
Abstract
National virtual multidisciplinary team meetings have been established in Swedish cancer care in response to centralized treatment of rare cancers. Though national meetings grant access to a large multidisciplinary network, we hypothesized that video-based meetings may challenge participants’ contributions to the case discussions. We investigated participants’ views and used observational tools to assess contributions from various health professionals during the multidisciplinary team meetings. Data on participants’ views were collected using an electronic survey distributed to participants in six national multidisciplinary team meetings for rare cancers. Data from observations were obtained from the multidisciplinary team meetings for penile cancer, anal cancer, and vulvar cancer using the standardized observational tools Meeting Observational Tool and Metric of Decision-Making that assess multidisciplinary team meeting functionality and participants’ contributions to the case discussions. Participants overall rated the multidisciplinary team meetings favorably with high scores for development of individual competence and team competence. Lower scores applied to multidisciplinary team meeting technology, principles for communicating treatment recommendations, and guidelines for evaluating the meetings. Observational assessment resulted in high scores for case histories, leadership, and teamwork, whereas patient-centered care and involvement of care professionals received low scores. National virtual multidisciplinary team meetings are feasible and receive positive ratings by the participants. Case discussions cover medical perspectives well, whereas patient-centered aspects achieve less attention. Based on these findings, we discuss factors to consider to further improve treatment recommendations from national multidisciplinary team meetings.
Keywords
Introduction
Case discussions in multidisciplinary team meetings (MDTMs) represent a focal point of the patient trajectory. Based on all relevant information available, a multidisciplinary and multiprofessional team of experts consider treatment alternatives and provide treatment recommendations based on the best evidence available. MDTMs have been found to be particularly relevant and beneficial in complex cases, where multidisciplinary case discussions have been reported to alter the treatment recommendation in up to one-third of the cases.1–3 Benefits linked to MDTMs include better coordination of care, development of clinical skills, and adherence to evidence-based treatment recommendations.4–8 Rare cancers are, as a group, associated with multiple challenges including late and incorrect diagnosis, adverse outcomes, limited clinical expertise, weak evidence for best practice, and difficulties in collecting large series for research and in carrying out clinical trials. 9
In Sweden, with a population of 10 million, surgery and select oncologic treatments for rare cancers, during recent years, been centralized to national specialist centers. This development was motivated by needs related to equal access to high-quality care, adherence to national treatment guidelines, infrastructures for research, and patient access to clinical trials. Between 2015 and 2017, treatment for penile cancer, anal cancer, vulvar cancer, gastroesophageal cancer, hepatobiliary cancer, and cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) underwent such centralization. As part of this process, national virtual MDTMs were developed to grant high-quality expert opinion and coordinated treatment recommendations across geographical areas, and case discussion herein were made mandatory. In 2017, a national MDTM was also initiated for childhood cancer with treatment responsibility from six regional pediatric oncology centers.
Efficient MDTM structures are influenced by a number of factors such as case selection, access to relevant information, technical equipment, participation from qualified experts, defined roles and responsibilities, leadership and teamwork, patient-centered care, and coordination of post-MDTM work. 10 Despite general agreement on the characteristics of an effective MDTM, teams show considerable variability related to, for example, organization, case selection, and decision-making processes.11,12 This variability and different cultures and traditions can be expected to be particularly challenging when MDTM teams in different geographical locations are brought together as virtual teams in national networks, which is the case in the newly established MDTMs for rare cancers in Swedish healthcare. We hypothesized that video-based meetings may challenge participants’ contributions to the case discussions. We, therefore, investigated participants’ experiences from virtual national MDTMs and assessed how different health professionals contributed the discussions and to what degree various disease-related and patient-related aspects were covered in the case discussions.
Materials and methods
Study design
With a focus on national virtual MDTMs for rare cancers, this study investigates health professionals’ views using an electronic questionnaire and through observational assessment evaluates MDTM function and participants’ contributions to the case discussions.
Setting
In Sweden, treatment for several rare cancers was centralized during 2015–2017 to two to four treatment centers. The type of treatment centralized was defined for each cancer type, but, in general, involved curative surgical and/or oncological treatment. Patients with palliative needs should, as far as possible, be treated in their local or regional hospitals, but should still be discussed at the relevant national MDTM at the time of diagnosis and when otherwise relevant for treatment recommendations. Case discussions should, according to the national standards of cancer care, be performed at the time of primary diagnosis and at the time of potential recurrence. These standards also define participating health expertise, which for anal cancer include surgeon, oncologist, radiologist, nuclear therapist, coordinator, contact nurse, and, when relevant, pathologist. The MDTMs are connected through a national video-conferencing platform. Members of the national expert teams are default participants, and responsible clinicians in regional hospitals may participate for select cases for which they are responsible or have referred. The leadership rests with the responsible physicians, which for the MDTMs included surgeons or oncologists. The national MDTM is coordinated from one of the national treatment centers, with annual rotating leadership among the two to four centers responsible. Sweden does not yet have a national formally implemented system for follow-up or evaluation of MDTMs.
Participants
All national MDTM teams for rare cancers in Sweden were eligble for the study. These included MDTMs for penile cancer, anal cancer, vulvar cancer, childhood cancer, cytoreductive surgery, advanced esophageal cancer, and hepatobiliary cancer. The latter MDTMs were grouped in the analyses motivated by a high degree of overlapping participants.
Questionnaire
Participants in the national MDTMs received a link by email to an online, SurveyMonkey-based, questionnaire designed by the study group. Two reminders were sent. Data were collected between May 2017 and May 2018. The responders were asked to rate 14 aspects of the national MDTM they participated in on a 7-point Likert-type scale (7 corresponded to fully agree and 1 to disagree). The questionnaire was distributed to 241 participants in MDTMs for penile cancer (n = 33), anal cancer (n = 30), vulvar cancer (n = 26), childhood cancer (n = 53), cytoreductive surgery (n = 12), and advanced esophageal and hepatobiliary cancer (n = 87). In total, 125 (52%) health professionals responded and included 45% women with 38% of the responders being above the age of 50. Among the respondents, physicians accounted for 87%, nurses for 11%, and medical secretaries for 2%. The respondents’ disciplines were surgery (56%), medicine/oncology (26%), pediatric oncology (10%), radiology (6%), and pathology (2%).
Observations
In the observational part of the study, members of the study group used observational evaluation tools. Motivated by well-established meeting structures, weekly MDTMs, and sufficient patient volumes, the MDTMs for penile cancer, anal cancer, and vulvar cancer were selected for this part of the study. The MDTM for penile cancer had participation from the two national centers, lasted a mean of 30 min, had a mean of 19 (15–22) participants, and discussed a mean of 11 (10–14) cases. The MDTM for anal cancer had four participating centers, lasted 40 min, had a mean of 21 (18–25) participants, and discussed a mean of 5 (4–6) cases. The MDTM for vulvar cancer had four participating centers, lasted 40 min, had a mean of 20 (15–25) participants, and discussed a mean of 6 (6) cases. Each MDTM was observed at three distinct occasions with participation from two study group members (M.N., B.O., J.W., and N.A. who are MDs) to a total of six observations for each MDTM. The observers independently rated the national MDTMs using the standardized observational tools: Meeting Observational Tool (MDT-MOT) and Metric of Decision-Making (MDT-MODe).13,14 MDT-MOT assesses overall meeting performance to support team development based on evaluation of 10 key domains including attendance, leadership and chairing, teamwork and culture, personal development and training, physical environment, technology and equipment, organization and administration, post-meeting coordination, patient-centered care, and clinical decision-making processes. These domains are evaluated using a 5-point Likert-type scale in which 5 implies optimal function and 1 implies insufficient function. 13 MDT-MODe evaluates the MDTM based on individual assessment of each case discussion using a 5-point Likert-type scare in which 5 implies optimal function and 1 implies insufficient function. 14 MDT-MODe is divided into two categories: availability of information (case history, patients’ view, psychosocial aspects, comorbidity, radiological, and pathological information) and paticipants’ (including chair, surgeons, physiotherapist, oncologists, radiologists, pathologists, nurses, and MDTM coordinators) contributions to the case discussions. 15 Prior to scoring, the observers read relevant publications and received oral information about the tools. Data using the MDT-MOT were collected from nine MDTMs, and data using the MDT-MODe were based on 67 case discussions.
Ethics
All data were handled anonymously and are presented at group level. The study was ethically reviewed and granted permission by the regional ethics committee at Lund University (registration number: 2016/195).
Statistical analysis
Participants’ response profiles based on Likert-type scale data and overall data from the instruments MDT-MOT and MDT-MODe are presented as diverging stacked bar charts. Data from MDT-MOT and MDT-MODe were analyzed for inter-observer variability using correlation coefficient estimates. For MDT-MOT, the total meeting score from each partipant was used. For MDT-MODe, inter-observer variability was estimated for each aspect based on all cases rated, followed by a total estimate of inter-observer variability for the tool as a whole. The mean score from the two observers for each aspect were evaluated and used in further analyses, which motivates use of 0.5 intervals in the stacked bar charts. Statistical analyses were performed in R version 3.2.2.
Results
Evaluation of participants’ views
The response profiles from the 125 participants in the six national Swedish MDTMs for rare cancers are presented in Figure 1. Strongly affirmative scores (5–7) related to my role at the MDTM is clear (85%), MDTM develops team competence (81%), and MDTM develops individual competence (80%). The statements that received the lowest degree of agreement (scores 1–3) were guidelines for documentation of treatment recommendations are clear (20%), technology is well-functioning (22%), and we evaluate working with the MDTM (30%).

Participants’ (n = 125) views on structure and function of six national virtual MDTMs in cancer care.
Observational assessment
MDT-MOT is based on six observations from each diagnosis, whereas MDT-MODe is based on the total number of cases in the total number of case discussions observed, which was 68 for penile cancer, 30 for anal cancer, and 36 for vulvar cancer. The mean scores from MDT-MOT and MDT-MODe observations were used in the further analyses. Inter-observer correlations were 0.71 for MDT-MOT and of 0.86 for MDT-MODe. MDT-MOT evaluates the MDTM as a whole. High scores were obtained for clinical decision-making processes, teamworking and culture, technology and equipment, physical environment, and leadership and chairing. Low scores applied to patient-centered care, organization, administration, and post-meeting coordination (Figure 2, Supplementary Table 1).
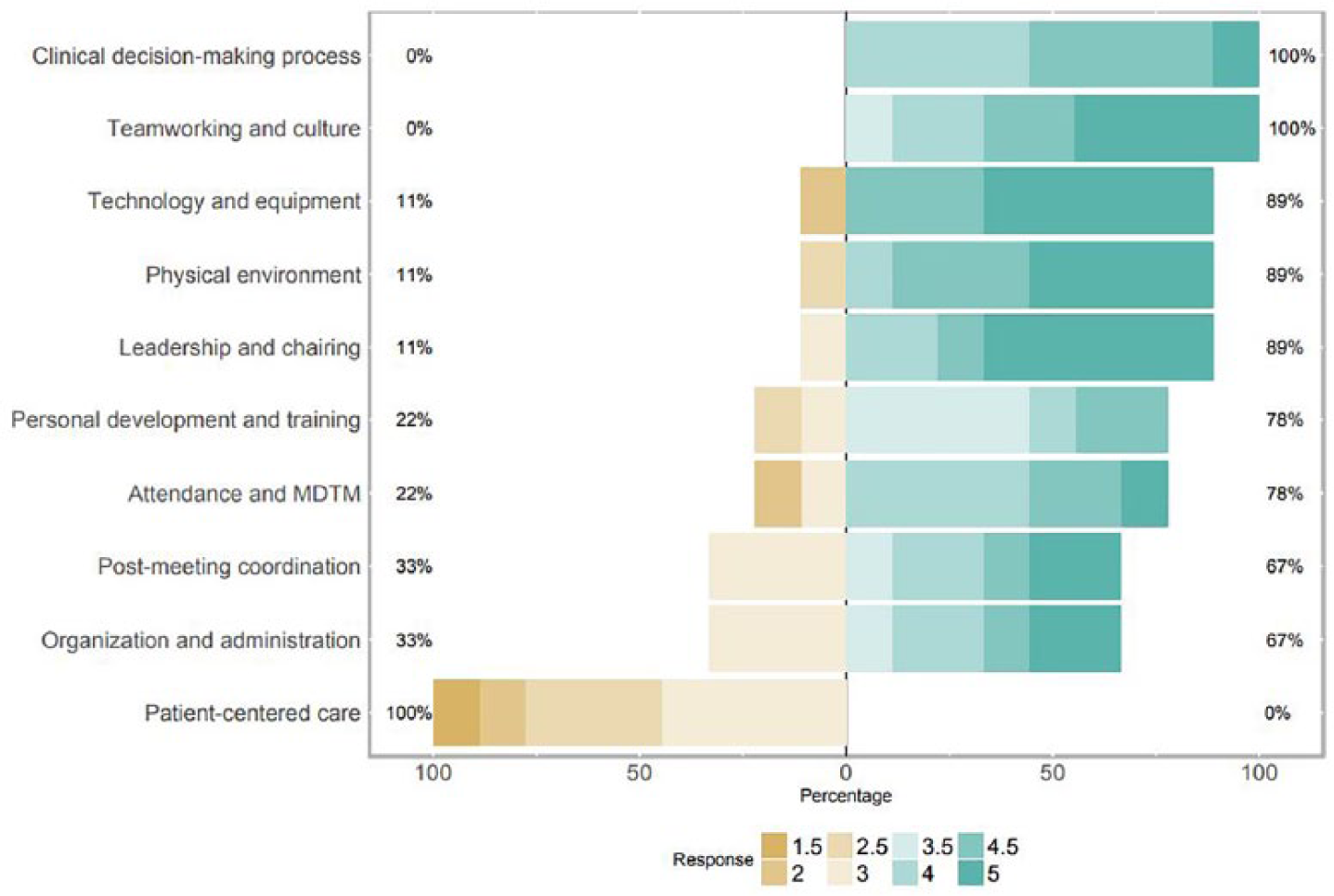
Observational assessment data based on MDT-MOT.
MDT-MODe evaluates each case discussion and considers availability of information and paticipants’ contributions to the case discussions. Case information and case discussions by the chair, surgeons, and oncologists scored high, whereas lower scores applied to radiologists, pathologists, nurses, physiotherapists, and MDTM coordinators (Figure 3, Supplementary Table 1). Low scores applied to information on psychosocial aspects and patients’ views.

Observational assessment data based on MDT-MODe. Stacked-bar chart showing the results from the MDTMs for anal cancer, penile cancer, and vulvar cancer. Evaluation of (a) information and (b) contribution to the discussion. The MDT-MODe tool assesses quality of presented information and participants’ contribution to the case discussion using a 5-point scale.
Comparison between participants’ views and observational tools
Based on questionnaire data, MDTM participants reported high scores, for example, development of team competence (81%), development of individual competence (80%), clear MDTM goals (78%), involvement in case discussions (78%), and well-functioning leadership (77%), which was in agreement with the results from the observational tools that showed favorable scores for leadership and charing, teamwork and culture, and personal development and training (Figures 1–3). The observational tools, however, discriminated contributions from the different disciplines with high scores for participation from surgeons and oncologists and lower scores for radiologists and pathologists. Based on the MDT-MODe, contributions from nurses, physiotherapists and MDTM coordinators received low scores.
Both observational tools suggested weak consideration of patient-related aspects such as patients’ preferences, comorbidity, and psychosocial aspects, which stand in contrast to the responses from the MDTM participants with 79% providing affirmative responses to consideration of comorbidity and 71% reporting to consider patients’ perspectives. Better outcome based on observations than questionnaire data applied to functionality of technology and equipment that was rated high using observational tools, whereas affirmative scores (5–7) for technical functionality were given by 63% of the participants.
Discussion
Main findings
National virtual MDTMs for rare cancers have, during recent years, been implemented in Swedish cancer care. Our data suggest that case information, leadership, and teamwork are overall well-functioning, whereas contributions from nurses, physictherapists and coordinators to the case discussions and considerations of patients’ perspectives are limited (Figures 1–3). In Sweden, the medical teams responsible for establishing national MDTMs had access to updated national standards of care and a video-based communication platform, but otherwise implemented these virtual MDTMs independently and without formalized leadership training, improvement programs, or structured evaluation plans.
Several instruments have been developed to assess and improve MDTM function, but there are no generally agreed measures or principles for MDTM evaluations. Available instruments include checklists (Multidisciplinary Team Quality Improvement Checklist (MDT-QuIC)), observation tools (Multidisciplinary Team Observational Assessment Rating Scale (MDT-OARS), MDT-MODe, MDT-MOT, and a tumor leadership assessment instrument (ATLAS)), and self-assessment instruments (Team Evaluation and ASSESSment Measure (TEAM) and Multidisciplinary Team Feedback for Improving Teamworking (MDT-FIT)).6,14,16,17 Our application of MDT-MOT and MDT-MODe was motivated by the wish to use two comparable instruments with somewhat different focus, that is, on overall function of the MDTM versus evaluation of the individual case discussions. The focus on the quality of information, the contributions to the case discussions, and the overall functionality of the meetings provide a basis for future team-led improvement programs. We demonstrate high inter-observer correlation and observations that are largely in agreement between the two observational assessment tools applied (Figures 2 and 3). MDT-MOT and MDT-MODe have been applied to MDTMs for different diagnoses.18–21 Our double readings resulted in inter-observer variabilities of 0.71 for MDT-MOT and 0.86 for MDT-MODe, which fit well with the findings from Gandamihardja et al., 19 who applied the MDT-MODe to MDTM for breast cancer with reliability coefficients of 0.73–0.93.
Studies on virtual MDTMs are rare, but experiences from regional MDTMs that connect specialists and community physicians in a geographical area demonstrate general satisfaction and suggest that virtual MDTMs are feasible and valuable.4,22 Development of individual- and team competence were two of the top-rated benefits among participants in national MDTMs (Figure 1). This suggests a potential to strengthen national professional networks, increase collaboration across geographical regions, support further education, and stimulate knowledge sharing, which has been documented in regional MDTMs.4,23,24 Access to relevant information and good teamwork with representation from all core disciplines have been identified as major determinants for reaching treatment recommendations at MDTMs.15,19,20,25 We did not observe difficulties in reaching joint treatment recommendations, which may partly be explained by the large expert network available, well-functioning leadership, and relatively few cases per MDTM with a mean of 3–8 min per case discussion.
The national Swedish MDTMs are planned for rotating leadership on an annual basis. Most MDTMs are led by surgeons, but rotating leadership that involves various disciplines and professions, for example, oncologists and specialist nurses, may be relevant to consider since experiences from other MDTMs suggest that this principle may improve teamwork and reduce potential conflicts.25,26 Formalized MDTM structures, definition of goals, and follow-up on implementation of treatment recommendations represent future focus areas. 4 Initiatives such as regular performance review, self-assessment and feedback, and e-based team training have proven effective and would likely be relevant and feasible also for national geographically disparate teams. 20
Biomedical elements have, in several MDTM settings, been shown to be better covered than psychosocial aspects, information on comorbidity, and patients’ views.13,19,27–29 A patient-centered approach is considered to be an important basis for individualized treatment recommendations14,23,24,30, and consideration of psychosocial aspects, comorbidities, and patients’ autonomy are recognized as pillars for an effective MDTM.28,31 Data based on participants’ ratings and data from our observations did, in this regard, differ with 71%–79% affirmative response among participants related to comorbidity and patients’ perspectives, whereas observations rated consideration of patient-related perspectives low (Figures 1–3). Jalil et al. 18 used the MDT-MODe tool to evaluate MDTMs for various cancer types, including urological, gastrointestinal, and head and neck cancers and reported scores comparable to ours for comorbidity (mean 2.6 vs 2.1), psychosocial considerations (1.5 vs 1.4), and patient view (1.6 vs 1.3). National MDTMs gather expertise that may be geographically far from the patient, which further underscores the need to ensure development of structures to grant consideration of patient perspectives.23,31 Furthermore, focus on patients’ preferences, performance status and comorbidities has been shown to positively influence implementation of MDTM recommendations.15,27 MDT-MODe suggested low contribution to the case discussions from nurses, physiotherapists, and MDTM coordinators with scores of 1.0–1.2 (Supplementary Table 1). This observation is supported by other studies, several of which have also applied MDT-MODe.14,15,19,20,24,29 This shortcoming likely reflects the dominance of medical aspects over patient-related aspects in the case discussions. A weak focus on rehabilitation perspectives at MDTMs has been reported from the United Kingdom.15,29,31–33 Based on the National Ewing Sarcoma MDTM in the United Kingdom, Bate et al. 32 have documented that patients feel that their views should inform the decision-making process and recommend initiatives such as treatment recommendations written in plain language and development of tools to improve patient involvement and enhance communication. Soukup et al. 25 demonstrated that a complete patient profile and contributions to the case review by all core disciplines drive the decision-making process at MDTMs. Our observations suggest that the national MDTM teams should discuss and consider how to grant an optimal balance between biomedical facts and patient-related aspects.23–25 Development of standards for how patient perspectives are granted consideration would be relevant. Such a development will likely require consideration of the current meeting format and should involve care professionals who may represent patients’ perspectives at the MDTM.
Since national MDTMs are resource demanding and require significant coordination, initiatives that grant safe and easy access to relevant information, skilled participants, well-functioning teamwork, good leadership, and efficient administrative routines are crucial.1,2,6,15 The extended number of participants from various hospitals with different routines and traditions adds a level of complexity to national MDTMs. Though overall feasible, a number of issues should be considered prior to initiation of a national MDTM for best possible outcome. These include infrastructure and technology, referral principles, requirements for participants, running principles, responsibilities for communicating recommendations, and principles for governance and evaluation of national MDTMs. Based on our experiences and observations, and on current literature, we summarized issues to consider into guidelines for virtual national MDTMs in cancer care (Table 1).
Guidelines for establishing and running a national virtual multidisciplinary team meeting.

MDTM: multidisciplinary team meeting; IT: information technology.
Strengths and limitations
We aimed to obtain a comprehensive picture rather than to perform detailed evaluations of the independent MDTMs. The combination of team members’ subjective views and objective evaluation based on observational tools represent strengths and allow for identification of areas of agreement as well as disagreement between the different measures. The concordant picture obtained for most factors and areas supports identification of relevant benefits and shortcomings. We regard a Hawthorne effect as less likely since the observers were present at one participating hospital, whereas the majority of the participants participated by video from other hospitals. Limitations include a response rate of 52% for the electronic questionnaire and observations limited to three MDTM sessions for each diagnosis. Though the observers documented good inter-observer agreement between the MDT-MODe and the MDT-MOT, the tools were new to the study group, and the evaluators may still be in the learning curve. Furthermore, the tools do not allow for scoring of individual specialists and do not account for cases where, for example, histopathological input was not considered relevant. The low scores for the contribution from nurses, physiotherapists, and MDTM coordinators may not fully reflect a suboptimal involvement, for example, limited involvement from nurses could reflect clinical trajectories where cases are discussed at the MDTM prior to being seen by the responsible nurse. Due to a limited number of answers from nurses and coordinators, subgroup analysis was not possible.
Conclusion
National virtual MDTMs for rare cancer type have successfully been established in Swedish cancer care. Evaluation based on participants’ views and structured observational assessment identified well-functioning leadership and teamwork, but revealed weaknesses related to patient perspectives, involvement of care professionals, and MDTM evaluation principles. To make best use of the expert networks involved in national MDTMs and to provide appropriate and acceptable treatment recommendations for patients with rare cancer type, we suggest that team review and MDTM evaluation should be prioritized with a specific focus on how patient perspectives and contributions from care personnel may be strengthened.
Supplemental Material
Rosell-supplementary_table_1-190204 – Supplemental material for Function, information, and contributions: An evaluation of national multidisciplinary team meetings for rare cancers
Supplemental material, Rosell-supplementary_table_1-190204 for Function, information, and contributions: An evaluation of national multidisciplinary team meetings for rare cancers by Linn Rosell, Jessica Wihl, Oskar Hagberg, Björn Ohlsson and Mef Nilbert in Rare Tumors
Supplemental Material
S_SV__VB__Page_proof_for__Rare_Tumors_-_RTU_841696 – Supplemental material for Function, information, and contributions: An evaluation of national multidisciplinary team meetings for rare cancers
Supplemental material, S_SV__VB__Page_proof_for__Rare_Tumors_-_RTU_841696 for Function, information, and contributions: An evaluation of national multidisciplinary team meetings for rare cancers by Linn Rosell, Jessica Wihl, Oskar Hagberg, Björn Ohlsson and Mef Nilbert in Rare Tumors
Footnotes
Acknowledgements
The authors would like to acknowledge Nathalie Alexandersson and Annika Wendt-Wesén for help with collecting data and the Regional Cancer Center South for support in research around MDTM perspectives. Authors also thank T. Soukup for generously sharing information on and accesss to the observational tools used.
Author contributions
All authors have relevantly contributed to the manuscript and approved of the final version and its submission.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was ethically reviewed and granted permission by the regional ethics committee at Lund University (registration number 2016/195).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Swedish Cancer Society, the ALF research funds, and the FOUU funds in Region Skåne.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.