
Abstract
Surgical resection is the first choice for treatment of a thymic carcinoid tumor and radiotherapy is often performed as adjuvant therapy. Here, we report a case of an unresectable and chemoresistant thymic carcinoid tumor that was treated successfully using standalone proton beam therapy (PBT). The patient was a 66-year-old woman in whom surgical resection of the tumor was impossible because of cardiac invasion. Therefore, chemotherapy was administered. However, the tumor grew to 15 cm in diameter and she developed severe superior vena cava (SVC) syndrome. She was referred to our hospital and received PBT at a dose of 74 GyE in 37 fractions. PBT was conducted without severe early toxicities. After PBT, the tumor mildly shrunk to 13 cm in diameter and SVC syndrome almost disappeared. Subsequently, the tumor has continued to decrease in size slowly over the last 2 years and late toxicities have not been observed. Our experience with this case suggests that PBT may be effective for an unresectable thymic carcinoid tumor.
Keywords
Introduction
Thymic carcinoid tumor is a rare entity worldwide.
1
3
The tumor has an aggressive biological phenotype with a tendency for invasion of adjacent structures, local recurrence, and distant hematogenous metastasis.4,5 Surgery is the treatment of choice when feasible, even if radical resection is not achieved. Postoperative radiotherapy may be useful in cases with incomplete resection.4,6 There are only a few reports of the use of radical radiotherapy for an unresectable thymic carcinoid tumor. Maurizio
We have previously shown that proton beam therapy (PBT) is an excellent method for high-dose irradiation of a tumor with a reduced dose to non-cancerous tissues.8–11 Here, we describe the first use of PBT for treatment of an unresectable giant thymic carcinoid tumor.
Case Report
A 66-year-old woman had a mediastinal tumor that was diagnosed as a thymic carcinoid tumor by biopsy. Metastasis had not occurred, but surgical resection was impossible because of invasion of surrounding organs including the heart, trachea and large vessels. Chemotherapy was administered for about 2 years, including 4 courses of cisplatin and etoposide, 3 courses of irinotecan, 3 months of octreotide, and 3 months of tegafur-gimeraciloteracil potassium, but the efficacy was limited and the tumor progressed slowly. At the first visit to our hospital the tumor size was 15 cm in diameter (Figure 1A). At that time, the patient developed severe superior vena cava (SVC) syndrome with dyspnea, facial edema, pleural effusion and mild heart failure, but without metastasis. PBT was immediately started for relief of symptoms.

A) Contrast computed tomography images at the first visit to our hospital. The tumor was 15 cm in diameter and had pressed against large vessels and caused superior vena cava syndrome with dyspnea, facial edema, pleural effusion and mild heart failure. B) The first irradiation field of proton beam therapy. The tumor volume was 1221 cc. The two yellow arrows indicate the beam direction. 100% = 2GyE.
Treatment planning computed tomographic (CT) images for PBT were taken at 5-mm intervals during the expiratory phase under a respiratory gating system (Anzai Medical Co., Tokyo, Japan).12,13 The clinical target volume (CTV) was defined as the iodine-enhanced area on the CT scan. An area of potential microscopic disease was not included because the irradiated area became too large. Proton beams ranging from 155 to 250 MeV generated through a linear accelerator and synchrotron (Probeat, Hitachi, Tokyo, Japan) were spread out and shaped with a ridge filter, double-scattering sheets, multileaf collimators, and a custom-made bolus to match the beams to the treatment-planning data. 14 The leaf margin was a minimum of 3 mm to avoid treatment-related toxicity (Figure 1B). Beams were synchronized with respiration and delivered in the expiratory phase, in which the tumor position was most stable and reproducible.12,13 In each treatment session, the positional relationship between the center of the irradiation field and the tumor was verified before irradiation with the patient lying in the treatment position, using a fluoroscopy unit attached to the treatment unit.
After 16 GyE in 8 fractions (4 to 5 fractions per week), the symptoms of SVC syndrome gradually improved. Four dose schedules were used for tumor shrinkage and taking into account the tolerance doses of critical organs: 36 GyE for tumor shrinkage, 52 GyE for tumor shrinkage at the tolerance doses of the trachea and spinal cord, 62 GyE at the tolerance dose of the esophagus, and 72 GyE at the tolerance dose of large vessels. At the end of PBT the maximum tumor size had shrunk slightly from 15 cm to 13 cm and the tumor volume had decreased from 1221 cc to 811 cc (Figure 2). Symptoms of SVC syndrome had almost disappeared and acute treatment-related toxicity was acceptable (grade 3 dermatitis, grade 3 esophagitis, grade 1 neutropenia; CTCAE v3.0). Subsequently the tumor has continued to decrease slowly over two years and symptoms of SVC syndrome have completely disappeared. Grade 3 or higher late toxicity has not been observed. The tumor is currently 10 cm in diameter and the patient has been followed up once every three months without any treatment.

Contrast computed tomography images at the end of proton beam therapy. The tumor was 13 cm in diameter and its volume had decreased to 811 cc.
Discussion
Surgery is the standard treatment for a thymic carcinoid tumor, with possible postoperative radiotherapy in cases with insufficient resection.4,6 Standard treatment has not been established for unresectable thymic carcinoid tumors. Chemotherapy and radiotherapy have been used, but the number of cases is too small to evaluate the efficacy. In our case, chemotherapy was ineffective and sufficient radiotherapy was difficult because of the low tolerance dose of surrounding organs.
We have previously shown that PBT can be used to avoid irradiation of surrounding organs compared to conventional radiotherapy,8–11 and we have used PBT in several cases that were difficult to treat using other approaches.15–18 A treatment plan for conventional radiotherapy in the current case using the same treatment planning CT as that used for PBT planning is shown in Figure 3. This verified that avoiding the spinal cord was difficult using oblique opposing portal irradiation. Therefore, the maximum dose of convention radiotherapy was restricted to the tolerance dose of the spinal cord. Additionally, conventional radiotherapy of 50 Gy in 25 fractions gives a V20 for the lung of 46.2% (an unacceptable dose to the lung) and a mean lung dose (MLD) of 2213 cGy. In contrast, PBT of 74 GyE in 37 fractions using the first irradiation field gives a V20 for the lung of about 30% and a MLD of 1644 cGy.
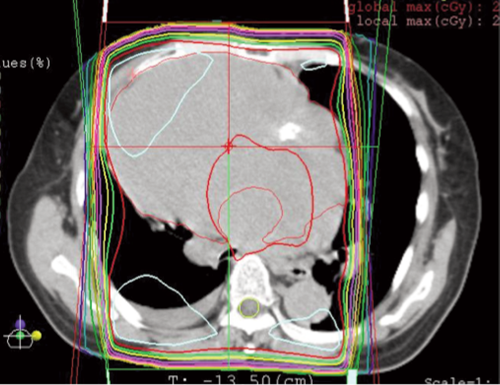
Conventional radiotherapy plan using the same treatment planning computed tomography. The treatment margin was set to give the same dose distribution covering the clinical target volume, compared to proton beam therapy. 100%=2 Gy. Avoiding the spinal cord is difficult and the dose to the lung (V20=46.2%, V30=37.6%, mean lung dose=2213 cGy) is not acceptable with irradiation at the tolerance dose of the spinal cord (50 Gy in 25 fractions) using this treatment plan.
The adequate dose to control a thymic carcinoid tumor is unclear.4–7 Maurizio
Conclusions
This case illustrates the successful use of proton beam therapy for an unresectable giant thymic carcinoid tumor that was difficult to treat with conventional radiotherapy. The excellent dose distribution of proton beam therapy has an advantage in treatment of patients with a large mediastinal tumor.
Funding
This work was supported in part by Grants-in-Aid for Scientific Research (B) (24390286), Challenging Exploratory Research (24659556), and Young Scientists (B) (25861064) from the Ministry of Education, Science, Sports and Culture of Japan.