
Abstract
Primary peritoneal serous carcinomas (PPSC) are exceedingly rare in male patients. Only a few cases were reported, and mostly with the limited immunophenotypical characterization. No molecular analysis of PPSC in males has been previously performed. We here describe another case of PPSC in a male patient. A comprehensive molecular analysis of the tumor revealed SF3B1 gene mutation as a possible driver.
Introduction
Primary peritoneal serous carcinoma (PPSC) is a rare malignancy with exceedingly low prevalence in male patients. The male:female ratio ranges from 0.0018 to 0.0045. 1 The first case of PPSC was described by Swerdlow in 1959 as “papillary tumor with psammoma bodies resembling ovarian carcinoma . . . arising from the pelvic peritoneum.” 2 Since then, PPSC has been increasingly recognized as a distinct histopathological entity and the tumor is classified in the same manner as its ovarian counterpart as low and high-grade serous carcinoma.3–5 In the absence of ovarian primary, it is likely that serous carcinomas develop from the epithelium of so called “secondary Mullerian system.” 3 To our knowledge, there are only four cases of PPSC in males previously reported in English literature.6–9 In this publication, we aim to present the fifth case of PPSC in a male patient with molecular analysis of the tumor for the common mutations known to be associated with serous type carcinomas.
Case report
We present a case of a 59-year-old asymptomatic non-smoker male patient. He was previously diagnosed with a stage II (T2N0M0) anal cancer (October 2016) and treated with Nigro protocol. 10 Eight month later (June 2017), the patient underwent a CT scan at an outside hospital which showed omental thickening and ascites. Cytopathological analysis of the ascites fluid at the outside hospital revealed fragmented fibroadipose tissue with marked desmoplastic stroma, ducto-glandular structures lined by cuboidal and low columnar epithelium and rare psammoma bodies.
The subsequent diagnostic laparoscopy at our institution revealed about 2–3 L of ascites fluid and multiple peritoneal implants on various peritoneal surfaces, particularly overlying the bladder. There were some smaller discrete implants overlying different portions of the small bowel, its mesentery and right diaphragm. The implants were biopsied, and the microscopic examination showed multiple nests of medium-sized malignant tumor cells infiltrating fibroadipose stroma with characteristic retraction artifact. The tumor cells were organized in micropapillary pattern and showed moderate amount of cytoplasm and hyperchromatic nuclei. Numerous psammoma bodies were noted. The surrounding stroma had a prominent desmoplastic response (Figure 1). Immunohistochemistry showed strong staining for CK7, PAX8, BerEP4, IMP3, and focal patchy positivity for p53 (wild type). The tumor cells were negative for CK20, CK 5/6, WT1, calretinin, TTF-1, thyroglobulin, D2-40, mCEA, ER, PR, CDX2 (Figure 2). Ki67 index was estimated as 10%–15%. Morphologic and immunophenotypic characteristic of the tumor were suggestive of a low-grade serous papillary carcinoma of the Müllerian origin despite of the fact that the patient is male. Further clinical workup did not reveal other definitive site of origin and no additional abnormalities suggesting of its primary peritoneal origin.
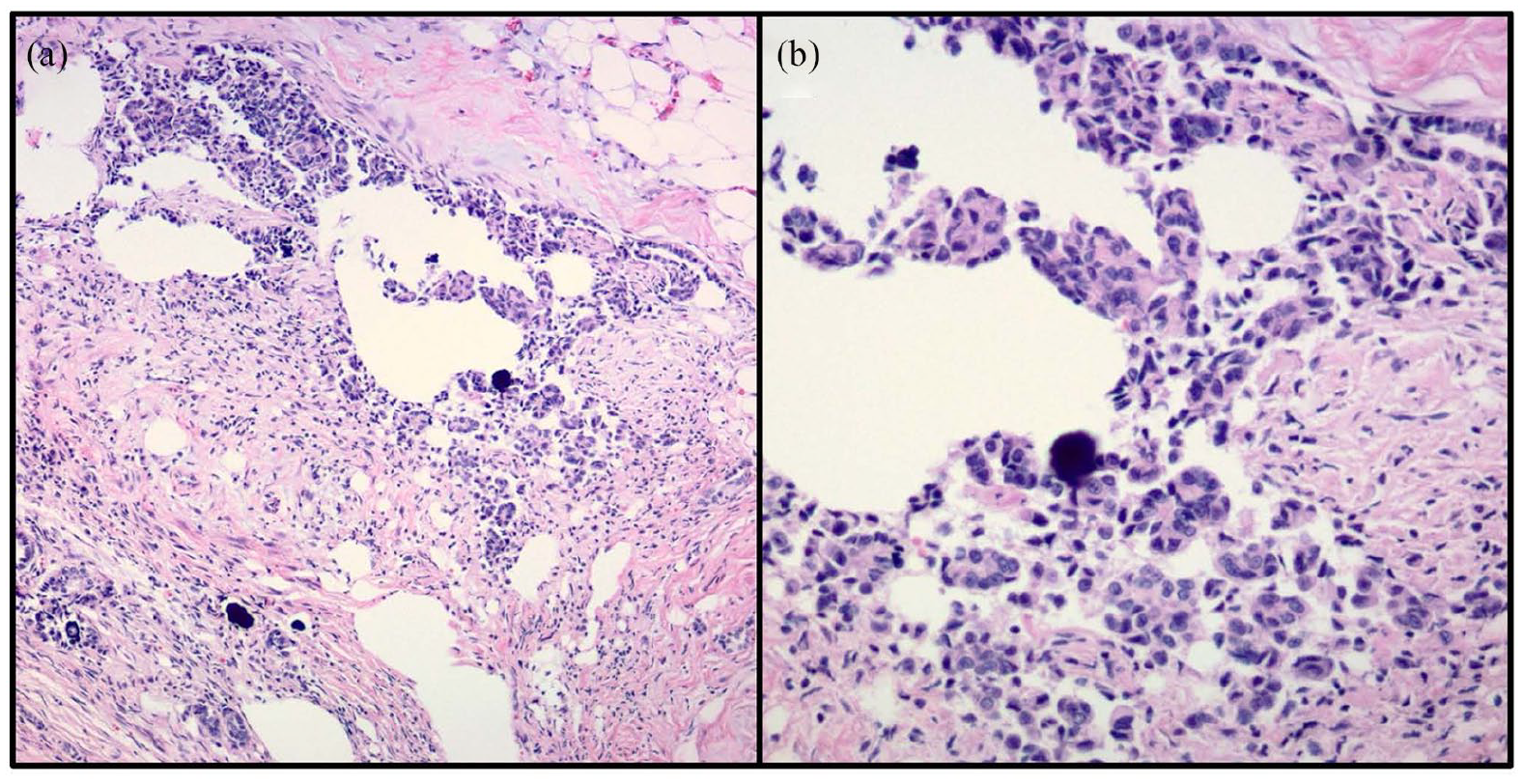
Hematoxylin-eosin stain demonstrating histological features of low grade serous carcinoma: (a) the tumor cells, organized in nests with micropapillary pattern and characteristic retraction artifacts. Psammoma bodies are noted (×100 magnification) and (b) low grade nuclear atypia in tumor cells seen on higher magnification (×400 magnification).
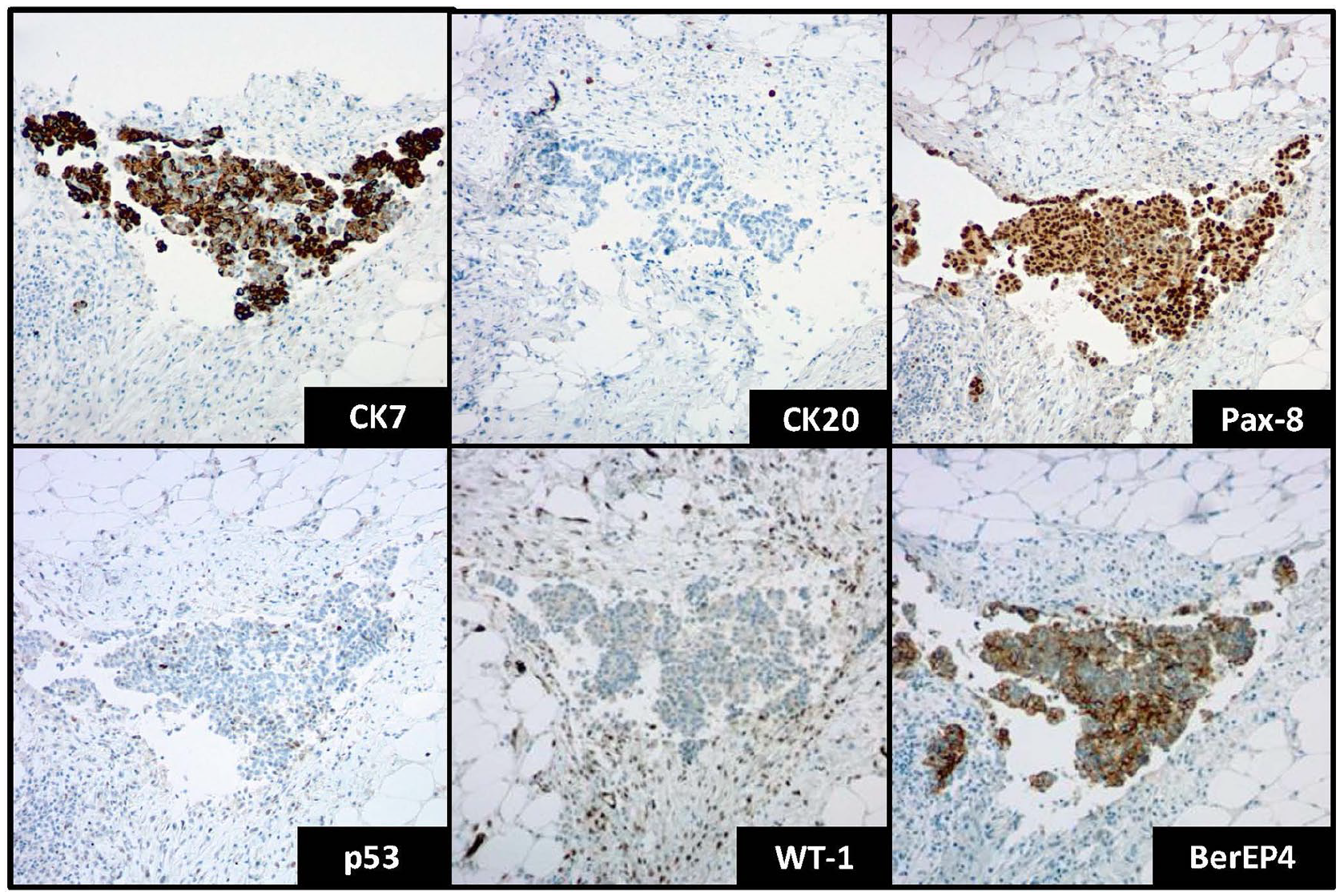
Selected immunohistochemical stains demonstrated in tumor cells. Positive staining for CK7, PAX8, BerEP4, and negative staining for CK20 and WT-1. Wild-type staining for p53 (×100 magnification).
Immunohistochemical studies showed no loss of mismatch repair proteins (MLH1, MSH2, MSH6, and PMS2). Tumor microdissection was done, and next generation sequencing studies were performed in September 2017 using Ion Cancer Panels (Thermo Fisher Scientific, Thermo Fisher Scientific Inc., Waltham, MA, USA) and amplicon sequencing was done based on manufacturers protocol. Molecular analysis revealed no copy number alterations. We identified pQ1228X stop codon mutation of SF3B1 gene of 7% of the tumor cells. Wild type variants of the following genes were identified: ABL1, AKT1, ALK, APC, ARID1A, ARID2, ATM, ATRX, BAX, BCL2L1, BRCA2, BRAF, BTG2, CCND1, CCND3, CCNE1, CDH1, CDKN1A, CDKN2A, CREBBP, CSF1R, CTNNB1, DAXX, DCC, E2F3/SOX4, EGFR, ELF3, EP300, EPC1, ERBB1, ERBB2, ERBB3, ERBB4, ERCC2, EZH2, FANCA, FAT4, FBXW7, FGFR1, FGFR2, FGFR3, FLT3, FOXA1, FOXQ1, GNA11, GNAQ, GNAS, HNF1A, HRAS, IDH1, IDH2, JAK2, JAK3, KDM6A, KDR, KIT, KLF5, KMT2A, KRAS, LKB1, LRP1B, MAGEA6, MAP2K4, MAPK8IP3, MCL1 MDM2, MEN1, MET, MLH1, MLL1, MLL2, MLL3, MPL, MYC, MYCL1, NCOR1, NF1, NFE2L2, NOTCH1, NOTCH3, NPM1, NRAS, P24, PALB2, PAIP1, PDGFRA, PIK3CA, PIK3R1, PKD1, PPARG, PRSS1, PTEN, PTPN11, PVRL4, R2, RB1, RET, RHOA, RHOB, RICTOR, RXRA, SF3B1, SLC16A4, SMAD4, SMARCB1, SMO, SRC, STAG2, TERT, TGFBR1, TGFBR2, TSC1, TSC2, TP53, TXNIP, NALCN, VEGFR, YAP1, YMHAZ, ZFP36L1, ZIM2, ZNF703.
Three months later the patient developed tumor recurrences at the trochar sites from his laparoscopy and possible pleural metastasis. He had received two cycles of paclitaxel and carboplatin therapy. He is currently stable and awaiting additional course of chemotherapy.
Discussion
Developmental aspects of primary peritoneal serous carcinoma (PPSC) are not fully uncovered. Though infrequent, PPSC is considerably more common in female patients due to its presumable development from persistent peritoneal rests of Müllerian epithelium (“secondary Müllerian system”).3,11 One can speculate that male PPSC can also arise from the epithelial remnants that did not convolute during ontogenesis due to abnormal focal resistance to Müllerian inhibiting factor. Serosal surfaces of the testis is a known site for primary serous-type tumors in males and the origin of these anatomically related tumors remains unclear as well. Another exceedingly rare type Müllerian type tumor clear cell adenocarcinoma arising from persistent Müllerian duct has been previously reported in male genitourinary tract. 12
Diagnostic challenges of PPSC in male patients stem from the extreme rarity of the tumor. Diagnostic criteria for PPSC in males are not clear yet and presumably similar to those in PPSC in female patient. It is extremely important to rule out possible primary sites before a diagnosis of PPSC is rendered. PPSC in females share histopathological similarities with adnexal serous carcinomas and therefore can be divided into two distinguishable groups of low- and high-grade tumors.3,5 Most of the case reports of PPSC in males follow the same classification. 9 Table 1 summarizes all PPSC cases in male patients reported in English literature.
Summary of reported cases of primary peritoneal serous carcinomas in male patients.

CDX2: caudal type homeobox 2; CK: cytokeratin; D2-40: podoplanin; EMA: epithelial membrane antigen; ER: estrogen receptor; HMWK: highmolecular weight cytokeratin; IHC: immunohistochemistry; IMP3: insulin-like growth factor II messenger ribonucleic acid-binding protein 3; LMWK: low molecular weight cytokeratin; mCEA: monoclonal carcino-embryonic antigen; PAX8: paired box gene 8; PR: progesterone receptor; PSA: prostate specific antigen; TTF-1: thyroid transcription factor-1; WT: wild type; WT-1: Wilms tumor-1.
Morphologically, the tumors are represented by complex papillary architecture, varying cytological atypia and psammoma bodies. One of four published PPSC cases in males was not graded; two cases presented as high grade, but p53 stain was not performed. Limited immunophenotypical characterization of three cases did not completely rule out other possibilities. The most complete immunophenotypic analysis was done by Xu et al. 9 Our case of PPSC underwent a comprehensive immunohistological workup with positive PAX8 and wild-type p53 staining that was most consistent with low-grade serous carcinoma.
Differential diagnosis for PPSC in males would include malignant mesothelioma and non-Müllerian metastatic carcinomas that can share similar morphological features. A recent study indicated that PAX8 can be expressed both in benign and malignant mesothelial cells. 13 This study showed that the expression of PAX8 is significantly more common in female patients. Importantly, in male patients, no cases with diffuse PAX8 positive staining in mesothelial cells were reported. PAX8 is a very useful but not the single immunohistochemical marker that aids the diagnosis. Malignant mesothelioma is usually WT-1, calretinin and D2-40 positive. However, WT-1 cannot be reliably used for differential diagnosis as it was found to be positive in male PPSC. 9 Urothelial micropapillary carcinoma shows positive immunostaining for CK7, CK20, and uroplakin that were not seen in our case.
Molecular characteristics of ovarian serous carcinoma are well-studied. TP53 mutation is a hallmark of ovarian serous carcinomas and is found at significantly higher rate in high-grade tumors defining a distinct molecular pathway for the later. Additional molecular alterations include KRAS, BRAF, NRAS, MSH2 mutations in low-grade tumors and BRCA, BARD1, BRIP1, CHEK2, MRE11A, PALB2, RAD50, RAD51C mutations, MYC, CCNE1, NOTCH3 amplifications in high-grade carcinomas.14–16 PPSC in females is characterized by the similar molecular profile such as loss of heterozygosity at chromosomal loci and overexpression of HER2 and BRCA mutations (~40% cases).17,18 A whole exome sequencing of a single case of female high-grade PPSC showed BRCA1, BRCA2 mutations as well as TP53, ERBB2, EGFR, KRAS and other mutations commonly found in ovarian serous cell carcinomas. 19 Interestingly, retrospective search of a database with 2,673 PPSC cases (including only five male cases) found no association with germline mutations of BRCA in men with PPSC. 1 No molecular analysis was previously performed on male PPSC tumors. In our case, we did not find any common mutations associated with PPSC in females; however, it was positive for SF3B1 gene mutation that encodes subunit 1 of the splicing factor 3b protein complex. SF3B1 mutations are associated with aberrant pre-mRNA splicing and are frequently found in myelodysplastic syndrome (MDS), chronic lymphocytic leukemia and were also reported in ovarian serous carcinomas. 20 Although our patient has no known diagnosis of MDS, we cannot entirely exclude the presence of a clonal hematopoiesis of indeterminate potential that interferes with the results.
To our knowledge, this is the fifth published case of PPSC in male and first case with molecular analysis performed. While it is not possible based on one case to draw a solid conclusion on molecular profile of such tumors in males, similarities with ovarian type serous carcinomas may suggest same lineage. Further studies of male PPSCs with full immunohistochemical work-up and molecular analysis are needed to better understand the molecular pathogenesis and aid in the diagnosis of this rare entity.
Footnotes
Author contributions
Vladislav Makarenko wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
UMass Medical Center does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.