
Abstract
Pericardial cysts are rare benign intrathoracic lesions, and calcified pericardial cysts are even more uncommon. Most pericardial cysts are asymptomatic, but patients may present with chest pain, dyspnea and any complications of pericardial effusion. We present a case of a left-sided calcified pericardial cyst, highlighting its rarity and symptoms in relation to its location.
Introduction
Pericardial cysts are rare intrathoracic lesions and usually form as a result of abnormal fusion of mesenchymal lacunae during embryogenesis, though cases have been documented following traumatic insult as well. 1 The incidence rate is about one in every 100,000 people. 2 They are most commonly found in the right cardio-phrenic angle. 3 The presence of a pericardial cyst in this common or, less frequently, unusual location presents a diagnostic challenge in distinguishing it from other intracardiac or mediastinal abnormalities.
The majority of pericardial cysts (>50%) are asymptomatic and have a relatively harmless natural course. Symptoms usually appear when the cyst compresses a nearby structure or undergoes complications.4,5 Here, we present an unusual case of calcified pericardial cyst who presented with presyncope.
Case presentation
A 50-year-old man, non-diabetic, and a nonsmoker, presented to our hospital with a long-standing history of dizziness and recurrent presyncope attacks without any significant past medical history. The initial symptoms started 2 years back, but for the last 6 months, the frequency increased. Presyncope was usually associated with heavy physical activity and occurred several times, but there was no loss of consciousness.
The body built of the patient was average. Physical examination, including cardiopulmonary examination, was unremarkable except for a few fine crepitations in the left lower chest. Routine blood tests, including echocardiogram, were normal. A routine chest Xray (Figure 1) was performed that showed a homogenous density mass with peripheral calcification along the left border of the heart. Echocardiography suggested an extracardiac nonperfused mass around the aorto-pulmonary window and left ventricle without any features of outflow obstruction. Chest X-ray showing rounded mass along the left border of the heart.
The tumor was further characterized by a contrast-enhanced thoracic computed tomography (Figure 2) as having a thick fluid inside and a calcified outer ring. The highest diameter was about 8.5 cm. Our main differential was teratoma while evaluating the patient. There was no pericardial effusion or any lymphadenopathy. Additional workout of presyncope including exercise tolerance test, 24 h Holter monitoring and CT scan of brain was normal. CECT scan demonstrates peripherally calcified mass around left side of the heart extending into left hemithorax.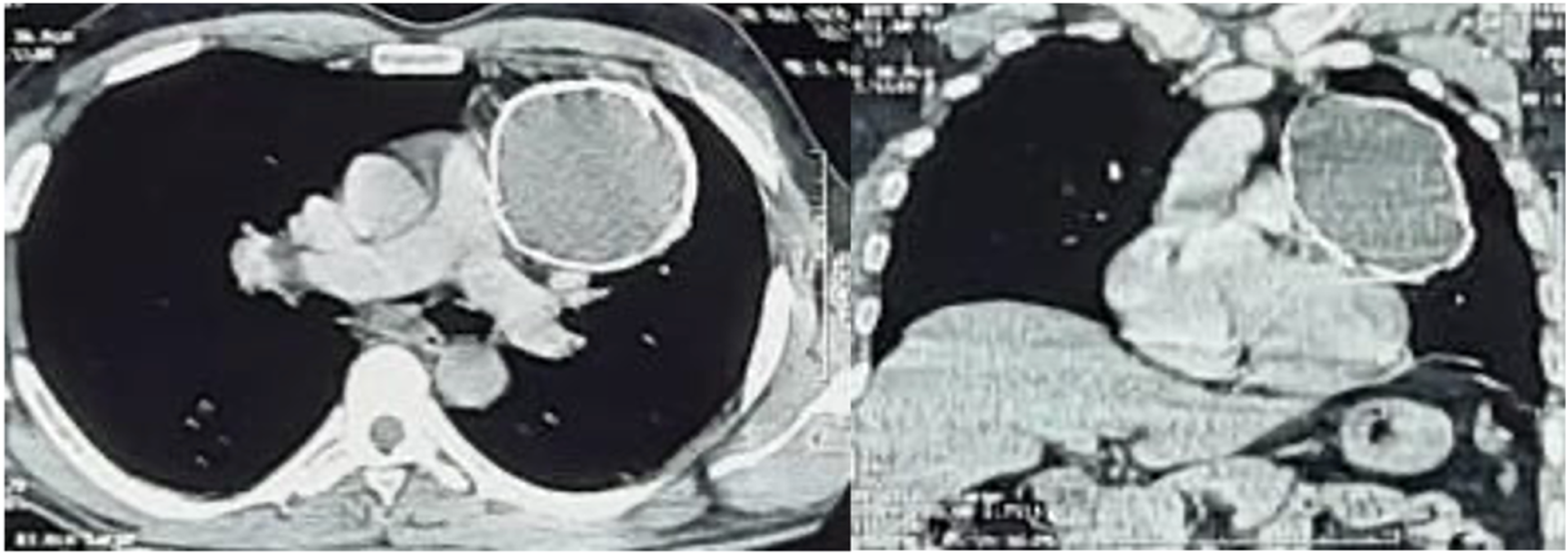
The patient underwent a left lateral thoracotomy, and mass was identified (Figure 3(a)) and removed. The mass was ovoid and firm in consistency that measures about 9 * 8 * 4.5 cm (Figure 3(b)) with a weight of 207 gm. The outer rim was calcified and it was filled with whitish thick fluid. The postoperative period was uneventful and patient was discharged on the seventh postoperative day. (a) Operative view of the mass in the left hemithorax, (b) resected specimen of the mass.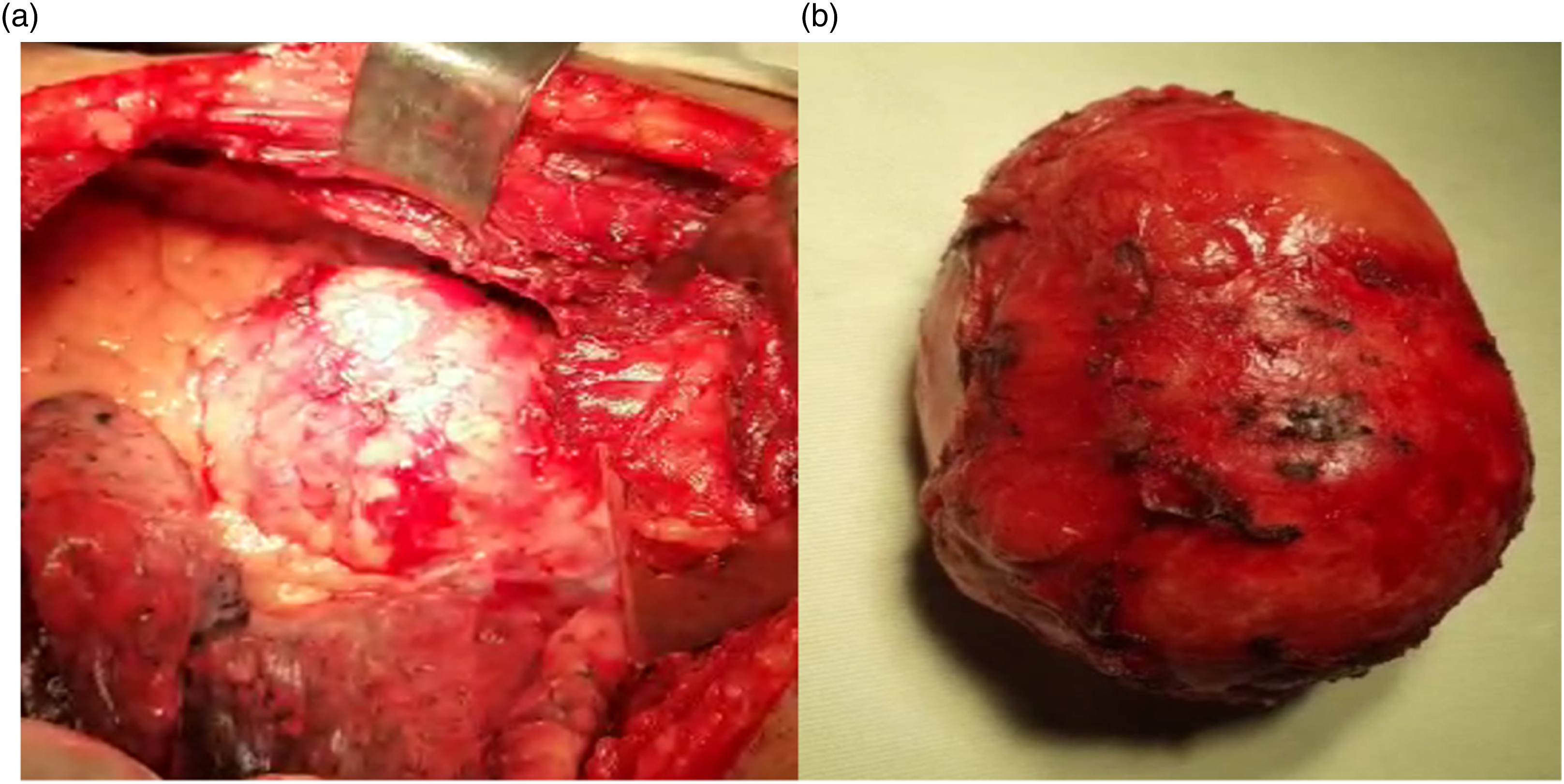
Histopathology report was consistent with pericardial cyst. And after 3 months of follow-up, patient’s initial symptoms were markedly resolved.
Discussion
Pericardial cysts are benign intrathoracic lesionsare very rare. Calcification of pericardial cysts is even more uncommon. Pericardial cysts frequently found at the right cardio-phrenic angle (51–70%) or left cardio-phrenic angle (28–38%), with a rare occurrence (8–11%) appearing in other mediastinal regions away from the diaphragm. 6 They are usually congenital, but they can be post inflammatory or traumatic.
Histologically, these cysts have a single layer of mesothelial cells lining them, while the connective tissue wall is made up of collagen and elastic fibers. They are known as “spring water cysts” because they are made of a clear fluid. 7 Calcification of pericardial cyst is extremely rare as found in our case. The cause of calcification of a pericardial cyst remains unknown and may be related to chronic inflammation. In our case we found thick viscous material within the cyst which may be an evidence of chronic inflammation.
Although pericardial cysts are typically asymptomatic, they can cause symptoms when they compress nearby mediastinal structures, as in the case of our patient. Other symptoms are related to complications which include infection, haemorrhage or rupture. Frequent symptoms include dyspnea, a prolonged cough, syncope, and persistent atrial tachycardia. 8 Syncope or presyncope is thought to be due to exertional or positional compression of the heart and outflow tract. 9
A pericardial cyst diagnosis is usually diagnosed incidentally by chest radiography showing a mass along the heart. Once suspected on the chest X-ray, thoracic CT scan with intravenous contrast has been a commonly used to confirm the diagnosis. MRI and echocardiography also facilitate in the diagnosis of pericardial cyst. 10
Asymptomatic individuals with pericardial cyst are often treated conservatively, but symptomatic patients require surgical excision or percutaneous aspiration.7,10 An excellent alternative to open surgical removal of a pericardial cyst is minimally invasive thoracoscopic excision. Our patient underwent surgical excision due to his symptoms and associated calcification.
Conclusion
In conclusion, we can say our case emphasizes the significance of a cyst’s anatomical location and size in relation to its presenting symptoms, and a consideration of the rarity of calcification of pericardial cysts, a trait that renders surgery the only feasible course of treatment.
Footnotes
Acknowledgements
We would like to thank the patient who gave consent; entire department of Thoracic Surgery, National Institute of Diseases of the Chest and Hospital (NIDCH), and Dr Khairul Anam, Director of NIDCH, Dhaka, Bangladesh.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Permission was taken from the patient.
Informed consent
Written informed consent for publication has been obtained from the patient and copy has been stored
Contributorship
Mofizur Rahman Mia (MRM) was the chief of the unit, treating this patient and carried out the patient diagnosis and supervised the report writing. S M Tajdit Rahman (TRT) contributed to regular follow-up of the patient, data collection from the preoperative, intraoperative, and postoperative periods. Sanghita Banik Proma prepared the first draft.
Mohammad Anamul Haque (MAH) carried out regular patient care. MRM and MAH performed the surgical procedure. TRT completed proofreading and gave it a final form. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Data availability
All patient data have been stored and available to corresponding author.