
Abstract
Purpose
Adrenocortical carcinoma (ACC) is a rare and highly aggressive malignant neoplasm, usually diagnosed in advanced stage. Role and efficacy of adjuvant radiotherapy has not been well defined. The objective of this study is to describe the various clinical characteristics and prognostic factors affecting the survival of ACC along with the role radiotherapy on overall survival and relapse free survival.
Methods
A retrospective analysis of 30 patients registered between 2007 and 2019 was carried out. The medical records containing clinical and treatment details were analysed. Data was analysed using SPSS 25.0. Survival curves were computed using Kaplan-Meier method. Univariate and multivariate analyses were performed to analyze the prognostic factors affecting the outcome. A p value of less than 0.05 was considered to be statistically significant.
Results
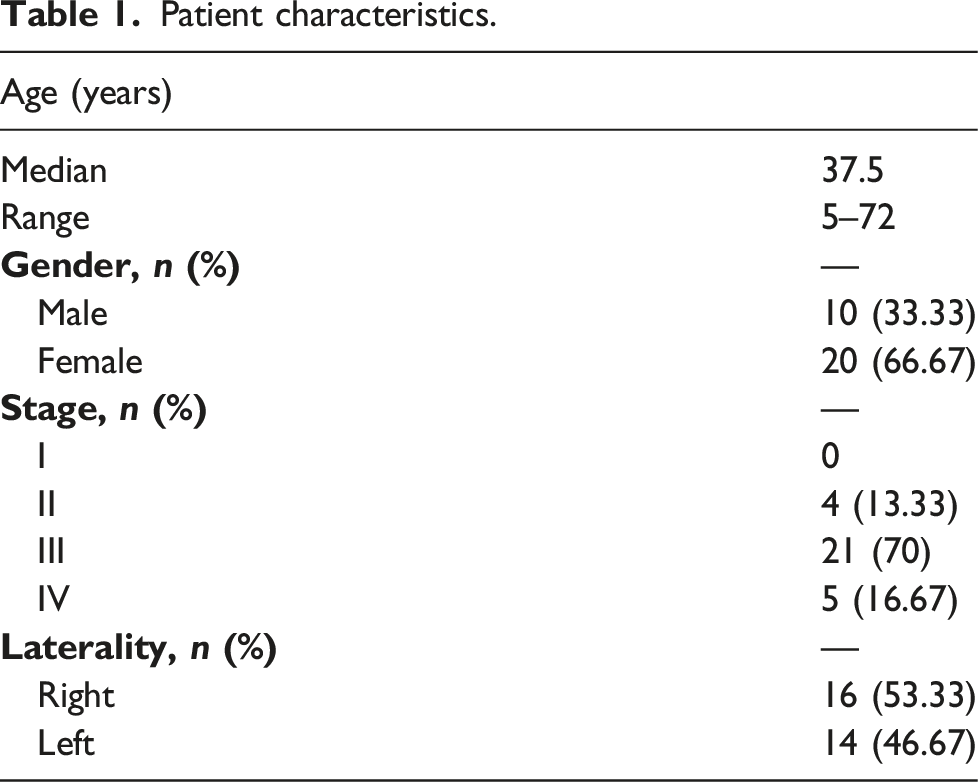
The median age of patients was 37.5 years (range, 5–72 years). 20 patients were females. Twenty-six patients had advanced stage (III/IV) disease while only four patients presented in early stage. Twenty-six patients underwent total adrenalectomy. Eighty three percent patients received adjuvant radiation therapy. The median follow up was 35.5 months (range, 7 monthss-132months). The estimated three- and 5-years overall survival (OS) was 67.2% and 23.3%, respectively. Capsular invasion and positive margins were the independent prognostic factors influencing both OS and relapse free survival (RFS). Out of 25 patients who received adjuvant radiation, only three patients had local relapse.
Conclusion
ACC is a rare and aggressive neoplasm with majority of patients presenting in advanced stage. Surgical resection with negative margins remains the mainstay of treatment. Capsular invasion and positive margins are independent prognostic factors for survival. Adjuvant radiation reduces the risk of local relapse and is well tolerated. Radiation can be used effectively in adjuvant and palliative settings in ACC.
Introduction
Adrenocortical carcinoma (ACC) is a rare and highly malignant tumor with incidence of 0.5–2 per million people per year with mortality accounting to 0.2% of all cancer related deaths globally.1-3 It is an aggressive malignancy with majority of the patients presenting in advanced stage. Locally advanced and metastatic stage (III/IV) accounts for almost 50% of total cases.4-6 Surgical resection remains the mainstay of treatment.7,8 The impact of surgical margin status on outcome in ACC is not clearly defined. In a multicentric database of 165 patients by Margonis et al., 9 median survival was 96.3 months for patients undergoing R0 resection as compared to 25.1 months for patients undergoing an R1 resection. Positive surgical margin status was associated with poor survival. However, in some studies, margin status did not influence overall survival (OS).10,11 Despite advancements in surgical techniques, the prognosis of ACC patients still remains guarded. Recurrence rates of as high as 85% have been reported in literature.12,13 This justifies the need for exploring effective adjuvant therapies to reduce the risk of relapse and improve survival. Due to rarity of ACC, there has been paucity of data evaluating the effect of adjuvant treatment on outcome of disease. There is dearth of quality evidence on use of adjuvant mitotane therapy and radiation therapy because of lack of prospective randomized trials. In a single centric large retrospective study of 391 patients of ACC by Else et al., 14 adjuvant mitotane therapy and radiation, improved relapse free survival (RFS), but failed to improve OS. The results have been mixed with some studies showing no improvements in RFS or OS with adjuvant mitotane and radiation.15,16 However, definitive data regarding the efficacy and indications of adjuvant systemic and radiation therapy have been missing and the benefits of adjuvant therapy remains controversial. In the past, ACC was considered radio-resistant entity. But the sample size in older studies undermining the role of radiation was very small, hence limiting the power of studies. With the advent of modern and precise techniques of radiation, the ability to deliver tumoricidal dose has been greatly enhanced. Recent studies have indicated significant improvement in OS and RFS with adjuvant radiation therapy.4,17,18 This study was undertaken to explore the potential prognostic factors, role of radiation and its impact on outcome in patients diagnosed with ACC.
Materials and methods
This retrospective study reviewed the medical records of 30 patients treated between 2007 and 2019 at a single regional cancer institute. All patients with histological proof of ACC were included in the study. Patients with incomplete medical records were not enrolled in the study. Patient charts were reviewed for demographic factors, treatment details including surgery, radiation therapy and chemotherapy details, pathological factors, TNM staging (American Joint Committee on Cancer), and treatment response. Patients were staged according to eighth edition of the TNM staging system. Pathological factors included tumor size, grade of tumor, mitotic index, Weiss score, margin status and capsular invasion. Detailed histopathological reports were examined to evaluate all these factors.
Adjuvant radiation was given in patients with margin positive disease, patients with tumor spillage at time of surgery, high grade disease and all stage III patients. For radiation treatment planning, contrast enhanced planning computed tomography (CT) was taken for all patients in supine position using a multislice CT scanner with a slice thickness of 2.5 mm (GE Healthcare Technologies). The images were then transferred to Eclipse TM treatment planning system (v8.6, Varian Associates). The dose of adjuvant radiation was 45 Gy in 25 fractions over 5 weeks and for palliative RT was 30 Gy in 10 fractions over 2 weeks. The clinical target volume (CTV) included tumor bed (which was delineated using preoperative CT films) and locoregional lymph nodes. The Planning target volume (PTV) was created by a 1-cm isotropic margin to CTV to account for setup and motion uncertainties. Radiation planning was done with three-dimensional conformal radiotherapy (3DCRT) in the initial years and evolved with time with later patients planned with volumetric modulated arc therapy (VMAT) with 6 MV photons.
Mitotane was given in adjuvant setting in patients with high risk of recurrence (capsular or vascular invasion, margin positive, large tumor size). The patients were started on dose of 500 mg thrice a day and gradually increased to 1 gram thrice a day. The main issues in compliance with Mitotane were the cost and unavailability of the drug.
Chemotherapy with EDP regimen was given to patients in stage IV or on relapse. The EDP regimen consisted of Etoposide 100 mg/m2 on days 2, 3 and 4, Doxorubicin 40 mg/m2 on day 1, and Cisplatin 40 mg/m2on days 3 and 4 given every four weeks.
Treatment response was evaluated for local and distant recurrence using RECIST scale (Response Evaluation Criteria in Solid Tumors). Complete response was defined for total disappearance of all target lesions; partial response was defined for 30% reduction in tumor size, 20% increase in tumor size being labelled as progressive disease while changes not meeting any of the above dimensions were deemed as stable disease.
Data analysis was done using Statistical Package for Social Sciences (SPSS) version 25.0. OS was defined as time from diagnosis till death or last follow up while RFS was defined as time from diagnosis till local/distant recurrence or last follow up. Patients were contacted to review the latest condition and imaging to calculate OS and RFS. Survival curves andrates were calculated using the Kaplan-Meier method. Univariate analysis for prognostic factors was done by log-rank test. Multivariate analysis was performed by Cox’s regression model. A p-value <0.05 was taken as statistically significant and variables with p < 0.05 on univariate analysis were selected for multivariate analysis.
Results
Patient characteristics.
Histopathological features.

Treatment and outcome
Treatment details.

The median follow up was 35.5 months (range, 7 months−132 months). In total, 17 patients experienced a relapse or progression of disease. Local failure alone was seen in three patients, local and distant relapse in five patients, and distant metastasis in nine patients. Most common site of distant metastasis was lungs (n = 7) followed by liver (n = 5) and bone (n = 2).
At the end of follow up, 16 patients (53.33%) were alive while 14 expired (46.67%). The 3-years OS and RFS was 67.2% and 45.4%, respectively while 5-years OS and RFS was 23.3% and 15%, respectively (Figures 1 and 2). Kaplan-Meier survival analysis curves showing overall survival (OS). Kaplan-Meier survival analysis curves showing relapse free survival (RFS).

Prognostic factors (univariate analysis).

Prognostic factors (multivariate analysis).

Three out of 25 patients who received adjuvant radiation developed local recurrence. Adjuvant radiation and Mitotane has not significantly affected the prognosis in terms of OS and RFS with non-significant p values.
Discussion
Due to the rarity of ACCs, a large-scale analysis for various prognostic factors and adjuvant therapies on patient outcome are difficult to conduct. This study demonstrates that despite multiple improvements in the diagnosis and treatment of solid malignancies over the past three decades, ACC continues to be a highly lethal malignancy with poor overall survival. This study represents the data from a single tertiary health care centre. The main finding of this study is that capsular invasion and positive margins results in a significant reduction in overall survival and enhances the risk of local recurrence in patients with ACC.
ACC can occur at any age and has bimodal age distribution with first peak in first decade and second peak in fourth and fifth decade. 19 Contrary to other studies, median age in our study was 37.5 years5,15,16 There was no bimodal age distribution. The other clinical characteristics reported in this study were comparable to other studies.5,13-16 ACC occurs with more frequency in females than in males as was seen in our study also.5,14,16 The effect of clinical characteristics on disease outcome in ACC is debatable.
Our data confirmed tumor stage, extent of resection, margin status and capsular invasion as established prognostic factors. Capsular invasion which is a pathological factor is an important prognostic marker for ACC. Though it has not been extensively studied in the past. We analysed the prognostic potential of this factor. We concluded that it significantly hampers the overall survival and relapse free survival. Similar to study by Kim et al., 20 presence of capsular invasion was independent prognostic factor for OS and RFS in our patient cohort. Therefore, it is pertinent to thoroughly examine the tumor capsule to rule out capsular and vascular invasion as these are associated with high risk of recurrence. Patients with capsular invasion has got poor survival with high chances of local recurrence.
Data on the use of adjuvant systemic therapy and radiation therapy has been mixed due to lack of prospective randomized trials. Due to the rarity of disease, the published studies have limitation of small sample size. In a study by Percarpio and Knowlton in 1976, it was observed that significant palliation was achieved with radiation in all patients. 21 Since then, various reports suggesting role of radiation in improving OS and RFS in ACC have been published. In a retrospective study by Fassnachtet al. 17 from the German ACC registry, 28 patients were recruited. Outcomes were compared between 14 patients who received adjuvant radiation and 14 patients who did not receive radiation and both the groups were matched for resection status, use of adjuvant mitotane, stage, and tumor size. Local recurrence occurred in two of 14 irradiated patients compared to 11 of 14 who did not receive radiation. Local RFS was significantly different between two groups but disease-free survival and OS were not significantly different. Similar conclusion was drawn by Sabolch et al. 4 who evaluated the effect of radiotherapy (adjuvant and definitive) on local control of ACC. Risk of local failure was 4.7 times more without use of radiation as compared with treatment regimens that included radiation. Thus, the authors concluded that radiotherapy should be considered in the adjuvant setting and highly recommended in advanced stage and larger tumor size. Improved local control after adjuvant radiation refuted the point that ACC is resistant to radiation. In our study, five patients who did not receive radiation witnessed recurrence within 1 year of diagnosis, whereas out of 25 patients who received radiation, only three had local relapse. Though the results were not significant for both OS and RFS, though this can be attributed to the small sample size in our study.
Adjuvant radiation is recommended in patients with high risk of local relapse such as incomplete resection, stage III, tumor spillage at time of surgery, large tumor size and high grade tumor. 22 With refinements in radiation therapy techniques, surrounding critical organs can be spared and adequate radiation dose can be safely delivered to tumor bed and locoregional lymph nodes. In our study, we administered 45 Gy as adjuvant radiotherapy to patients meeting above mentioned criteria. None of the patients in our series developed grade 3 or four toxicity and all patients tolerated treatment well without any breaks. Polat et al. 22 reviewed the published data and reported their experience and found that 52 (57%) of 91 patients benefitted from palliative radiation. In our series only one patient received palliative RT with 30 Gy and the palliation was achieved. Hence, radiation gives local control in adjuvant setting and relieves palliative symptoms in metastatic disease in ACC.
Margin status plays a vital role in the prognosis of ACC. Complete surgical resection with negative margins is the treatment of choice and co-relates with favourable prognosis. 3 R1 or R2 resection is an independent poor prognostic factor associated with worst OS of 20 and 15%, respectively. 3 Similar conclusion was drawn from our study. Survival was significantly worse in patients with margin positive disease as compared to patients with negative margins (p = 0.04) in the current report.
In a retrospective single centre study by Else et al., 14 adjuvant treatment with mitotane but not radiation significantly improved RFS without any effect on OS. When both the treatments are given in combination, these affect RFS, and radiation increases local tumor control by preventing tumor bed recurrence and therefore can reduce morbidity resulting from local relapses. Mitotane has been used in advanced and adjuvant settings with promising results. However, recurrence rate of 50% within 5 years have been observed even in patients who receive mitotane.23,24
The first randomized trial of adjuvant mitotane versus observation in patients at low-intermediate risk of recurrence (the Adjuvo study) failed to show any benefit with adjuvant mitotane in this group. The addition of adjuvant mitotane did not improve RFS or OS. The study demonstrated that patients with low-intermediate risk of recurrence have better prognosis with 5-years RFS of 75% and can be cured with surgery alone. 25
The study has limitations which are commonly seen in retrospective analyses, such as small sample size, heterogeneity of patient and stage characteristics and treatments. Owing to the rarity of this disease and the heterogeneous distribution of patient population, the absolute benefit of radiation has been underestimated. Furthermore, the evaluation of radiation therapy is complicated by differences in radiation technology and application. Radiation was given in majority of the patients and only 12% developed recurrence in the radiation group which is comparable to literature.14,22 Advancements in radiation techniques has enabled to deliver tumoricidal doses with sparing of the surrounding organs at risk; thereby improving the therapeutic ratio. Mitotane role as concomitant therapy was not explored in this study as most of the patients had financial constraints and compliance was not good due to cost issues and lack of availability of the drug. Adjuvant radiation is able to prevent local recurrence in most of the patients as documented in the current study also, although it remains to be demonstrated whether this translates into improved survival.
Conclusion
ACC is a relatively rare tumor with unfavourable prognosis and require multimodality treatment as most of the patients are diagnosed with advanced stage disease. Outcome of the disease is mainly driven by the resectability of the tumor and stage. Surgical resection with negative margins remains the mainstay of treatment. Recurrence is common despite complete surgical resection. Capsular invasion and positive margins were independent poor prognostic factors for survival in our study. Adjuvant radiation can be safely delivered and is an effective and safe therapy in controlling local recurrence as well as to palliate the symptoms in ACC. The study demonstrated that ACC is not a radioresistant entity and better local control can be attained with the addition of radiation in high-risk cases. With the latest advancements, radiation has a bigger role in adjuvant and metastatic setting in the multimodality treatment paradigm of ACC. However, prospective trials are needed to elucidate the effect of radiation on overall survival.
Footnotes
Author Contributions
All the authors had contributed for the conception & study design, data acquisition & interpretation, and drafting the article. All authors critically reviewed the manuscript for its content, contributed to the interpretation and presentation of the review, and approved the final version of the same before submission. Specific contributions by the authors individually have been highlighted below: Dr. Divya Khosla - conceptualization, study concepts and design, experimental studies/data analysis, treatment and follow-up of the patients, statistical analysis, manuscript preparation, and editing and was guarantor of integrity of the study. Dr. Rakesh Kapoor - literature research, treatment and follow-up of the patients and supervision. Dr. Aditya K Singla - data collection, literature research, manuscript preparation, and manuscript editing. Dr. Kannan Periasamy - literature research, manuscript editing, and supervision. Dr. Shikha Goyal - literature research, experimental studies/data analysis, and supervision. Dr. Renu Madan - conceptualization, manuscript preparation, and manuscript editing. Dr. Narendra Kumar - clinical studies, literature research. Dr Arunanshu Behera - treatment and follow-up of the patients, and approved the final version before submission. Dr Shrawan K Singh - treatment and follow-up of the patients, and approved the final version before submission. Dr Sanjay K Bhadada - manuscript editing and approved the final version before submission. Dr Rama Walia - manuscript editing and approved the final version before submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Retrospective clinical analysis and all authors have followed the principles outlined in the Declaration of Helsinki for all human experimental investigations. Approved from Institutional Ethics Committee.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.