-sectional study on coping strategies of frontline healthcare workers amid the COVID-19 pandemic in a developing country by Isaac Akanko, Patience Aseweh Abor and Carlos Kokuvi Tetteh in SAGE Open Medicine
Footnotes
Appendix
Measurement validity and reliability assessment results—psychometric properties of scale.

| Construct | A | CR | AVE | T values | Loading |
|---|---|---|---|---|---|
| Fear of COVID-19 | 0.892 | 0.891 | 0.621 | – | – |
| I am very afraid of COVID-19 | – | – | – | 6.662 | 0.7 |
| I am afraid of losing my life because of COVID-19 | – | – | – | 7.331 | 0.766 |
| I often cannot sleep because I’m worried about getting COVID-19. | – | – | – | 8.318 | 0.865 |
| My heart races when I think about getting COVID-19 | – | – | – | 8.229 | 0.855 |
| When watching news and stories about COVID-19 on social media, I become nervous or anxious | – | – | – | Fixed | 0.742 |
| Depression, Anxiety, and Stress | 0.819 | 0.819 | 0.602 | – | – |
| I often feel scared without any good reason | – | – | – | 6.852 | 0.766 |
| I often feel I have nothing to look forward to | – | – | – | 7 | 0.79 |
| I find it difficult to relax and often get agitated | – | – | – | Fixed | 0.771 |
| Personal preventative measures | 0.704 | 0.710 | 0.385 | – | – |
| I follow strict protective measures such as hand washing, alcohol-based hand sanitizers, use of a face mask, and or protective clothing | – | – | – | 3.942 | 0.563 |
| I observe social distancing protocols | – | – | – | 4.397 | 0.759 |
| I am taking zinc and vitamin C supplements to boost my immunity | – | – | – | 3.816 | 0.537 |
| I employ healthier lifestyles such as eating a healthy diet and exercising to boost my immunity | – | – | – | Fixed | 0.598 |
| Seeking external expert support | 0.615 | 0.622 | 0.357 | – | – |
| I talk to religious leaders more often than I used to and pray more often | – | – | – | 3.482 | 0.549 |
| I seek help from a psychologist | – | – | – | 3.52 | 0.563 |
| I avoid media news about COVID-19 and related deaths | – | – | – | Fixed | 0.672 |
| Mitigating factors/institutional support | 0.610 | 0.633 | 0.374 | – | – |
| My hospital provides me with the necessary PPE | – | – | – | 3.358 | 0.615 |
| The government tax waiver and insurance is a big incentive | – | – | – | 3.02 | 0.450 |
| My hospital will support me once I get infected | – | – | – | Fixed | 0.735 |
| Fit statistics | Chi-square (df) | X2/df | RMSEA | IFI | CFI |
| Model fit | 182.54(125) | 1.46 | 0.070 | 0.903 | 0.900 |
Source: Field Data (2021).
CR: composite reliability; alpha (a): Cronbach’s alpha; AVE: average variance extracted; DF: degree of freedom; RMSEA: root mean square error of approximation; CFI: comparative fit index; IFI: incremental fit index were reported.
Descriptive results—coping mechanisms adopted by frontline personnel.
| Items | Min | Max | Mean | SD |
|---|---|---|---|---|
| 1. Personal preventative measures | ||||
| I follow strict protective measures such as hand washing, alcohol-based hand sanitizers, use of a face mask, and or protective clothing. | 3.00 | 5.00 | 4.65 | 0.50 |
| I observe social distancing protocols | 2.00 | 5.00 | 4.34 | 0.68 |
| I am taking zinc and vitamin C supplements to boost my immunity | 1.00 | 5.00 | 3.55 | 1.24 |
| I employ healthier lifestyles such as eating a healthy diet and exercising to boost my immunity | 1.00 | 5.00 | 3.88 | 1.05 |
| Overall | 2.50 | 5.00 | 4.11 | 0.64 |
| 2. Seeking external expert support | ||||
| I talk to religious leaders more often than I used to and pray more often | 1.00 | 5.00 | 2.87 | 1.22 |
| I seek help from a psychologist | 1.00 | 5.00 | 2.67 | 1.20 |
| I avoid media news about COVID-19 and related deaths | 1.00 | 5.00 | 2.34 | 1.24 |
| Overall | 1.00 | 5.00 | 2.63 | 0.92 |
| 3. Mitigating factors/institutional support | ||||
| My hospital provides me with the necessary PPE | 1.00 | 5.00 | 4.17 | 0.83 |
| The government tax waiver and insurance is a big incentive | 1.00 | 5.00 | 2.74 | 1.41 |
| My hospital will support me once I get infected | 1.00 | 5.00 | 3.19 | 1.25 |
| Overall | 1.00 | 5.00 | 3.37 | 0.88 |
Source: Field Data (2021).
Authors Contribution
Isaac Akanko (MD, male) and Patience Aseweh Abor (PhD, female) contributed to the conceptualization of the study. Isaac Akanko undertook the literature review, collected the data, and performed the analysis. Patience Aseweh Abor supervised the study. All the authors contributed to writing different sections of the manuscript. Carlos Kokuvi Tetteh (PhD student, male) and Patience Aseweh Abor significantly revised all sections of the study. Isaac Akanko was a MSc. Health Service Management student supervised by Patience Aseweh Abor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical clearance for the study was sought and granted from the Ghana Health Service Ethics Review Committee (GHS ERC) and respective medical facilities such as the 37 Military Hospital. A protocol ID number (37MH-1RB/MAS/IPN/510/2021) was assigned and subsequently given ethical approval by GHS ERC. Data collected were kept confidential and under lock with only the research team and the ethics committee had access to it. The risk involved in participating in this study was the loss of time during the interview.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.