
Abstract
Here we describe a case of open surgery for superior vena cava syndrome due to invasive thymoma. An 85-year-old woman presented with facial swelling and exertional dyspnea. Computed axial tomography revealed a thymoma in the mediastinum, extending to the superior vena cava, right atrium, and bilateral brachiocephalic veins. Endovascular therapy did not seem feasible because superior vena cava appeared totally occluded, and stenting could cause tumor embolism to the pulmonary arteries. Open surgery facilitated macroscopically complete and successful tumor resection. If long-term survival seems possible, open surgery could be a viable treatment option for superior vena cava syndrome that is ineligible for endovascular therapy.
Introduction
Superior vena cava (SVC) syndrome is caused by the obstruction or compression of SVC blood flow. In most cases, this is caused by lung or mediastinal tumors. Some tumor types causing SVC syndrome are sensitive to radiotherapy. However, tumors such as thymoma respond poorly to chemotherapy or radiation. 1 In such cases, endovascular treatment has been widely accepted as palliative treatment for severely symptomatic patients with malignant diseases. 2
As this is palliative therapy, patients need to undergo subsequent therapies to resolve the underlying disease. Open surgical treatment may be considered in patients with resectable tumors and in those who can endure the procedure.
We report a case of open surgical treatment of SVC syndrome due to invasive thymoma.
Case report
An 85-year-old woman with hypertension presented with facial swelling and dyspnea for a year. She was referred to our institution because of echocardiographic findings of tumors in right atrium (RA). Physical findings included swelling of the face and upper extremities. The soluble interleukin 2 receptor level was 468 U/mL, and laboratory results were, otherwise, unremarkable. Chest X-ray showed cardiomegaly with a cardiothoracic ratio of 54.2%. Electrocardiography showed a normal sinus rhythm of 83 bpm. Transthoracic echocardiography revealed two bundles of masses in RA with irregular margins. One bundle was mobile, whereas the other was immobile. Contrast-enhanced computed tomography revealed irregular marginated tumors in the mediastinum, SVC, RA, and left and right brachiocephalic veins (Figure 1(a) and (b)). Positron emission tomography showed an abnormal standardized uptake value of 5.37 in SVC and RA. Percutaneous intravenous biopsy revealed a thymoma. She was diagnosed with SVC syndrome due to invasive thymoma.

Preoperative enhanced computed tomography. (a) Two bundles of masses in the right atrium. (b) Irregular marginated tumor mass located in the mediastinum, superior vena cava, and bilateral brachiocephalic veins.
Because SVC appeared totally occluded, endovascular treatment appeared technically challenging, and stenting could cause tumor embolism to the pulmonary arteries. Moreover, the patient appeared strong enough to endure surgery. Thus, open surgery was selected with expectations of tumor resection and long-term survival. After induction of general anesthesia, the central venous pressure was 30 cmH2O. Through median sternotomy, the mediastinal tumor was resected. A cardiopulmonary bypass with aortic return and venous drainage via RA-IVC (inferior vena cava) was initiated, and total flow was obtained. The bilateral brachiocephalic veins were dissected, the tumors were excised with a 7-Fr Fogarty balloon catheter, and venous cannulas were inserted into them. The total flow was regained. The bilateral brachiocephalic veins were reconstructed with 14 mm ringed polytetrafluoroethylene grafts (GORE-TEX; W.L. Gore and Associates, Newark, DE, USA), and the venous cannula was reinserted through the grafts. The SVC and RA were incised, and two bundles of masses were observed in the free wall of the RA (Figure 2(a)). The tumors were excised en bloc, including from the SVC, RA, and left and right brachiocephalic veins. Entire tumor tissues were excised macroscopically. RA was reconstructed with bovine pericardium, and the bilateral brachiocephalic grafts were separately anastomosed to RA (Figure 2(b)).
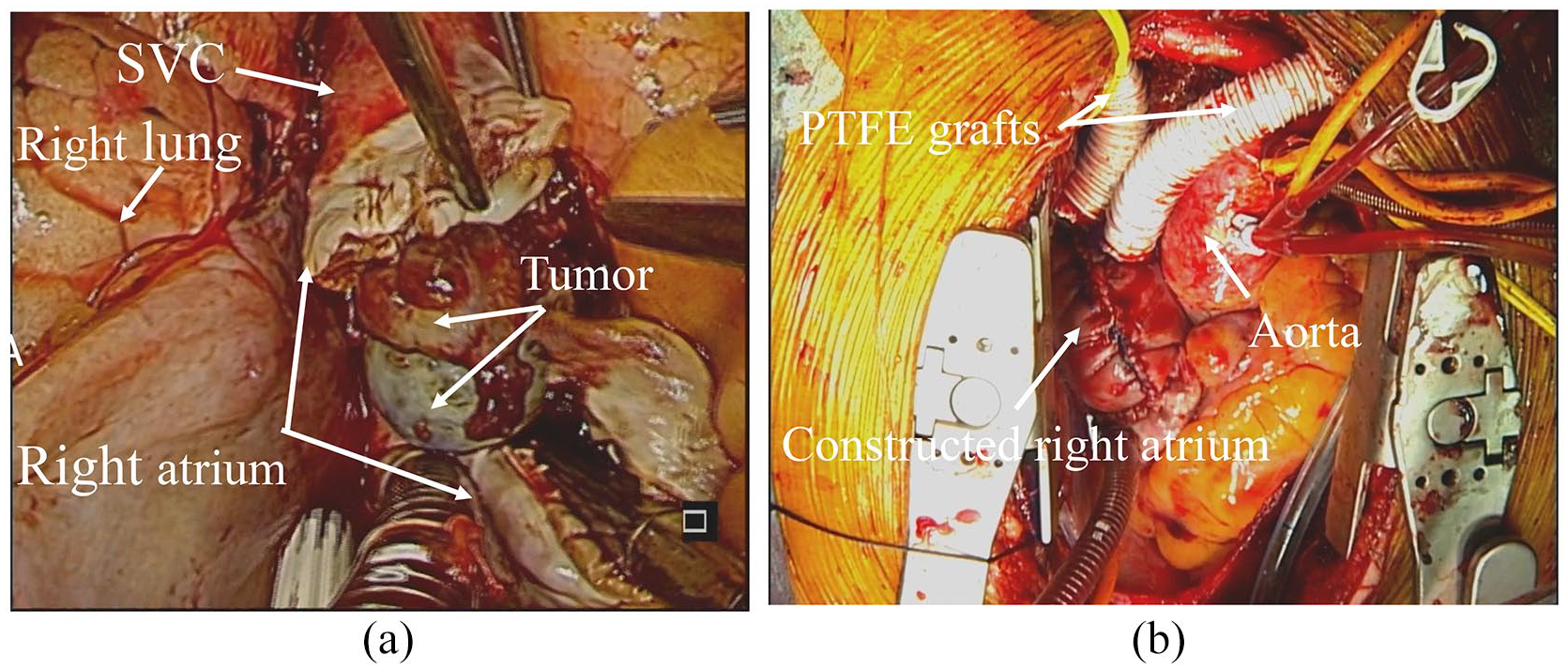
Operative findings. (a) Two bundles of masses in the right atrium. (b) The two separate polytetrafluoroethylene grafts were anastomosed to the right atrium reconstructed by bovine pericardium.
The central venous pressure decreased to 10 cmH2O. The pathological diagnosis was invasive thymoma, Masaoka stage IVA (Type B2), due to pleural and pericardial dissemination. On the first postoperative day, the patient was extubated. On the second postoperative day, she was able to resume her diet and received anticoagulation therapy with warfarin. Symptoms such as edema and dyspnea were relieved rapidly. On the 27th postoperative day, she was discharged. Postoperative radiotherapy/chemotherapy was not planned considering old age and possible adverse effects. Postoperative enhanced computed tomography revealed no residual tumors, and both grafts were patent. Anticoagulation therapy was maintained. The patient experienced recurrence, but has been regularly following up at our clinic for 4 years since the operation.
Discussion
Endovascular treatment for SVC syndrome has become the first line of treatment for severely symptomatic patients.3,4 However, open surgery treatment is effective when endovascular treatment is not anatomically suitable or when more durable long-term symptom relief is expected. 5
Thymomas are rare, indolent tumors, with no randomized studies regarding their management. Furthermore, few reports have included patients with advanced disease because thymic malignancies are rare. 6 Ströbl et al. 7 reported a worse prognosis in patients with Masaoka stage IV disease (10-year survival rate of 47%).
Surgery is widely performed for resectable thymoma, and multimodal therapy incorporating preoperative chemotherapy and postoperative radiotherapy is indicated for potentially resectable lesions, whereas radiotherapy/chemotherapy may be indicated for unresectable lesions. Modh et al. 6 reported that aggressive treatment involving chemotherapy, surgical resection, and postoperative radiation for advanced invasive thymic malignancies may improve survival.
In the present case, endovascular treatment seemed difficult because SVC appeared totally occluded and stenting could cause tumor embolism. Therefore, open tumor resection was planned despite advanced disease, and it was successfully performed with macroscopic excision of entire tumor tissues. Postoperative radiotherapy/chemotherapy was not planned considering possible adverse effects.
The optimal duration of anticoagulant therapy remains unclear, although Dartevelle et al. 8 recommended a 6-month treatment regimen with dicumarol (warfarin). At the time of writing this report, our patient was receiving warfarin for 4 years since the surgery, with the target PT-INR range set to 1.6–2.6 based on Japanese guidelines. 9
Although the sinus node was resected with RA and SVC during the surgery, an ectopic atrial rhythm was maintained postoperatively in our patient. In such cases, postoperative bradyarrhythmia can occur; therefore, temporary pacemaker lead placement should be considered.
Conclusion
Endovascular treatment is a viable treatment option for SVC syndrome in severely symptomatic patients. However, if tumors are resectable and long-term survival is expected, open surgery could be the better option.
Footnotes
Acknowledgements
The authors would like to thank Cactus for the English language review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This case was reported while adhering to the tenets of the World Medical Association Declaration of Helsinki. Submitted manuscripts conformed to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Meeting presentation
The contents of this article were presented at the 174th meeting of the Kanto Koushinetsu area in The Japanese Association for Thoracic Surgery (Niigata, Japan).