
Abstract
Ampullary cancers are rare accounting for 0.2% of all gastrointestinal cancers. Signet ring is a rare variant of adenocarcinoma, characterized by having more than 50% of mucin secreting cells and clinically having a worse prognosis. We present the case of a teenage girl with this tumor, the youngest ever reported in medical literature. An 18 years old girl with no significant past medical history presented to our clinic with symptoms of upper abdominal pain and jaundice. Her upper GI endoscopy showed an ampullary lesion which was biopsied—diagnosing it as adenocarcinoma. She underwent a pancreato-duodenectomy (Whipple’s procedure) with Child’s reconstruction and a feeding jejunostomy. Her final histopathology report was documented as infiltrating adenocarcinoma of Signet Ring variety arising from the Ampulla of Vater. Being such a rare entity, there is a lack of randomized trials advising the optimum treatment for such cases. Till then anecdotal experiences will drive the optimum management of this rare disease.
Introduction
Ampullary cancers are rare accounting for 0.2% of all gastrointestinal cancers. Majority being adenocarcinomas, other varieties include papillary, Adenosquamous, and Mucinous. Histologically they are defined as being intestinal or Pancreatobiliary in origin. Signet ring is a rare variant of adenocarcinoma, characterized by having more than 50% of mucin secreting cells and clinically having a worse prognosis. We present the case of a teenage girl with this tumor, the youngest ever reported in medical literature.
Case
An 18 years old girl with no significant past medical history presented to our clinic with symptoms of upper abdominal pain and jaundice. Her ultrasound showed significant intrahepatic biliary dilatation. Her upper GI endoscopy showed an ampullary lesion which was biopsied—diagnosing it as adenocarcinoma. On further probing it was found that her mother had also developed duodenal cancer few years ago, however she couldn’t get any treatment and succumbed to the disease. On abdominal CAT scan the lesion was resectable and the decision was taken to operate her after discussion in the Institutional Tumor Board. She underwent a pancreato-duodenectomy (Whipple’s procedure) with Child’s reconstruction and a feeding jejunostomy. Her postoperative course was uneventful and she was discharged home on sixth POD. Her final histopathology report was documented as infiltrating adenocarcinoma of Signet Ring variety arising from the Ampulla of Vater (Figure 1). Size of lesion was 2.5 cm by 0.9 cm, margins clear and 0 out of 17 nodes were involved. The patient was advised Adjuvant Chemotherapy but not complied upon. She was lost to follow up and returned 8 months later with a large abdominal mass—biopsy proved it as metastatic adenocarcinoma of signet ring variety, confirming it to be recurrence of the Ampullary Carcinoma. She was put on Chemotherapy with palliative intent as the recurrent mass was surgically irresectable (Figure 2). After three cycles of Gemcitabine and 5 FU, she did not respond to the therapy.

Biopsy of Surgical specimen. Signet ring cells on high magnification (poorly cohesive cells with central vacuoles containing intracytoplasmic mucin.

Large abdominal mass.
Discussion
Also known as poorly cohesive type—Signet ring cell cancer demonstrates characteristic signet-ring cells with intracytoplasmic mucin and typical eccentrically located, crescent shaped nuclei (Figure 3). Most commonly found in the stomach, signet ring variety of the ampulla is an unusual and aggressive variant with only a handful of cases being reported in the literature (Table 1). Gardner et al. 1 was the first one to report SRCC as a variant of adenocarcinoma in 1990. Since then only 38 cases have been reported in the medical literature most of them being ages 40 and above. 2 Twenty-one of them were males and 19 females. The youngest reported was 32 years old female by Purohit et al. in 2005 3 and the oldest being 82 years old female by Ushida et al. 4 in 2017. The average age at presentation was 59 years. Our case is strange because this is the only case of such a tumor in a teenager. The largest case series has been published by Wen et al. 5 who reported eight cases from a single institution in Hangzhou, China. Adenocarcinoma arising from the Ampulla of Vater is unusual owing to the presence of three different types of epithelial cell linings there—intestinal, pancreatic, and Biliary. There is no consensus on the origin of Signet ring cell cancers. Blundell et al. 6 hypothesized that these originate from neuroendocrine cells in the gastric mucosa causing metaplasia. However, Wen et al. 5 from his study has proposed classification into four different types I, PB, gastric, and mixed. They also observed that presence of gastric mucosa or neuroendocrine cells was not mandatory for SRCC thus negating Blundell. Expression of CK7, along with negativity for CK20, CDX-2, and MUC2 signifies pancreatobiliary type SRCC, and vice-versa.
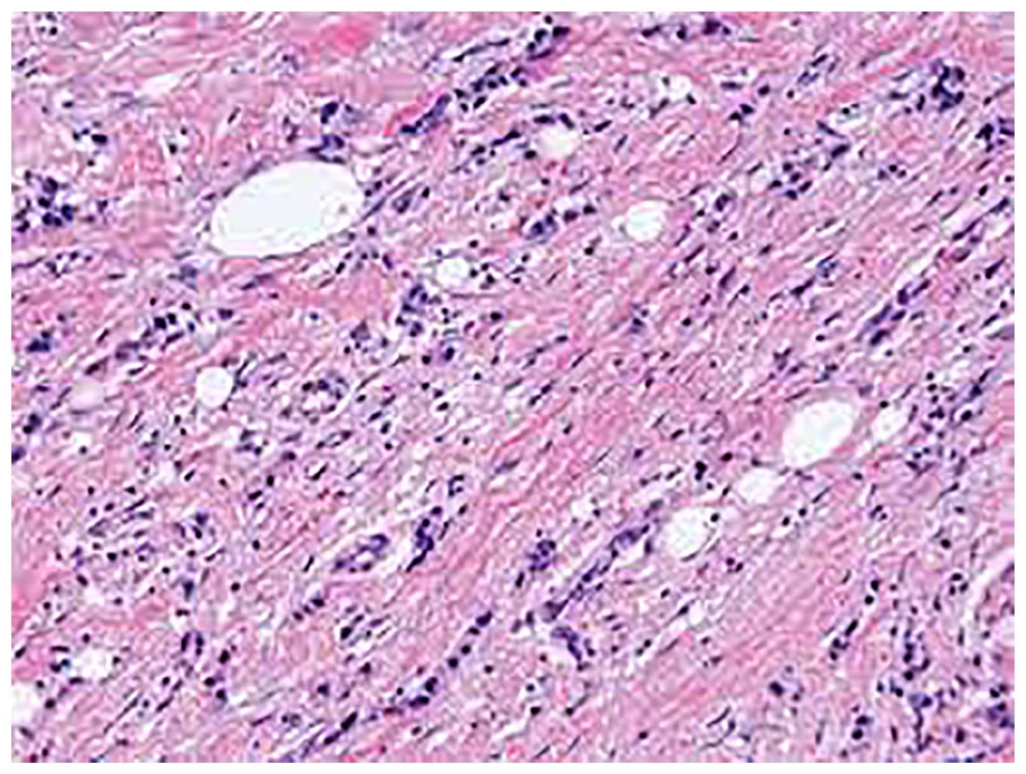
Signet ring cells—on Surgical specimen biopsy.
Reported Cases of Signet Ring Cell Cancer of Ampulla of Vater in Medical Literature.

Most of the ampullary cancers present early 2 as they cause obstruction to the biliary tract and the patient presents with obstructive jaundice. Not all ampullary cancers are obvious on the CAT scan. Those that are visible, have subtle findings of thickening and mass in some cases. Hence, Endoscopic Ultrasound is considered the gold standard to visualize and biopsy any ampullary lesion. Once the lesion has been confirmed and the biopsy shows dysplasia or invasive cancer, the cornerstone of treatment is surgery—Pancreaticoduodenectomy with reconstruction. Most of the cases reported in the literature did not have lymph node involvement, 2 just like the girl in our case. Only seven cases out of all the reported ones had Lymph node metastasis or N1 disease. 2 Patients like these have been offered adjuvant chemotherapy in some cases while some have just been observed. Being such a rare entity, there is a paucity of data on adjuvant treatment and no randomized trials to show any benefit.
Conclusions
Gardner et al. 1 was the first one to report SRCC as a variant of adenocarcinoma in 1990. The Dutch guidelines do not recommend any adjuvant therapy for completely resected ampullary cancer. 34 However the SRCC variety being more aggressive may need adjuvant therapy. Being such a rare entity, there is a lack of randomized trials advising the optimum treatment for such cases. Till then anecdotal experiences will drive the optimum management of this rare disease.
Footnotes
Author contributions
AAK drafted the initial manuscript. AJ and LS reviewed the final draft and helped in critical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Reporting of individual rare cases does not require Ethical Committee approval at our institute—cancer Foundation Hospital, Karachi.
Informed consent
Written and informed consent was Taken from patient and family.