
Abstract
Endometrial cancer (EC) is a disease with good and poor prognostic subtypes. Dedifferentiated endometrial carcinoma (DEC), undifferentiated endometrial carcinoma (UEC), and clear cell endometrial carcinoma (CEC) are rare high-grade tumors, associated with a poor prognosis and high pathologic stage. Many studies have been performed on the programmed death-ligand 1 (PD-L1) axis mainly focus on endometrioid adenocarcinomas and little research has been done on rare subtypes. The present body of work aims to evaluate the role of indoleamine-2,3-dioxygenase (IDO-1) and stromal differentiation (SD), their correlation with clinicopathologic features and overall survival. Here we found that positive IDO-1 expression in immune cells correlated with worse disease-free survival (p = 0.02), recurrence (p = 0.03), high pathologic tumor stage (p = 0.024), lymph node metastasis (p = 0.028), and myometrial invasion (p = 0.03). Our findings suggest IDO-1 to be relevant in both MMR intact and deficient tumors; however, >20% immune cell staining was restricted to MMR deficient cancers. For the stroma, immature, myxoid differentiation was found to correlate with worse disease-free survival (p = 0.04). We also found the correlation between IDO-1 expression and immature stroma. Looking forward, IDO-1 could be promising for immunotherapy and SD could be the answer to clinical heterogeneity.
Introduction
Endometrial cancer (EC) is the fourth most common malignancy in women, harboring a lifetime risk of approximately 3%. 1 The 5-year survival dropped to 84% in 2006, from 88% in 1975, 2 making EC the only cancer subtype to see an increase in patient mortality. Advanced stage and high-grade EC are lethal. There is significant heterogeneity in EC, characterized by a spectrum of histologic, and molecular findings. 3 The most common histologic subtype on EC is endometrioid, followed by serous carcinoma. 3
Undifferentiated endometrial carcinoma (UEC), dedifferentiated endometrial carcinoma (DEC) and clear cell endometrial carcinoma (CEC) are rare subtype EC which are under-studied, considered as high-grade tumors, and have an aggressive clinical behavior with poor prognostic outcomes. 4 UEC accounts for less than 9% of all cancers 5 and is termed DEC when associated with a better differentiating endometrial carcinoma component. CEC accounts for 2%–5.5% of EC cases. 6
Many studies have demonstrated the significance of programmed death-ligand 1 (PD-L1) expression in endometrial carcinomas subtypes.7,8 However, the tumoral microenvironment (TME) is complex with different cell lineages, cytokine mediators, and stroma components, and is not limited to the programmed death-ligand axis.
Tumor stroma was a relatively new concept which has been termed as “a wound that does not heal” by Flier et al. 9 His hypothesis was that the developing of tumoral stroma was similar to the immunobiological processes controlling wound response. 10 Since then, research has been focused on extracellular matrix (ECM), and different cellular components of the TME. A few studies have revealed stroma and tumor microenvironment and their clinical significances in cervix, breast, colon, and stomach cancers.11–15 Research has revealed the stroma differentiation to be correlated with poor overall prognosis, and believe it may be an optimal method to determine a tumor’s metastatic capacity. 16
Recently, studies have found that indoleamine-2,3-dioxygenase (IDO-1), an immune regulatory enzyme, can repress the T cell response and hinder the efficacy of immunotherapies. 17 IDO-1 has been shown as a negative prognostic signature in EC, 18 and the IDO1 enzyme inhibitor (Epacadostat) clinical trials have been shown to be well tolerated by cancer patients. 17
The present study is the first to evaluate IDO-1 and SD in the following rare subtype endometrial cancers: DEC, UEC, and CEC. Prior studies have evaluated SD in the uterine cervix, 13 but not in the uterine corpus. The role of immune check point inhibition is still somewhat ambivalent in EC and currently, the clinical significance of IDO-1 is not fully understood. Understanding the role of IDO-1 and SD in these rare subtype ECs may lead to better prognostication, improved therapies, and patient outcomes in a true clinical environment.
Materials and methods
Institutional Review Board
This study has been approved by Northwell Institutional Review Board committee from the Office of the Human Research (Northwell Health IRB#: 18-0890). Study methods were carried out in accordance with all relevant guidelines and regulations. Patient consent was waived by the institutional review board (IRB) committee due to the retrospective nature of this study
Study design
This study was retrospective in nature, and we selected only tissue specimens from procedures performed in our health system. We aimed for the largest possible sample size and selected a case selection interval of 17 years to facilitate this (2000–2017). Rare subtype endometrial carcinomas (DEC, UEC, CCC) were selected (Figure 1). We searched in the pathology database (Cerner Millennium) for specimens with keywords “clear cell carcinoma” and/or “uterine carcinoma with undifferentiated component” and/or “undifferentiated endometrial carcinoma” and/or “undifferentiated carcinoma with better differentiated components,” and cases were selected from the database consecutively. Cases lacking clinical information, appropriate follow-up, or tissue specimen availability were excluded. We did not deploy any other specific patient stratification or matching by stage of disease or age to avoid limiting our sample size.

Poor prognostic subtype endometrial carcinomas: (a) dedifferentiated endometrial carcinoma 2×, (b) dedifferentiated endometrial carcinoma 10×, (c) undifferentiated endometrial carcinoma 2×, (d) undifferentiated endometrial carcinoma 10×, (e) clear cell endometrial carcinoma 2×, and (f) clear cell endometrial carcinoma 10×.
All cases were reviewed by four observers (SH, DW, CJ, and MN) to confirm the diagnosis and to identify the best tumor-containing slide. Corresponding blocks were collected by the research coordinators under direction of the principal investigator. Further clinicopathological data was collected from the electronic medical records and patient follow-up data was collected from the New York State Cancer Registry Database (NYSCR) by the cancer registry group at Northwell Health.
The primary end point of this retrospective cohort analysis was to evaluate the role of IDO-1 and SD on disease-free survival, defined by the time to death, recurrence or second primary. The secondary end points of this study were to determine the relationship between IDO-1 expression and SD to the pathological and the clinical profile. In exploratory analyses IDO-1 expression and SD was compared to multiple variables including age, FIGO (International Federation of Gynecology and Obstetrics) stage, AJCC (American Joint Committee on Cancer) pathologic TNM stage, lymph node metastasis, cervical involvement, myometrial invasion, IDO-1/SD, mismatch repair (MMR) status, histology type, recurrence status, and survival status.
Slides were digitalized for the purpose of the study and were scanned on a Leica Aperio AT2 (Leica Biosystems, Buffalo Grove, Illinois, USA) whole slide scanner at 20×. Observers accessed digital slides through the Aperio vendor agnostic whole slide image viewer.
Immunohistochemistry
Formalin fixed, paraffin embedded tumor blocks were collected and cut at a 4-micron thickness. Staining was undertaken on a Ventana benchmark autostainer (Ventana Medical System, Tucson, Arizona). Immunohistochemistry (IHC) was performed with the following antibody clones for IDO-1 and MMR: IDO antibody (Vendor: Sigma Aldrich; Plarform: Ventana Ultra; Clone: polyclonal; Detection kit: Optiview DAB; Dilation: 1:2000), MLH-1 (Vendor: Ventana; Clone: M1, #790-5091; Detection kit: U OptiView DAB; Dilation: prediluted) MSH2 (Vendor: Ventana; Clone: G219-1129, #790-5093; Detection kit: U OptiView DAB; Dilation: prediluted), PMS2 (Vendor: Ventana; Clone A16-4, #790-5094; Detection kit: OptiView DAB IHC v6, Dilation: prediluted), and MSH6 (Vendor: Ventana; Clone SP93, #790-5094, Detection kit: U OptiView DAB IHC v6, Dilation: prediluted). Staining protocols were followed according and antibodies were pre-diluted by the manufacturer at the Immunopathology Laboratory of Long Island Jewish Medical Center (New Hyde Park, NY).
Biomarker expression
Staining was scored manually with consensus positivity between two observers (SH & MN) and IDO-1 IHC was scored within tumor cells (TC) and immune cells (IC) for percentage tissue involvement as shown in Figure 2. Cytoplasmic unequivocal staining of intensity above background was considered positive. MLH1, PMS2, MSH2, and MSH6 were scored in tumoral cells and considered intact (+) if >1% of tumor cells were positive. Negative staining was characterized by the absence of any detectable IHC staining, characterized by a pale gray discoloration in tumor and stromal components.

Indoleamine-2,3-dioxygenase expression in rare endometrial carcinomas: (a) tumoral IDO-1 expression (40×) and (b) tumoral IDO-1 expression (40×).
Stromal differentiation
A detailed, semi-quantitative approach was undertaken with particular attention to the invasive tumoral front. Stroma was scored on a three-tier grading system based on Hacking et al. 19 Fine, eosinophilic collagen fibers, often stratified into multiple layers were considered as mature stroma (SD1). Immature, myxoid SD was further divided into low-grade and high-grade stroma based on the degree of myxoid, basophilic-to-gray ECM. Low-grade stroma (SD2) contained a mosaic pattern of myxoid stroma and eosinophilic collagen fiber. Practically, low grade SD contained a minimum amount (40× field) of myxoid stroma. High-grade stroma (SD3) contained low variability in intensity between stromal matrix regions, with stromal cells surrounded by contiguous regions of myxoid stroma. In high-grade, immature (myxoid) stroma was the predominate stromal pattern (>50%) at the extramural tumor front (Figure 3).

Stromal differentiation in poor prognostic subtype endometrial carcinomas. Mature stroma (SD1) was composed of fine, eosinophilic collagen fibers, often stratified into multiple layers. Low-grade stroma (SD2) contained high variability in absolute difference in intensity between stromal matrix regions (mosaic pattern), with less contiguous areas of myxoid stroma. High-grade stroma (SD3) demonstrated low variability in absolute difference in intensity between stromal matrix regions, and stromal cells surrounded by contiguous regions of myxoid stroma: (a) mature stroma (2×), (b) mature stroma (10×), (c) low-grade stroma (2×), (d) low-grade stroma (10×), (e) high-grade stroma (2×), and (f) high-grade stroma (10×).
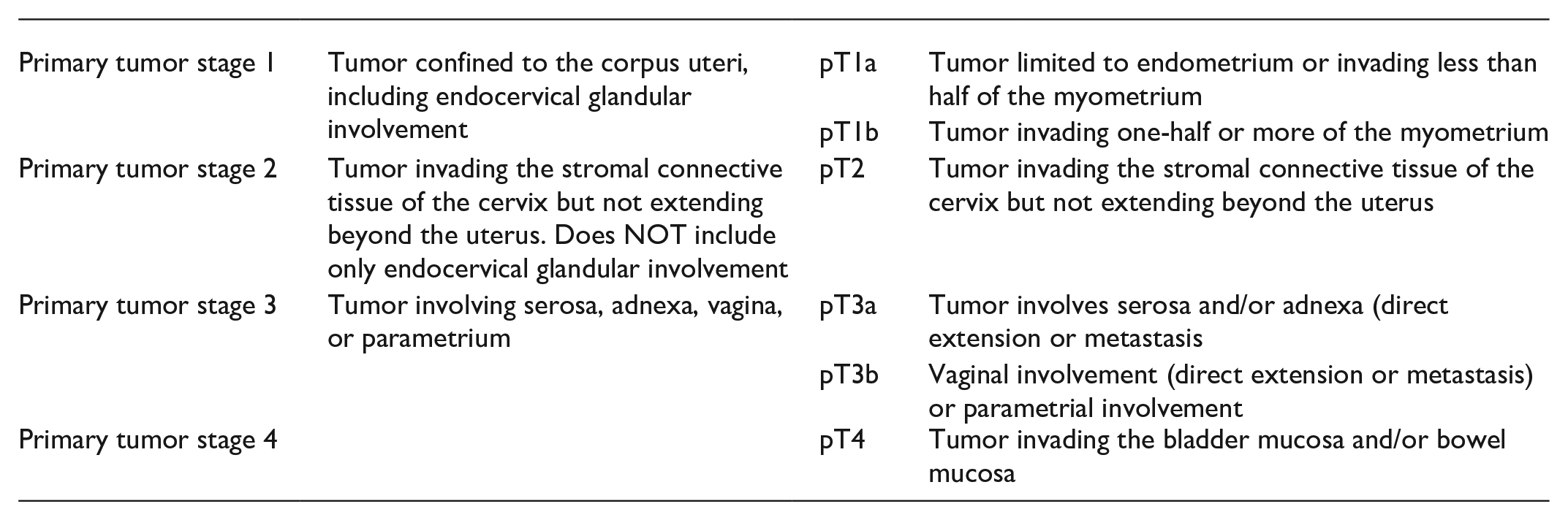
FIGO staging
Primary tumor stage was staged as per College of American Pathologists (CAP) protocol as following:
Lymph node was staged as following:

Distance metastasis was staged as following:

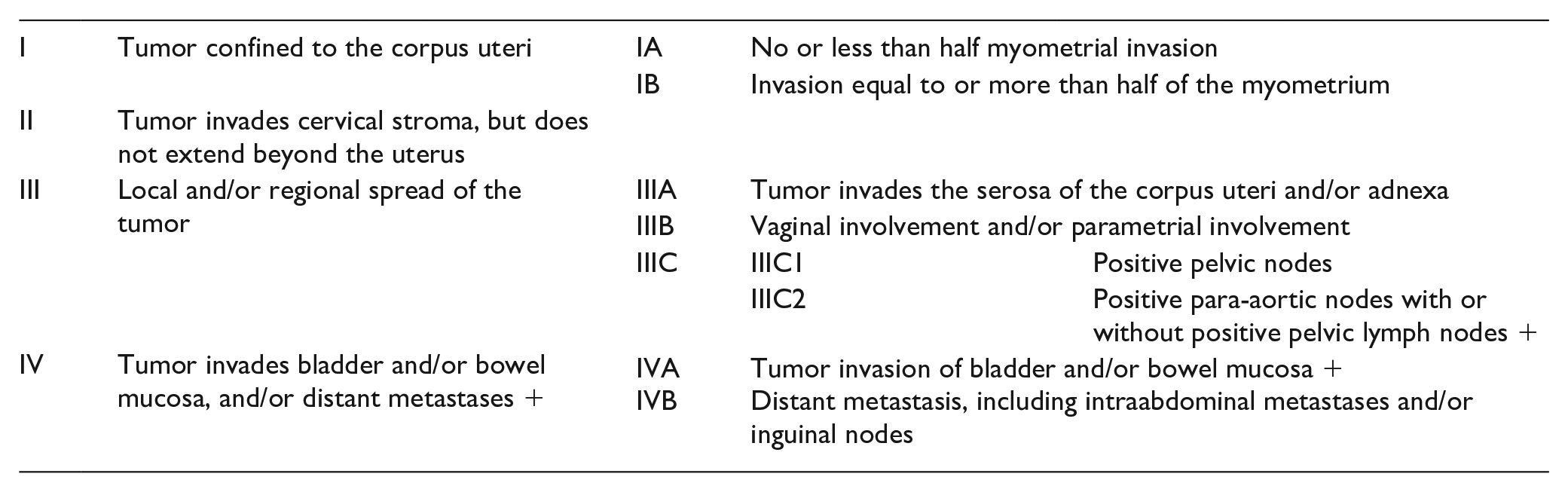
FIGO disease stages were classified based on the 2018 FIGO Cancer Report using the following criteria:
Statistical analysis
Descriptive statistics such as frequencies and percentages were calculated for the categorical variables. Non-linear regression was performed for IDO-1 expression and DFS. The log rank Kaplan–Meier method was used to evaluate DFS as a function of time. Cox-regression was performed to assess proportional hazard ratios (HR) between variables. The two tailed Fisher exact test was used to assess relationships between IDO-1, SD and the clinico-pathological profile. Statistical Analysis was performed using Prism graphpad 8.4.2 (San Diego, California, USA). A p value of <0.05 was used to indicate statistical significance.
Results
A total of 38 cases with available tissue blocks were used for immunohistochemical analysis. Out of 38 cases, 36 had undergone total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO). Two cases underwent biopsy only. 27 (74%) cases fell into the MMR intact cohort, while a total of 11 cases (26%) had MMR deficiency (Table 1). IDO-1 was common in our cohort. Thirty cases (79%) demonstrated immune cell staining ⩾1% and 16 cases (42%) demonstrated staining above the 5% threshold. In tumor cells, 24 cases (63%) demonstrated immune cell staining ⩾1% and 7 cases (18%) demonstrated staining above the 5%. Overall, 36 cases (95%) demonstrated >1% IDO-1 staining in either tumoral or immune cells, while 20 cases (53%) demonstrate IDO-1 staining >5% in either tumoral or immune cells. During follow-up, the two biopsy cases were included for the analysis of immunohistochemical expression with clinical findings and DFS, but not pathologic variables. Based on linear regression analysis of DFS, positivity for IDO-1 expression was determined to be 5% for tumor cells and 1% for immune cells (Figure 4). Based on the assessment of SD, cases were classified as follows: mature, 10 immature, low-grade, 16 and immature, high-grade. 8
Immunohistochemical expression compared to MMR status.

Indoleamine-2,3-Dioxygenase; TC: tumor cell; IC: immune cell; SD: stromal differentiation; MMR: mismatch repair.

Heatmap analysis and non-linear regression of indoleamine 2,3 dioxygenase expression: (a) non-linear regression of IDO-1 TC, (b) heatmap showing IDO TC and IC, and (c) non-linear regression of IDO-1 IC. IDO-1, Indoleamine 2,3 Dioxygenase.
Indoleamine-2,3-dioxygenase
For immune cells, IDO-1 expression was found to correlation with higher pathological tumor stage (p = 0.024), lymph node metastasis (p = 0.028), deeper myometrium invasion (p = 0.028), high grade SD (p = 0.02), and recurrence (p = 0.03) (Table 2). There was no statistically significant association for IDO-1 positivity and MMR deficiency; however, all the cases with immune stromal staining ⩾20% were found to be associate with MMR deficiency in our study. All remaining variables, including all of those associated with tumoral IDO-1 expression, were not found to have clinical significance (p > 0.05).
Indoleamine-2,3-dioxygenase and the clinico-pathological profile.

IDO-1: indoleamine-2,3-dioxygenase; FIGO: International Federation of Gynecology and Obstetrics; AJCC: American Joint Committee on Cancer; SD1: mature stroma; SD2: low grade immature stroma; SD3: high-grade immature stroma; MMR: mismatch repair.
Significant features (p ⩽ 0.05) are shown in bold.
Stromal differentiation
SD was broken up into mature (SD1), low grade (SD2), and high grade (SD3), as well as mature (SD1) and immature (SD2&3). When comparing the three grades separately, we found high grade immature stroma 3 to be associated with IDO-1 IC positivity (p = 0.001), which was also seen when low and high-grade immature SD cohorts were combined (p = 0.001). When low and high-grade stromal cohorts were combined, immature stroma was also found to correlate with higher FIGO stage (p = 0.03), higher pathological tumor stage (p = 0.001), lymph nodes metastasis (p = 0.001), cervical involvement (p = 0.01), deeper myometrium invasion (p = 0.001) and recurrence (p = 0.03). The remaining variables were not statistically significant (p > 0.05) and can be seen in Table 3.
Stromal differentiation and the clinico-pathological profile.

SD1: mature stroma; SD2: low grade immature stroma; SD3: high-grade immature stroma; FIGO: International Federation of Gynecology and Obstetrics; AJCC: American Joint Committee on Cancer; IDO-1: indoleamine-2,3-dioxygenase; MMR: mis-match repair.
Significant features (p ⩽ 0.05) are shown in bold.
Disease-free survival
Regarding Cox-regression of DFS, FIGO stage was found to be a poor prognostic factor on both univariate (p = 0.019) and multivariate analysis (p = 0.049). Pathological tumor stage was also found to be a poor prognostic factor on both univariate (p = 0.003) and multivariate analysis (p = 0.027). Positive IDO-1 staining in immune cells (>1%) was found to be a poor prognostic signature on univariate (p = 0.05) and multivariate analysis (p = 0.01). Similar prognostic pattern was also seen in SD on univariate (p = 0.007) and multivariate analysis (p = 0.018). The log rank method for Kaplan-Meier DFS analysis revealed IDO-1 IC positivity (p = 0.02), and SD combined (p = 0.04) to be poor prognostic signatures (Figure 5). The remaining clinico-pathological variables were not significant (p > 0.05) on Cox-proportional hazard regression analysis (Table 4).

Kaplan–Meier disease free survival analysis. IDO-1, indoleamine-2,3-dioxygenase; TC, tumor cell; IC, immune cell; Grade 1, mature stroma; Grade 2, low grade immature stroma; Grade 3, high-grade immature stroma: (a) survival analysis based on IDO-1 TC, (b) survival analysis based on IDO-1 IC, (c) survival analysis based on stroma grade, and (d) survival analysis based on stroma maturation.
Univariate and multivariate analyses of cancer free survival using the cox proportional-hazard regression.

HR: hazard ratio; CI: confidence interval; FIGO: International Federation of Gynecology and Obstetrics; AJCC: American Joint Committee on Cancer; SD1: mature stroma; SD2: low grade immature stroma; SD3: high-grade immature stroma; PT: stage; IDO-1: indoleamine-2,3-dioxygenase; MMR: mismatch repair.
Significant features (p ⩽ 0.05) are shown in bold.
Discussion
The present study is the first revealed the TME in rare EC, including the role of IDO-1 in IC and its relationship to SD. Here we demonstrated the expression of IDO-1 in immune cells and immature, myxoid stroma to have clinical significance in EC. We selected this cohort of rare, high-grade ECs because these tumors have limited treatment options currently and are seen to have uniformly poor outcomes.
We did not find a statistical association between IDO-1 positivity and MMR deficiency; however, immune cell staining >20% was exclusively seen with MMR deficiency in our study. This mirrors what was seen by Mills et al. 20 ; Clinically, a lower cutoff of 1% (IC) and 5% (TC) were used in our study based of linear regression analysis of DFS. Regarding IDO-1 expression in EC, different groups have published varying degrees of expression based on different cutoffs, from 18.1% to 60% (Table 5).18,20–23
Summary of IDO-1 expression found in endometrial carcinoma.

IDO-1: indoleamine-2,3-dioxygenase; MMR: mismatch repair.
Of clinical significance is the association for IDO-1 expression in ICs and worse DFS (p = 0.02). Here, too, we observed higher anatomical extent of disease in the form of pathological tumor stage, lymph node metastasis, deeper myometrium invasion; as well as immature SD, and recurrence to be associated with positive IDO-1 staining in immune cells. However, the expression of IDO-1 in TCs was not found to have clinical significance.
The effect of IDO-1 on clinicopathological features and recurrence may be important to support the targeting potential of IDO-1 as a therapeutic. Considering that IDO-1 expression was found to be associated with worse DFS, it is possible that poor prognostic EC patients could be excellent candidates for IDO-1 based immunotherapy. Some clinical trials have suggested Epacadostat, the best-in-class IDO-1 enzyme inhibitor, to be well tolerated by cancer patients. 17 Although a randomized phase III study (ECHO-301/KN-252) in metastatic melanoma was recently unsuccessful. 24 Despite this, many groups are still positive about resuming clinical development of compounds targeting the IDO-1 pathway, and still view it as an attractive target. 25
In recent years, a certain invasive pattern called microcystic, elongated and fragmented (MELF) 26 has been described. It is characterized by a distinctive fibromyxoid stromal reaction and acute inflammation infiltrates surrounding the tumor invasive front. This pattern was found to be associated with higher rate of lymphovascular invasion and lymph node metastases, more commonly in low grade endometrial carcinoma. This phenomenon may be better described by the process of SD. The clinical significance of fibromyxoid stroma and its association with survival length were not fully understood, although there was previous study Cao et al. 13 demonstrated immature stroma in 122 patients with cervix squamous cell carcinoma associated with poor prognosis.
The present study evaluated SD in rare tumors arising in the uterine corpus. We performed a similar approach as Hacking et al. 19 recently demonstrated in the paper of immature stroma in colorectal cancer.
Regarding the clinical profile, patients with immature stroma were found to be associated with higher FIGO stage (p = 0.03), pathological tumor stage (p = 0.001), lymph node metastasis (p = 0.001), cervical involvements (p = 0.01) and myometrium invasion (p = 0.001). Moreover, a higher propensity for recurrence (p = 0.01) was also found in our study, suggesting that these patients may benefit from more aggressive therapies.
Interestingly, along with worse DFS, low-grade immature SD was found to be associated with significant higher IDO-1 expression (p = 0.02). Meanwhile, the high-grade immature SD subset was exclusively positive for IDO-1 staining (n = 10), suggesting that these patients may be benefit hugely from IDO-1 based therapeutics and immune modulation. On the other hand, mature stromal differentiation was found to be protective in our patient cohort and had a higher percentage of negative staining.
The relationship between IDO-1 and the desmoplastic stroma (SD) is not well understood. Recent studies have revealed an abundant increase expression of colony-stimulated factor 1(CSF-1) in desmoplastic stroma in endometrioid adenocarcinoma. 27 The CSF-1 activates macrophages in tumor microenvironments. Meanwhile, several studies have shown IDO-1 is expressed by activated macrophages and natural-killer cells in the TME. IDO-1 increases the surrounding immune tolerance by acting as a suppressor to T cell immunity through the inhibition of effector T cell function and the induction of CD4 +, CD25 +, FOXp3+ Tregs. 28 Furthermore, Foxp3+ Tregs are commonly seen in the stroma at the tumor invasive front. This may explain the close relationship between IDO-1 expression and SD in our study, although more future studies need to be done to reveal the underlying molecular mechanism and to better understand its role in EC.
It is important to mention that there are several pitfalls to our study, and this was a retrospective study with the potential for selection bias. Secondly, due to the rarity of this cancer subtype, multi-institution collaboration will be important for larger study cohorts in future studies.
For patients with rare high-grade EC, the stroma is a brave new frontier, one which is rich in biologic diversity and detrimental for therapeutic decision making. 19 Although well-designed, robust clinical trials will be needed to prove this hypothesis, looking forward, we will need to think beyond PD-L1 and tumoral differentiation in EC.
Conclusion
In conclusion, our study revealed the prognostic factors of desmoplastic stroma and IDO-1 in rare, high-grade endometrial carcinoma (ECs). We found that immature desmoplastic stroma is associated with worse disease-free prognosis. We also found that high expression of IDO-1 in immune cells is associated with worse prognosis. The management of high-grade ECs are limited. Patients with high-grade ECs are usually associated with poor outcomes. Our study throw light on the new possible therapies for this population.
Footnotes
Acknowledgements
We thank Claudine Alexis and Kathy Quinn for their role as research coordinators.
Author contributions
MN, DW, and SH developed the theoretical formalism. SH, JC, and DW contributed to the acquisition of data. DW performed the analytic calculations and performed the numerical simulations. SH, DW, CJ, and MN contributed to the final version of the manuscript.
The authors report no conflicts of interest in this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by Northwell Institutional Review Board committee from the Office of the Human Research (Northwell Health IRB#: 18-0890). Study methods were carried out in accordance with all relevant guidelines and regulations.
Informed consent
Waived
Data availability
Pathology data and the statistical analyses for the current study are available from the corresponding author upon reasonable request.